
TL;DR: Hyperbaric oxygen therapy (HBOT) is one of the most evidence-supported adjunctive treatments for diabetic foot ulcers and chronic wounds. A 2025 network meta-analysis of 99 randomised controlled trials (7,356 patients) found HBOT significantly reduced major amputation risk (OR 0.35, 95% CI 0.16-0.78). A separate 2025 meta-analysis (Zhang et al., Int J Burn Trauma) likewise reported a substantial reduction in amputation rates with systemic HBOT, though its pooled estimate carried a reported confidence interval that was statistically implausible, so the magnitude should be interpreted with caution. For referring physicians, the clinical evidence supports early referral for patients with non-healing diabetic wounds, particularly those at risk of limb loss.
What Does the Latest Research Say About HBOT for Wound Healing?
Hyperbaric oxygen therapy (HBOT) is an adjunctive treatment in which patients breathe 100% oxygen at pressures greater than 1 atmosphere absolute (ATA), typically 2.0-2.4 ATA, inside a pressurised chamber. For chronic wound management, HBOT enhances tissue oxygenation, promotes angiogenesis, reduces oedema, and supports collagen synthesis in hypoxic wound beds. The Undersea and Hyperbaric Medical Society (UHMS) lists several wound-related indications among the 15 conditions on its current UHMS Indications list (15th Edition, 2024), including diabetic foot ulcers meeting specific Wagner grade criteria.
The past two years have produced a remarkable volume of high-quality systematic reviews and meta-analyses examining HBOT for wound healing. This article synthesises the most current evidence from 2024-2026 to help referring physicians make informed decisions about when and how to refer patients with non-healing wounds to hospitals and regulated facilities offering hyperbaric medicine in Canada.
How Effective Is HBOT for Diabetic Foot Ulcers?
Diabetic foot ulcers (DFUs) affect an estimated 15-25% of patients with diabetes mellitus during their lifetime. When standard wound care fails, the risk of major amputation escalates dramatically. HBOT has been studied extensively as an adjunctive therapy for DFUs, and the recent evidence is compelling.
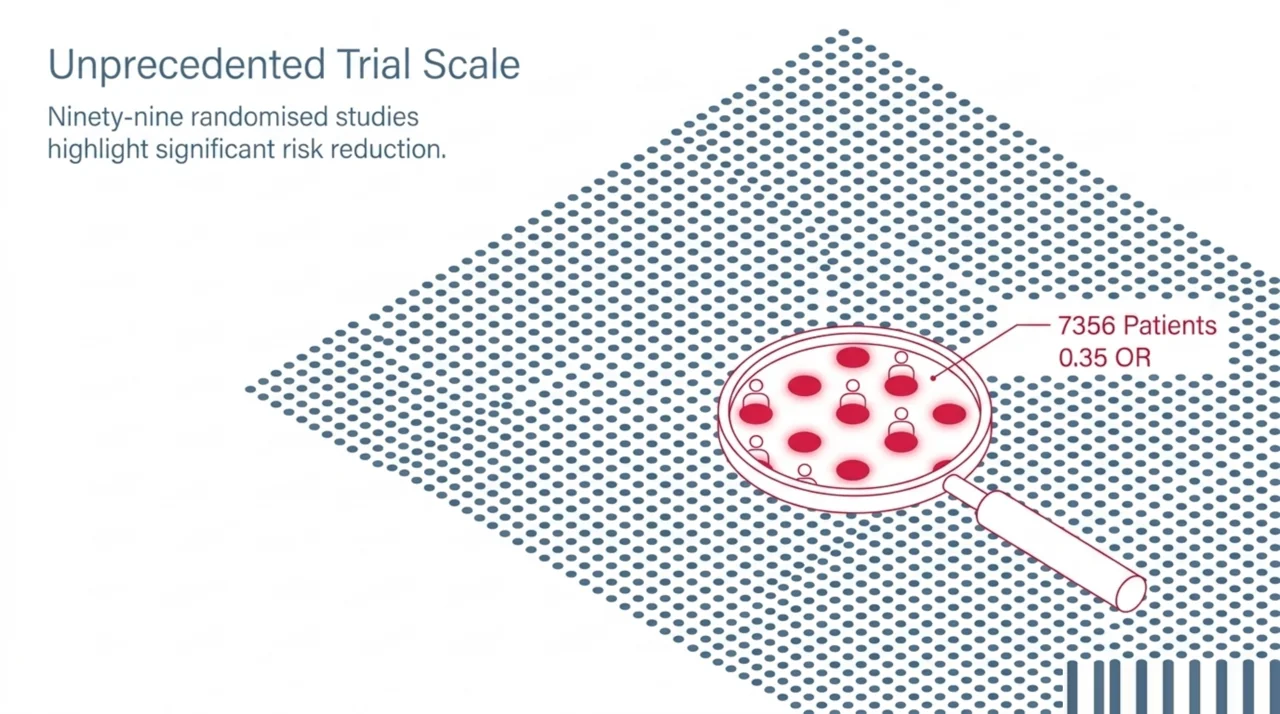
A landmark 2025 network meta-analysis published in PeerJ compared 12 different interventions for DFU across 99 randomised controlled trials involving 7,356 patients (DOI: 10.7717/peerj.19809). HBOT demonstrated a statistically significant reduction in amputation risk compared to standard of care (OR 0.35, 95% CI 0.16-0.78). While stem cell therapy ranked highest for amputation prevention overall (OR 0.12), HBOT was the only widely available, non-experimental therapy to achieve significance in this critical outcome. For wound healing rates, HBOT was associated with significantly improved healing compared to standard care.
A separate 2025 meta-analysis in the International Journal of Burns and Trauma (DOI: 10.62347/WVEM7973) evaluated systemic HBOT, negative pressure wound therapy (NPWT), platelet-rich plasma (PRP), and vacuum-assisted closure for DFUs. The results were notable: systemic HBOT was associated with a significant reduction in amputation rates. NPWT showed the strongest results for ulcer closure and healing time reduction, while HBOT’s primary advantage centred on limb preservation.
Key Outcome Data From Recent Systematic Reviews
| Study (Year) | Design | Patients | Key HBOT Finding |
|---|---|---|---|
| Hu et al. (2025), PeerJ | NMA, 99 RCTs | 7,356 | Amputation OR 0.35 (95% CI 0.16-0.78) |
| Zhang et al. (2025), Int J Burns Trauma | SR + MA, 10 studies | N/R | Significant reduction in amputation risk |
| Damineni et al. (2025), Cureus | SR, 6 studies | 391 | Reduced major amputation, improved healing rates |
| Apolo-Arenas et al. (2024), Int J Vasc Med | SR, 7 studies | N/R | Significant improvement vs standard care for DFU |
| Du et al. (2024), Adv Skin Wound Care | MA, 31 RCTs | N/R | Amputation RR 0.529 (95% CI 0.325-0.862) |
Does HBOT Reduce the Risk of Amputation in Diabetic Patients?
The strongest and most consistent finding across the recent literature is HBOT’s role in amputation prevention. This is arguably the most clinically meaningful outcome for referring physicians to consider.
The 2025 systematic review published in Cureus (DOI: 10.7759/cureus.78655) analysed six studies encompassing 391 patients. The majority of included studies demonstrated that HBOT, when added to standard wound care, led to reduced rates of major amputation, improved ulcer healing, and decreased ulcer size and depth compared to standard care alone. The authors noted that while one study found no significant differences in long-term outcomes, the overall evidence favoured HBOT as an adjunctive therapy.
A 2024 systematic review in the International Journal of Vascular Medicine (DOI: 10.1155/ijvm/8450783) specifically examined HBOT for amputation prevention in chronic diabetic foot. Most included studies showed positive results for wound healing and amputation prevention compared to standard care alone. The reviewers concluded that hyperbaric chamber use combined with standard care is “favourable in patients with chronic DFUs” and showed “promising and positive results for wound healing in DFU and the prevention of amputations.”
These findings align with the 2024 meta-analysis of 31 randomised controlled trials by Du et al. (DOI: 10.1097/ASW.0000000000000131), which found that patients receiving oxygen-based therapies (including HBOT) had significantly lower amputation rates (RR 0.529, 95% CI 0.325-0.862), better short-term wound healing (RR 1.544), greater percentage reduction in ulcer area, shorter healing times, and higher post-treatment transcutaneous oxygen pressure (TcPO2) values.
What Are the Mechanisms Behind HBOT’s Wound Healing Effects?
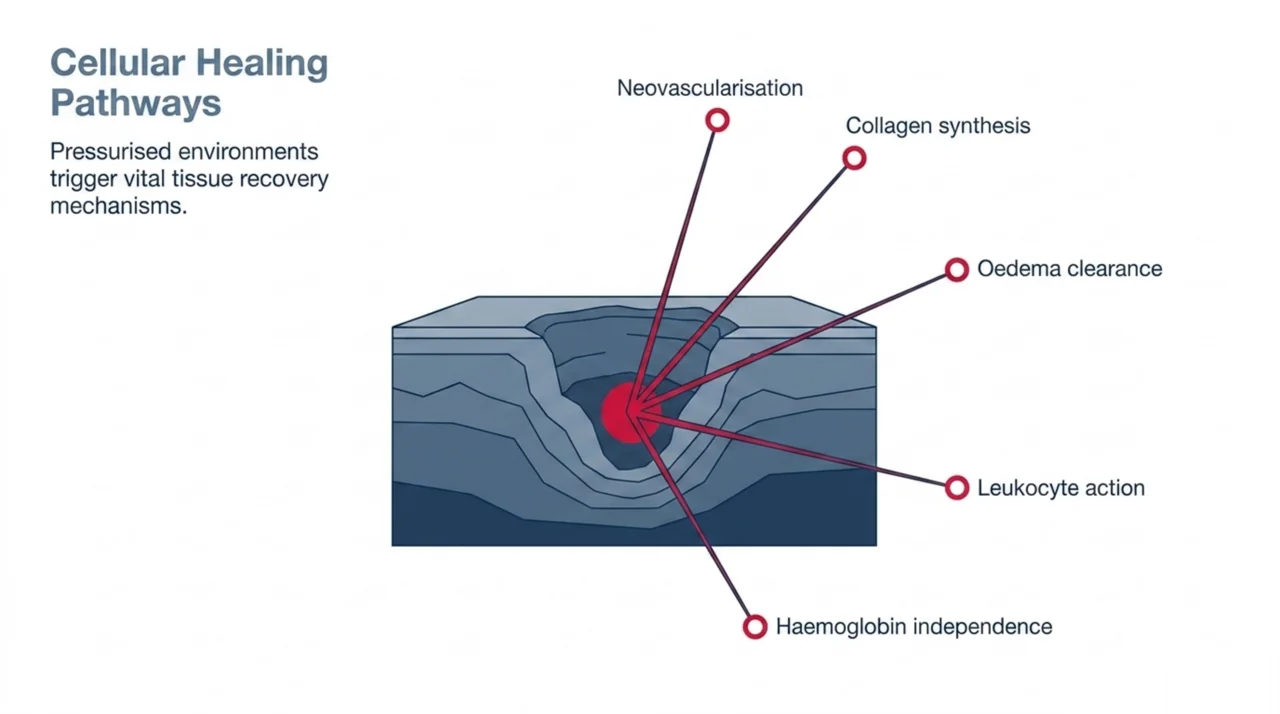
Understanding the physiological basis for HBOT in wound healing helps physicians identify which patients are most likely to benefit. HBOT’s therapeutic mechanisms in chronic wounds operate through several interconnected pathways:
- Enhanced tissue oxygenation: HBOT increases dissolved plasma oxygen concentrations by 10-15 times normal levels, delivering oxygen to hypoxic wound beds independent of haemoglobin. This is particularly relevant in diabetic microangiopathy where capillary perfusion is compromised.
- Neovascularisation: Repeated hyperbaric exposures stimulate vascular endothelial growth factor (VEGF) production and angiogenesis. The 2026 systematic review by Astasio-Picado et al. specifically noted HBOT’s “beneficial effects on angiogenesis” as a distinguishing mechanism (DOI: 10.3390/medicina62010109).
- Collagen synthesis support: Oxygen-dependent hydroxylation of proline and lysine is essential for collagen cross-linking. HBOT provides the supraphysiological oxygen tension needed to support this process in hypoxic tissues.
- Infection control: Elevated tissue oxygen pressures enhance leukocyte bacterial killing through oxidative burst pathways. HBOT also potentiates the effectiveness of certain antibiotics, including aminoglycosides and fluoroquinolones.
- Oedema reduction: Hyperoxia causes vasoconstriction in well-perfused tissues while simultaneously increasing oxygen delivery, resulting in reduced oedema without compromising tissue oxygenation.
How Does HBOT Compare to Other Advanced Wound Therapies?
Referring physicians increasingly face the question of which adjunctive therapy to recommend when standard wound care fails. The 2025 network meta-analysis by Hu et al. provides the most comprehensive head-to-head comparison available. Across the 12 interventions studied, the rankings varied by outcome measure:
| Outcome | Top Ranked | HBOT Ranking | HBOT Performance |
|---|---|---|---|
| Healing rate | Stem cells (SUCRA 89.7%) | Mid-range | Improved vs standard care |
| Healing time | Amniotic membrane (SUCRA 84.7%) | Lower-mid | Not significantly faster |
| Wound area reduction | Low-level laser (SUCRA 93.9%) | Lower-mid | Modest reduction |
| Amputation prevention | Stem cells (SUCRA 79.9%) | 2nd tier | OR 0.35 – significant |
This ranking underscores an important clinical nuance: HBOT’s primary advantage lies in limb salvage, not wound closure speed. For patients where the primary clinical concern is preventing major amputation, HBOT remains one of the most effective available interventions. For patients where rapid wound closure is the priority and amputation risk is low, other therapies such as NPWT or PRP may offer faster results.
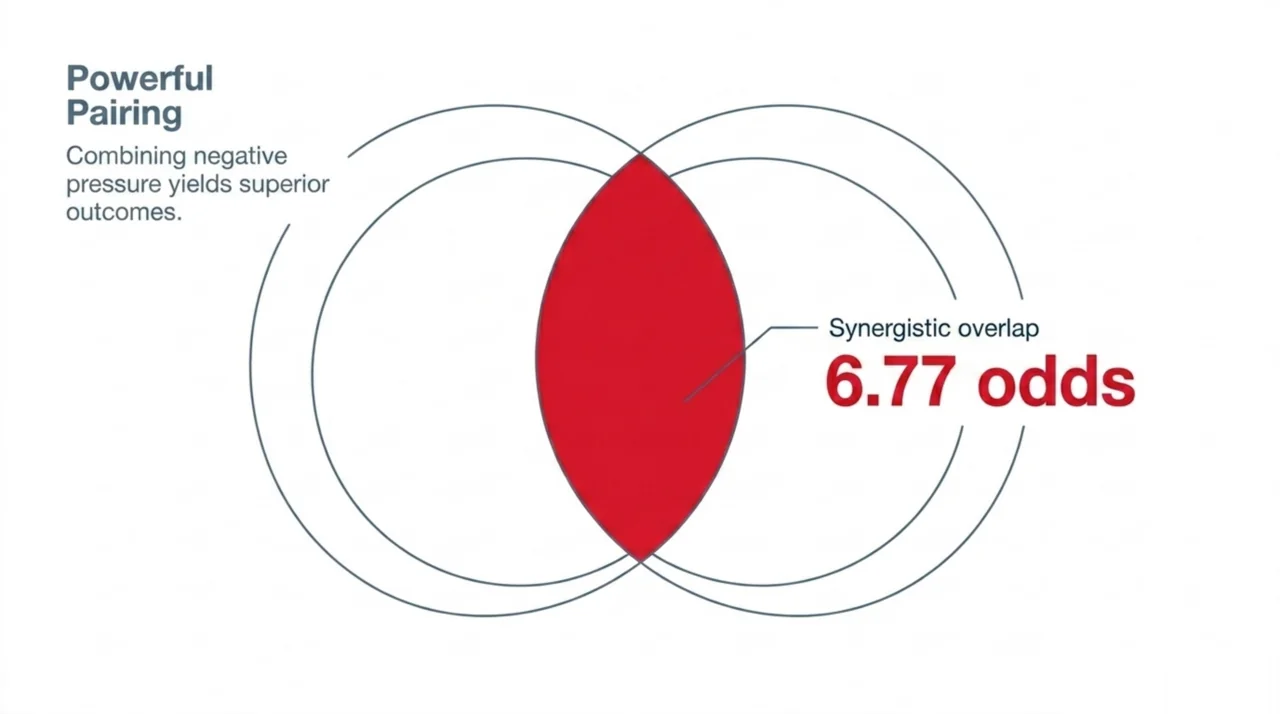
A 2024 meta-analysis on combined NPWT and HBOT found that using both therapies together produced significantly better outcomes than NPWT alone, with a wound healing odds ratio of 6.77 (95% CI 3.53-12.98). This suggests that combination approaches may offer the best results for complex cases.
Which Patients Should Physicians Refer for Hyperbaric Wound Treatment?
Based on the current evidence, the following patient profiles represent the strongest candidates for HBOT referral in the context of wound management:
- Wagner Grade 3-4 diabetic foot ulcers that have failed to respond to at least 30 days of standard wound care, including offloading, debridement, infection management, and glycaemic optimisation.
- Patients at imminent risk of major amputation where limb salvage is the primary clinical goal. The evidence for amputation prevention is the strongest outcome across all recent reviews.
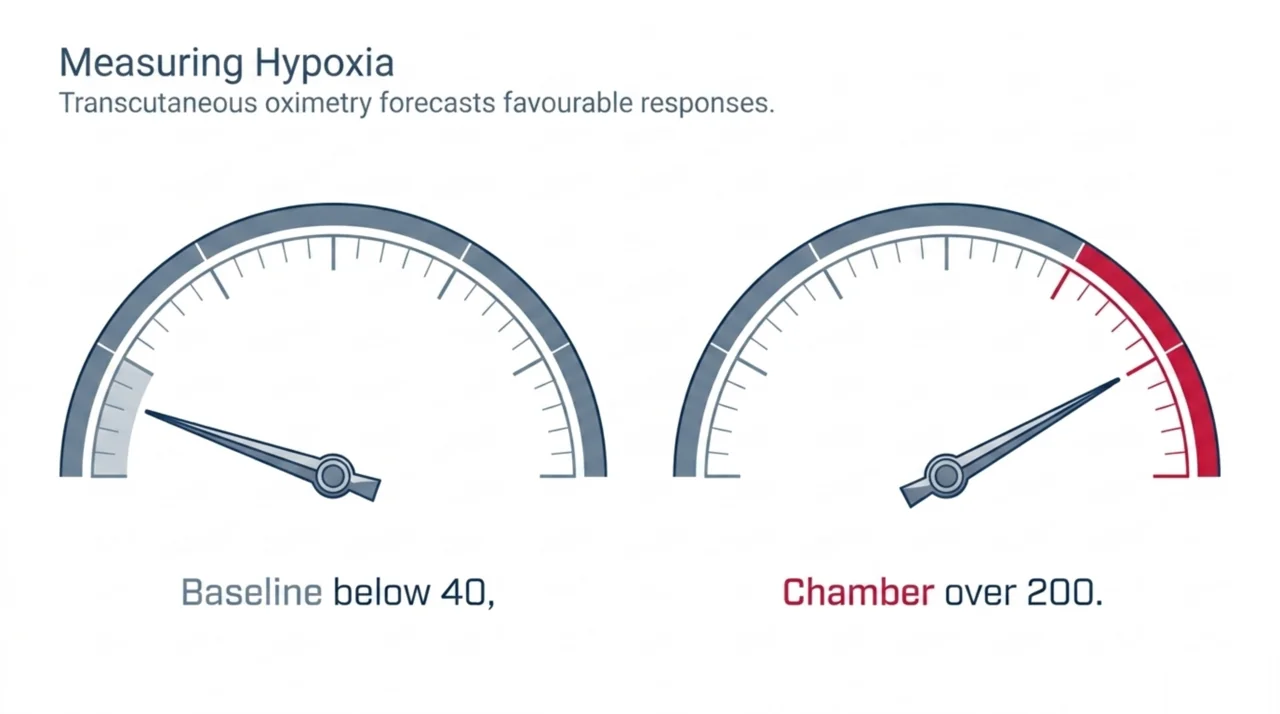
- Patients with compromised tissue oxygenation confirmed by transcutaneous oximetry (TcPO2). A baseline TcPO2 below 40 mmHg at the periwound area, with an increase to above 200 mmHg during an in-chamber hyperbaric oxygen challenge, suggests the patient will respond to HBOT.
- Post-surgical patients with compromised grafts or flaps where tissue viability is threatened by hypoxia.
- Patients with chronic wounds complicated by osteomyelitis where HBOT can enhance antibiotic penetration and leukocyte function.
Contraindications to Screen For
Before referring, physicians should screen for absolute and relative contraindications. Untreated pneumothorax is the only absolute contraindication. Relative contraindications include uncontrolled seizure disorders, severe congestive heart failure, active malignancy undergoing certain chemotherapy regimens, and claustrophobia. Patients on bleomycin or cisplatin should be discussed with the hyperbaric medicine team. For a complete screening guide, see the approved conditions and contraindications resource on Canada Hyperbarics.
How Can Canadian Physicians Refer Patients for HBOT?
The referral process for hyperbaric oxygen therapy varies by province. In provinces with publicly funded programmes, HBOT for recognised indications can be accessed through hospital-based hyperbaric units. In provinces without public coverage, patients may access treatment through private clinics, often with support from extended health insurance benefits.
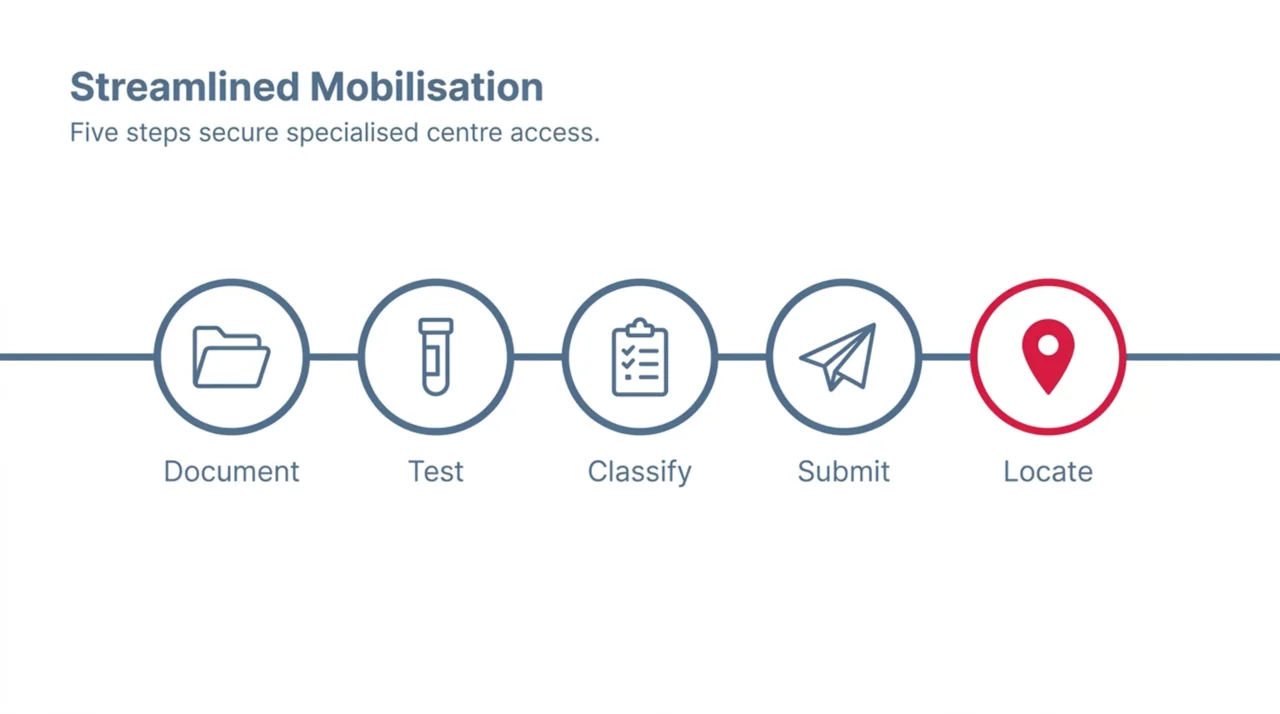
Key steps for referring physicians in Canada:
- Document treatment failure: Record at least 30 days of standard wound care with measurable outcomes showing inadequate healing progress.
- Obtain TcPO2 measurement: If available, baseline and in-chamber transcutaneous oximetry results strengthen the referral and help predict treatment response.
- Classify wound severity: Use the Wagner classification system. HBOT is most strongly indicated for Wagner Grade 3 and above.
- Complete the referral: Include wound photographs, relevant lab work (HbA1c, vascular assessment results), treatment history, and comorbidity summary.
- Locate a facility: The Canada Hyperbarics facilities directory lists hospitals and regulated facilities across the country. Facilities accredited by the Canadian Undersea and Hyperbaric Medical Association (CUHMA) meet national safety and quality standards.
Canada Hyperbarics maintains a comprehensive research database with over 14,400 studies searchable by condition, which physicians can use to review the evidence base for specific clinical scenarios. The coverage guide provides province-by-province details on public health insurance coverage for HBOT.
What Are the Limitations of the Current Evidence?
While the recent evidence strongly supports HBOT for DFU management, referring physicians should be aware of several limitations identified across the reviewed studies:
- Heterogeneity in protocols: Included studies used varying pressures (2.0-2.5 ATA), session durations (60-120 minutes), and total treatment sessions (20-40+). No standardised protocol has been universally adopted.
- Methodological concerns: The 2025 Cureus review noted moderate-to-high risk of bias in several key domains, including performance bias from insufficient blinding. Blinding in HBOT trials is inherently challenging due to the physical nature of treatment.
- Long-term outcomes: The 2024 meta-analysis by Du et al. found no statistically significant difference in long-term wound healing (RR 1.227, 95% CI 0.976-1.542), though short-term parameters were significantly improved.
- Selection bias: Observational studies included in several reviews were susceptible to inconsistent patient allocation, potentially distorting treatment comparisons.
- Standard care variability: The definition of “standard care” varied across studies, making direct comparisons difficult.
The evidence quality is improving, however. The inclusion of large network meta-analyses and the growing number of RCTs represent meaningful progress from the earlier evidence base, which relied more heavily on case series and retrospective analyses.
Frequently Asked Questions
What Wagner grade qualifies a diabetic foot ulcer for HBOT?
Most hyperbaric facilities and insurance programmes require Wagner Grade 3 or higher (deep ulcer with abscess or osteomyelitis) for HBOT referral. Some facilities accept Grade 2 ulcers that have failed standard care for 30 or more days. The UHMS guidelines specify that the wound must not have responded adequately to standard wound care before HBOT is initiated.
How many HBOT sessions are typically needed for wound healing?
Standard protocols call for 20-40 sessions at 2.0-2.4 ATA for 90-120 minutes per session, delivered daily five days per week. Clinical reassessment typically occurs after 20 sessions. If measurable improvement is documented, treatment may continue. If no improvement is observed, continuation is generally not recommended.
Is HBOT covered by provincial health insurance for wound care in Canada?
Coverage varies by province. In Ontario, OHIP covers HBOT for 14 recognised indications at both hospitals and eligible private clinics, including diabetic wound-related indications. In British Columbia, MSP coverage is limited to Vancouver General Hospital. Alberta covers HBOT through Alberta Health Services hospital clinics in Calgary and Edmonton. For other provinces, the Canada Hyperbarics coverage guide provides current details on each provincial health plan.
Can HBOT be combined with negative pressure wound therapy?
Yes, and the evidence supports this approach. A 2024 meta-analysis of 15 studies found that combining NPWT with HBOT produced significantly better wound healing rates (OR 6.77), reduced bacterial load (OR 0.16), shorter healing times, and reduced hospitalisation compared to NPWT alone. The two therapies address complementary mechanisms: NPWT manages exudate and promotes granulation, while HBOT enhances tissue oxygenation and angiogenesis.
What is the role of transcutaneous oximetry in HBOT referral?
Transcutaneous oxygen pressure (TcPO2) measurement is the most reliable predictor of HBOT response in wound patients. A periwound TcPO2 below 40 mmHg indicates tissue hypoxia. An in-chamber hyperbaric challenge showing TcPO2 rising above 200 mmHg suggests the wound will respond to HBOT. This test can help physicians identify patients who will benefit most, avoiding unnecessary treatment in patients unlikely to respond.
Does HBOT help with non-diabetic chronic wounds?
HBOT is approved for several non-diabetic wound types, including compromised surgical grafts and flaps, chronic refractory osteomyelitis, and delayed radiation tissue injury. The 2024 meta-analysis by Du et al., which included 31 RCTs covering various chronic wound types, found significant benefits for oxygen-based therapies across multiple wound aetiologies, not limited to diabetic ulcers.
What are the risks of HBOT for wound patients?
HBOT is generally well tolerated. The most common adverse effect is middle ear barotrauma; symptomatic cases requiring intervention occur in approximately 2-4% of patients and are typically mild. Other potential effects include transient myopia (reversible after treatment cessation), claustrophobia, and rarely, oxygen toxicity seizures (estimated at less than 1 in 10,000 treatments). The 2026 systematic review by Astasio-Picado et al. noted that both HBOT and NPWT “presented significant advantages” with acceptable safety profiles.
Where can I find hyperbaric treatment centres in Canada?
The Canada Hyperbarics facilities directory lists hospitals and regulated facilities across every province. The directory includes CUHMA-accredited centres and provides contact information for referrals. Physicians can also contact the Canadian Undersea and Hyperbaric Medical Association (CUHMA) directly for guidance on locating appropriate facilities.
Clinical Takeaways for Referring Physicians
The 2024-2026 evidence base for HBOT in chronic wound management has grown substantially, driven by multiple large-scale systematic reviews and network meta-analyses. The key findings that should inform clinical decision-making include:
- Amputation prevention is HBOT’s strongest outcome: Across all recent reviews, HBOT consistently and significantly reduces major amputation risk in diabetic foot ulcer patients. This is the primary clinical indication for referral.
- Early referral matters: Patients referred after prolonged treatment failure may have less salvageable tissue. Consider HBOT referral after 30 days of inadequate healing with standard care, rather than waiting for imminent limb threat.
- Combination therapy shows promise: Combining HBOT with NPWT produces significantly better outcomes than either therapy alone. Multi-modal wound management should be discussed with the hyperbaric medicine team.
- Patient selection is critical: TcPO2 testing can help identify patients most likely to benefit. Not every chronic wound patient will respond to HBOT, and appropriate screening maximises treatment value.
- Limitations remain: Protocol standardisation and long-term outcome data are still needed. However, the current evidence supports HBOT as a valuable adjunctive therapy when standard care fails.
For physicians seeking more detailed evidence on specific wound types and conditions, the Canada Hyperbarics research library provides access to over 14,400 indexed studies with searchable filters by condition category.
References
- Astasio-Picado A, et al. Comparative Evidence on Negative Pressure Therapy and Hyperbaric Oxygen Therapy for Diabetic Foot Ulcers: A Systematic Review. Medicina (Kaunas). 2026;62(1):109. DOI: 10.3390/medicina62010109
- Hu X, et al. Comparison of the efficacy of 12 interventions in the treatment of diabetic foot ulcers: a network meta-analysis. PeerJ. 2025;13:e19809. DOI: 10.7717/peerj.19809
- Zhang Y, et al. A systematic review and meta-analysis of treatment modalities and their impact on the healing progression of diabetic foot ulcers. Int J Burns Trauma. 2025;15(2):41-52. DOI: 10.62347/WVEM7973
- Damineni U, et al. Clinical Outcomes of Hyperbaric Oxygen Therapy for Diabetic Foot Ulcers: A Systematic Review. Cureus. 2025;17(2):e78655. DOI: 10.7759/cureus.78655
- Apolo-Arenas MD, et al. Use of the Hyperbaric Chamber Versus Conventional Treatment for the Prevention of Amputation in Chronic Diabetic Foot. Int J Vasc Med. 2024;2024:8450783. DOI: 10.1155/ijvm/8450783
- Du X, et al. Effects of Oxygen Therapy on Patients with a Chronic Wound: A Systematic Review and Meta-analysis. Adv Skin Wound Care. 2024;37(5):1-9. DOI: 10.1097/ASW.0000000000000131
- Yang L, et al. Adjunctive hyperbaric oxygen therapy and negative pressure wound therapy for hard-to-heal wounds: a systematic review and meta-analysis. J Wound Care. 2024;33(12):950-957. DOI: 10.12968/jowc.2022.0213
This content is for informational purposes only and does not constitute medical advice. Hyperbaric oxygen therapy should only be administered under the supervision of qualified medical professionals at accredited facilities. Consult with a hyperbaric medicine specialist to determine if HBOT is appropriate for your patient’s specific clinical situation. Treatment decisions should be based on individual patient assessment and current clinical guidelines.