Common Questions
Frequently Asked Questions
Comprehensive answers about hyperbaric oxygen therapy in Canada, select a category to explore.
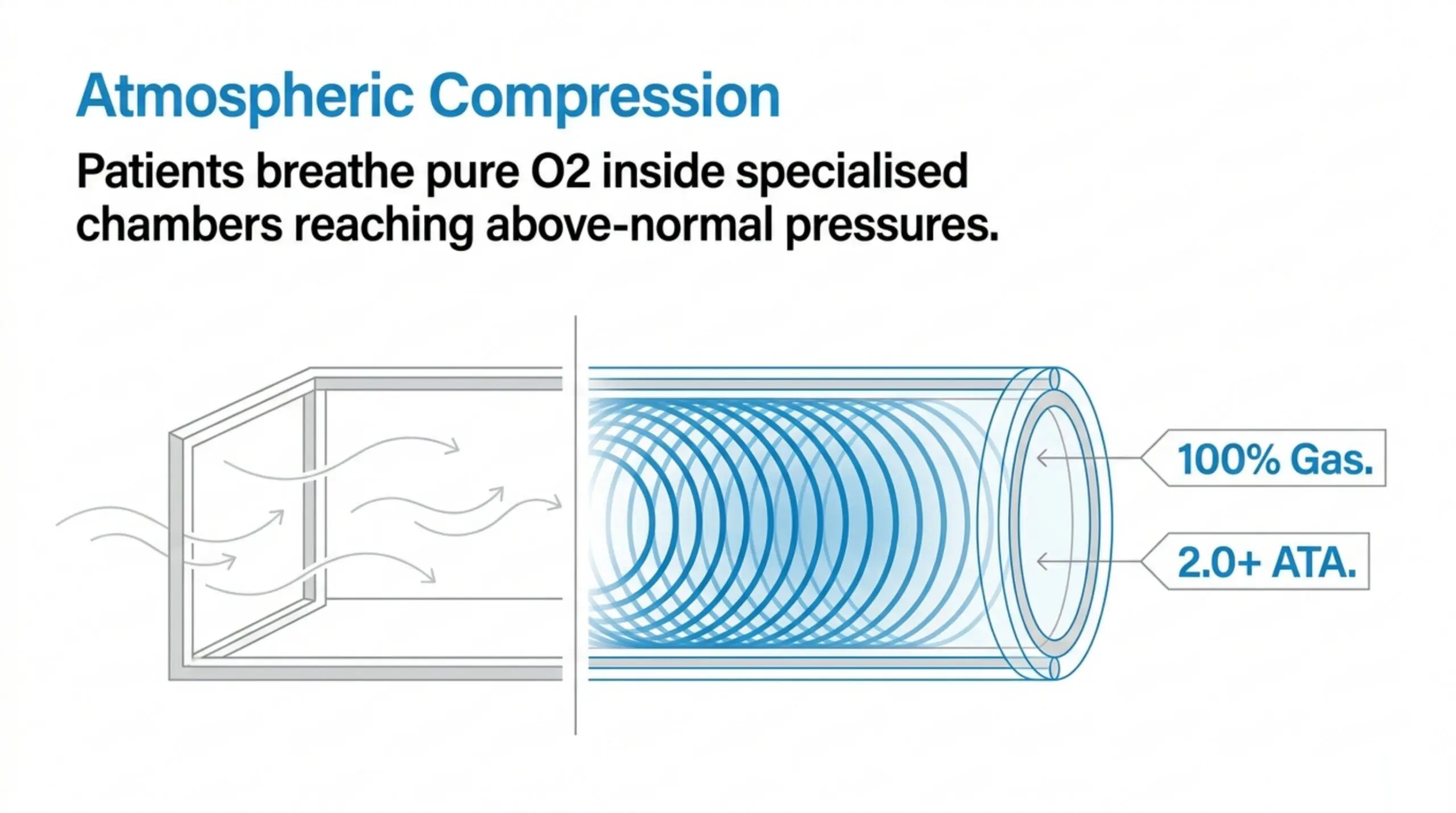
Hyperbaric oxygen therapy (HBOT) is a medical treatment where patients breathe 100% pure oxygen inside a pressurised chamber at pressures above normal atmospheric levels, typically between 1.5 and 3.0 atmospheres absolute (ATA). This dramatically increases the amount of dissolved oxygen in the blood plasma, up to 10 to 15 times normal levels, enabling enhanced oxygen delivery to tissues throughout the body. HBOT promotes healing through mechanisms including angiogenesis (new blood vessel formation), stem cell mobilization, reduced inflammation, and enhanced antimicrobial activity. Treatments typically last 60 to 120 minutes per session.
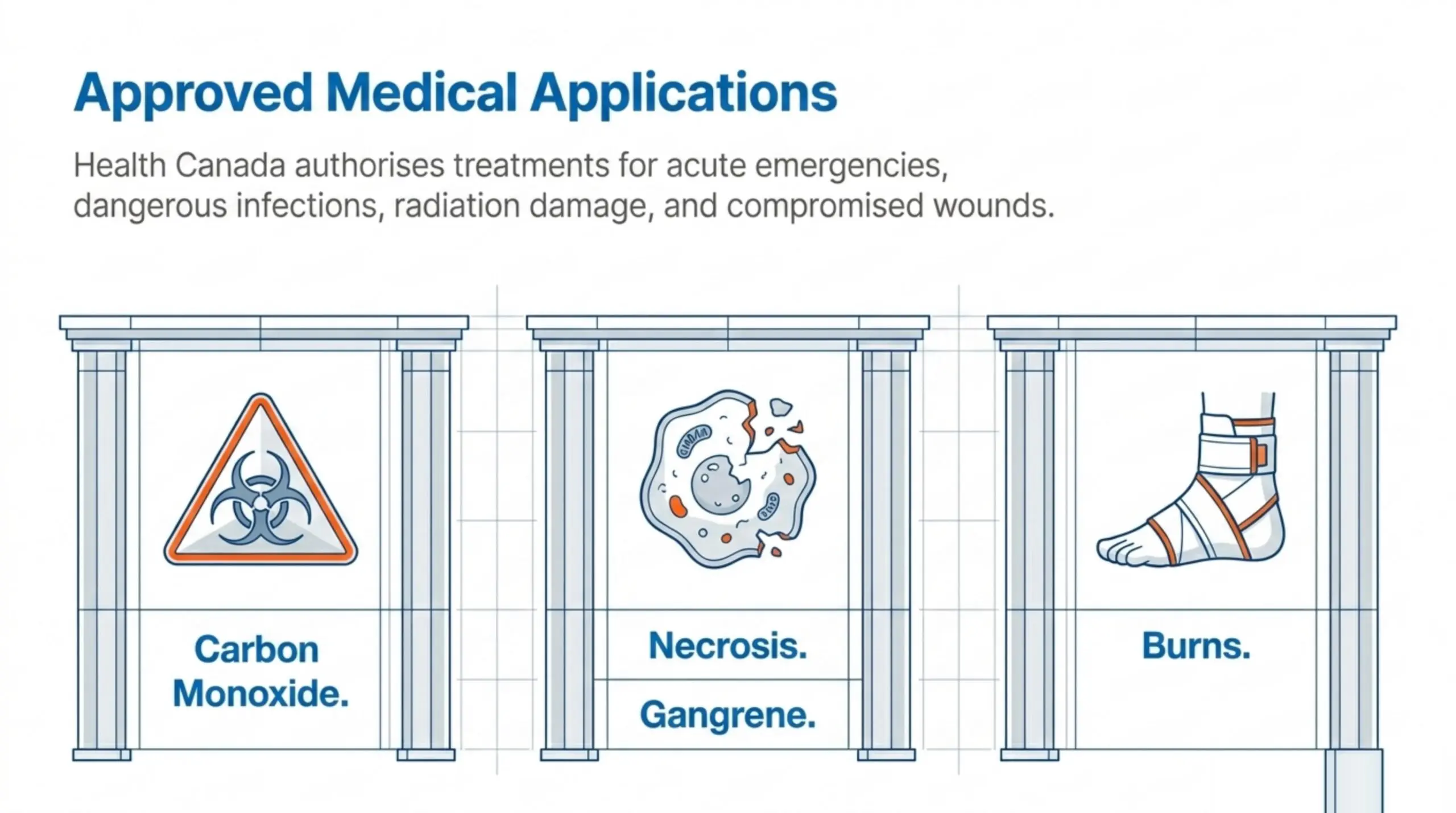
In Canada, 14 conditions are publicly funded for HBOT at hospital programmes. The canonical Ottawa Hospital list, used as the OHIP reference: (1) air or gas embolism, (2) carbon monoxide poisoning, (3) gas gangrene, (4) crush injury, compartment syndrome & acute traumatic ischaemia, (5) decompression sickness, (6) enhancement of healing in selected problem wounds, (7) exceptional blood loss (anaemia), (8) necrotizing soft tissue infections, (9) chronic osteomyelitis, (10) soft tissue radiation necrosis, (11) radiation damage affecting bone, (12) compromised skin grafts & flaps, (13) thermal burns, and (14) sudden sensorineural hearing loss. Intracranial abscess is on the UHMS Indications list but not on Health Canada's 14-condition list; where it is treated, funding should be confirmed with the receiving hospital. Emerging research is investigating HBOT for traumatic brain injury, stroke recovery, long COVID, fibromyalgia, and PTSD.
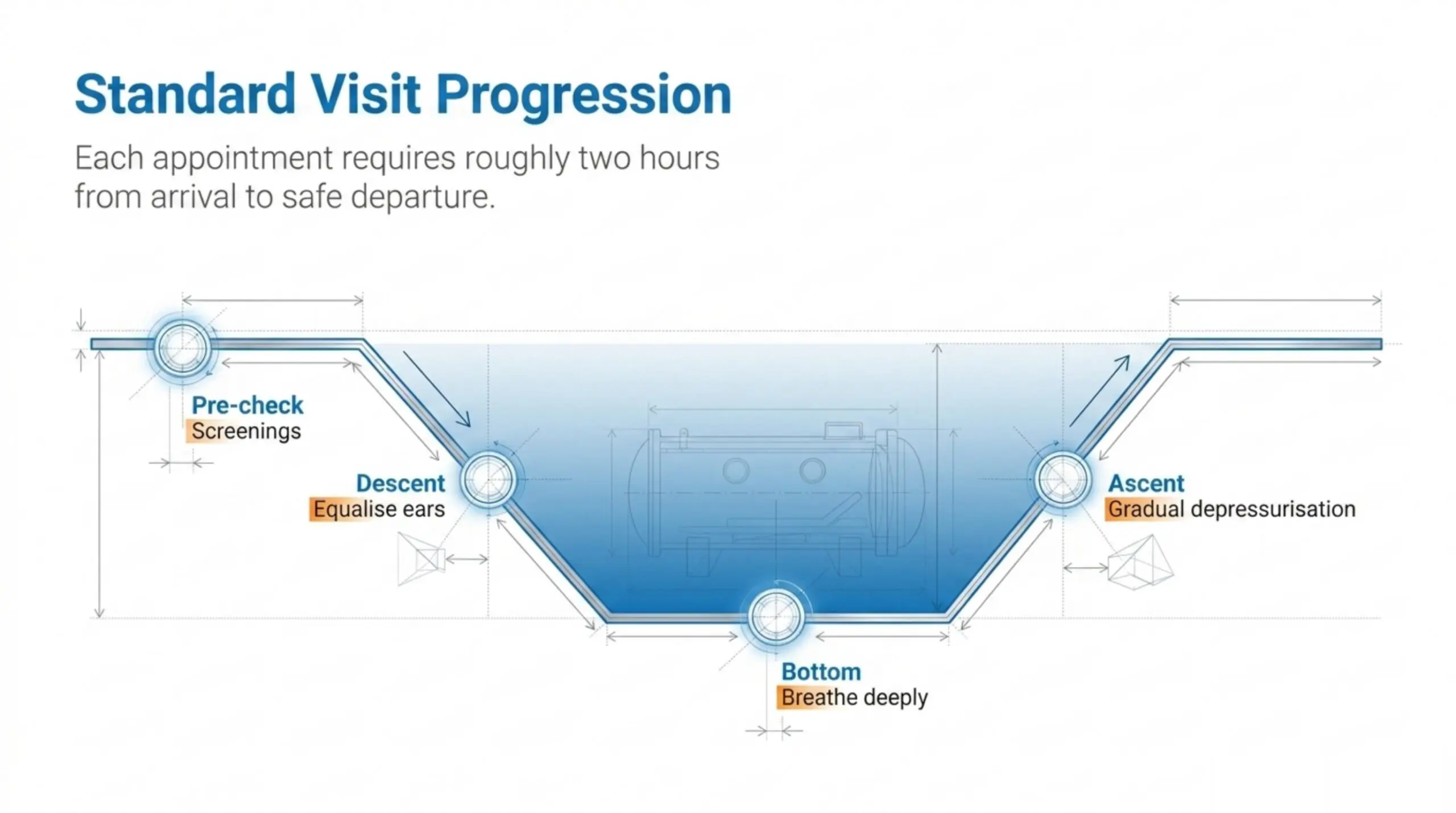
Before: You will change into a hospital gown or cotton clothing. Metal objects, electronics, and certain personal items are not permitted inside the chamber. Your care team will review equalization techniques for your ears, similar to what you would do on an airplane. During: You will sit or lie down inside the chamber while breathing pure oxygen. Sessions typically last 60 to 120 minutes. You may hear a hissing sound as the chamber pressurises and feel fullness in your ears, yawning or swallowing usually relieves this. Many patients watch television, listen to music, or sleep. After: The chamber depressurises gradually over 10 to 15 minutes. You can return to normal activities immediately. Your care team may check your blood pressure, pulse, and ears. Some patients feel temporarily lightheaded or fatigued, but this typically resolves quickly.
The number of sessions varies significantly by condition and severity. Emergency conditions like carbon monoxide poisoning or decompression sickness may require only 1 to 5 treatments. Chronic wound care protocols typically involve 20 to 40 sessions over several weeks. Radiation injury treatment may require 30 to 60 sessions. Each session generally lasts 60 to 120 minutes at pressures between 2.0 and 2.4 ATA. Your treating physician will develop a protocol specific to your condition, and treatment plans are regularly reassessed based on clinical response.
For hospital-based HBOT covered by provincial health insurance, you typically need a referral from your family physician or specialist to a hospital with a hyperbaric medicine program. Major programs exist in Toronto (Toronto General Hospital), Vancouver (Vancouver General Hospital), Halifax (QEII Health Sciences Centre), Hamilton (Hamilton Health Sciences), Ottawa (The Ottawa Hospital), and other centres. Note that some provinces, including Manitoba and PEI, do not have public hospital-based HBOT programs - patients in those regions are typically referred to facilities in neighbouring provinces. For private clinics, a physician referral may not be required, but a medical assessment is always performed before treatment begins. Contact your provincial health authority or the Canadian Undersea and Hyperbaric Medical Association (CUHMA) for guidance on finding an accredited facility near you.
A monoplace chamber treats one patient at a time in a clear acrylic tube pressurised entirely with 100% oxygen. No mask or hood is needed, and many patients find the visibility less claustrophobic. A multiplace chamber is a larger steel room that treats several patients simultaneously; the room is pressurised with air while patients breathe 100% oxygen through a hood or mask. Multiplace chambers allow medical staff to enter during treatment, which is important for critically ill patients or emergencies. Both types are medical-grade, NFPA-99 certified, and equally effective, the choice depends on the facility and clinical needs. Most Canadian hospital programs use monoplace chambers, while some military and larger centres operate multiplace units.
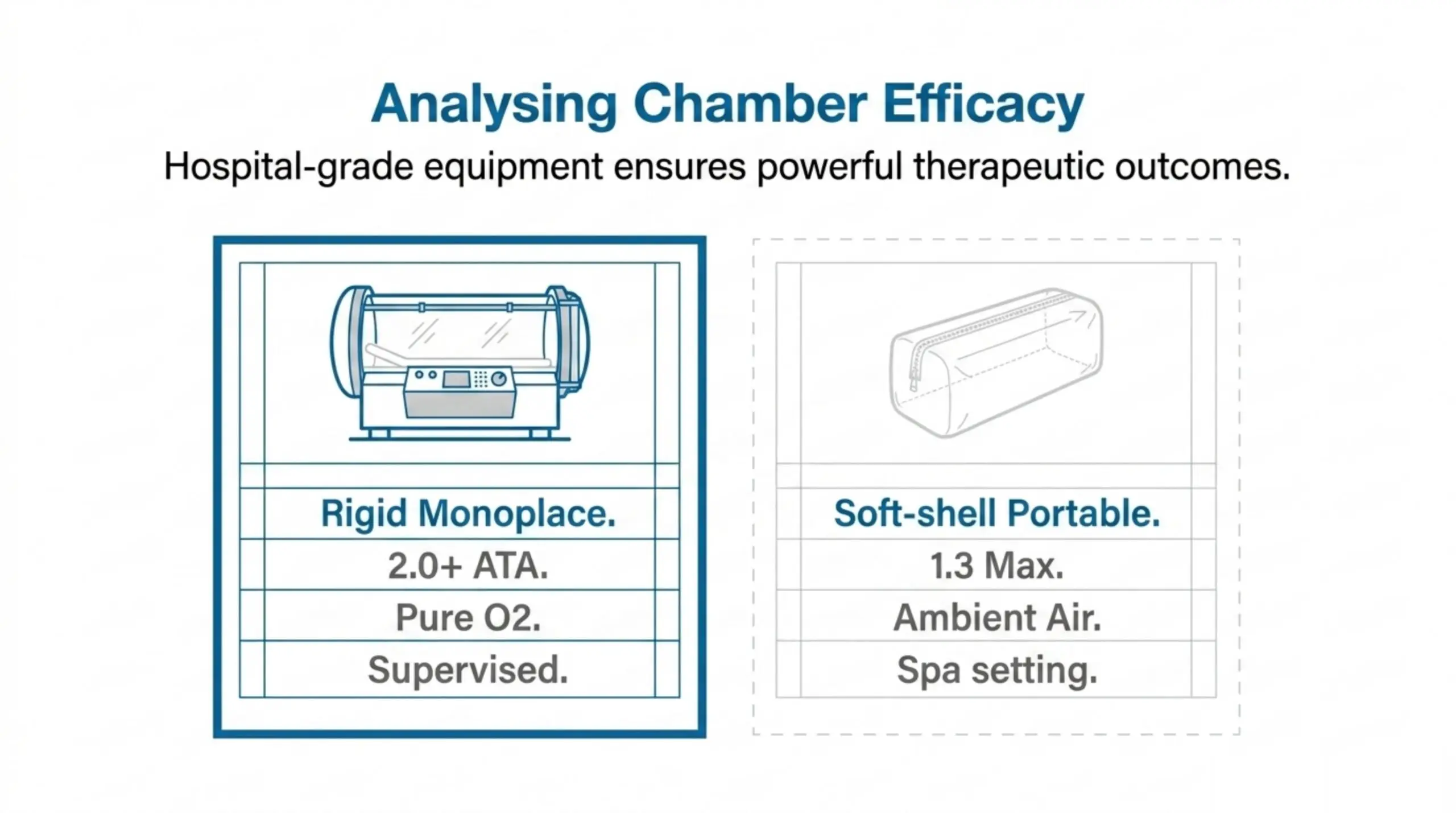
Clinical HBOT uses rigid monoplace or multiplace chambers capable of reaching 2.0 to 3.0 ATA while delivering 100% oxygen. These are the chambers used in hospital settings and supported by the peer-reviewed clinical literature. "Mild" or "soft-shell" portable chambers typically only reach 1.3 to 1.5 ATA and deliver concentrated air (approximately 24 to 28% oxygen, not 100%). Health Canada and the FDA authorize soft chambers only for acute mountain sickness. The evidence base for recognised conditions is built on clinical-grade HBOT at 2.0+ ATA. Therapeutic equivalence of mild HBOT has not been established for most conditions. If you are considering home-use or portable chambers, discuss the clinical limitations with your healthcare provider.
Claustrophobia is a common concern among first-time HBOT patients, and the good news is that most people find treatment far more comfortable than they expect. Monoplace chambers are constructed from clear acrylic, allowing patients to see their surroundings at all times, while multiplace chambers are large enough to seat several people simultaneously, far from a confined space. For patients with significant anxiety, a mild sedation option can be discussed with your medical team to ensure you remain relaxed and comfortable throughout the session. Every chamber is equipped with a two-way intercom system so you can speak with a trained staff member at any moment during treatment. Clinical experience shows that the majority of patients who initially report claustrophobia adapt fully within their first one to two sessions once they experience the open sightlines and constant communication available to them.
Because hyperbaric chambers operate in a high-oxygen environment, clothing material is a critical safety consideration, 100% cotton garments are required, as synthetic fabrics such as polyester, nylon, and rayon can generate static electricity and pose a fire risk under elevated oxygen concentrations. Most facilities provide patients with approved cotton scrubs or a gown so you do not need to bring anything special. All jewelry, watches, electronics, lighters, and matches must be left outside the chamber before treatment begins. Petroleum-based products including lotions, creams, perfumes, colognes, hair sprays, and makeup are strictly prohibited, as these substances are highly flammable in oxygen-enriched conditions. Eyeglasses are generally permitted and can improve comfort during your session; confirm any specific items with your care team at check-in. Arriving with clean, unscented skin and leaving valuables securely stored will ensure your session proceeds safely and without delay.
Your visit begins with a pre-treatment screening where the team reviews your health status, confirms no contraindications are present, and answers any questions, plan to arrive 20 to 30 minutes before your scheduled session. You will then change into approved 100% cotton clothing, remove all prohibited items, and enter the chamber, where a staff member will walk you through what to expect. The compression phase lasts approximately 10 to 15 minutes as the chamber pressure is gradually increased; during this time you may notice a sensation of fullness in your ears, which is relieved using simple techniques such as swallowing, yawning, or the Valsalva manoeuvre, your technician will guide you through these. Once target pressure is reached, the treatment phase begins: you breathe 100% medical-grade oxygen through a mask or hood for 60 to 90 minutes while your body absorbs oxygen at levels up to 10 to 15 times greater than normal atmospheric breathing. The session concludes with a 10 to 15-minute decompression phase, after which a staff member will conduct a brief post-treatment assessment to confirm you feel well before you leave. Total visit time from arrival to departure is typically 2 to 2.5 hours, and most patients feel relaxed or mildly fatigued afterward, both normal responses to the therapy.
Hyperbaric oxygen therapy has gained significant visibility through its adoption by elite athletes and public figures, including NBA superstar LeBron James, who has credited HBOT as a cornerstone of his recovery regimen, as well as Tom Brady, Novak Djokovic, and Cristiano Ronaldo, all of whom have incorporated pressurised oxygen sessions into their performance and longevity protocols. Recording artist Justin Bieber has also spoken publicly about using hyperbaric therapy as part of his wellness routine, further driving mainstream awareness. Professional NBA, NFL, and MLB players have publicly used HBOT as part of their recovery regimens, and team training staff increasingly incorporate hyperbaric sessions into recovery protocols. It is important to note, however, that clinical decisions about HBOT should always be grounded in peer-reviewed medical evidence and a consultation with a qualified physician, not solely in celebrity endorsement.
Supplemental oxygen at normal atmospheric pressure (such as a home oxygen concentrator) raises the arterial oxygen content modestly but cannot dissolve additional oxygen into blood plasma the way hyperbaric pressure can. HBOT at 2.0 to 2.8 ATA produces roughly 15 to 20 times the plasma-dissolved oxygen achievable at sea level. This difference is what enables HBOT to reach tissues with poor circulation or to interrupt the pathology of carbon monoxide poisoning, decompression sickness, and gas embolism in ways home oxygen cannot.
Clinical-grade hyperbaric oxygen therapy delivers 100 per cent oxygen at 2.0 to 2.8 ATA inside a Health Canada-licensed chamber. Oxygen bars and "mild" or "soft" hyperbaric chambers operate at 1.3 ATA or less, sometimes with ambient air rather than concentrated oxygen, and are not Health Canada-licensed for the 14 recognised indications. The clinical evidence base supporting HBOT specifically references pressures of 2.0 ATA and above; lower-pressure protocols do not produce the same dissolved-oxygen physiology. Provincial health plans cover treatment only at hospital programmes operating clinical-grade chambers.
The evidence base varies by indication. For the 14 recognised conditions, the evidence ranges from gold-standard randomised controlled trials and Cochrane reviews (carbon monoxide poisoning, decompression sickness, diabetic foot ulcers, late radiation tissue injury) to robust observational and case-series evidence (gas gangrene, intracranial abscess, sudden sensorineural hearing loss). The UHMS Indications Manual (15th Edition, 2024) and CUHMA Standards of Practice both grade evidence per indication. Off-label uses (long COVID, traumatic brain injury, autism, anti-aging) have promising but predominantly preliminary evidence; the Canada Hyperbarics research database indexes 14,545+ peer-reviewed HBOT studies across all indications.
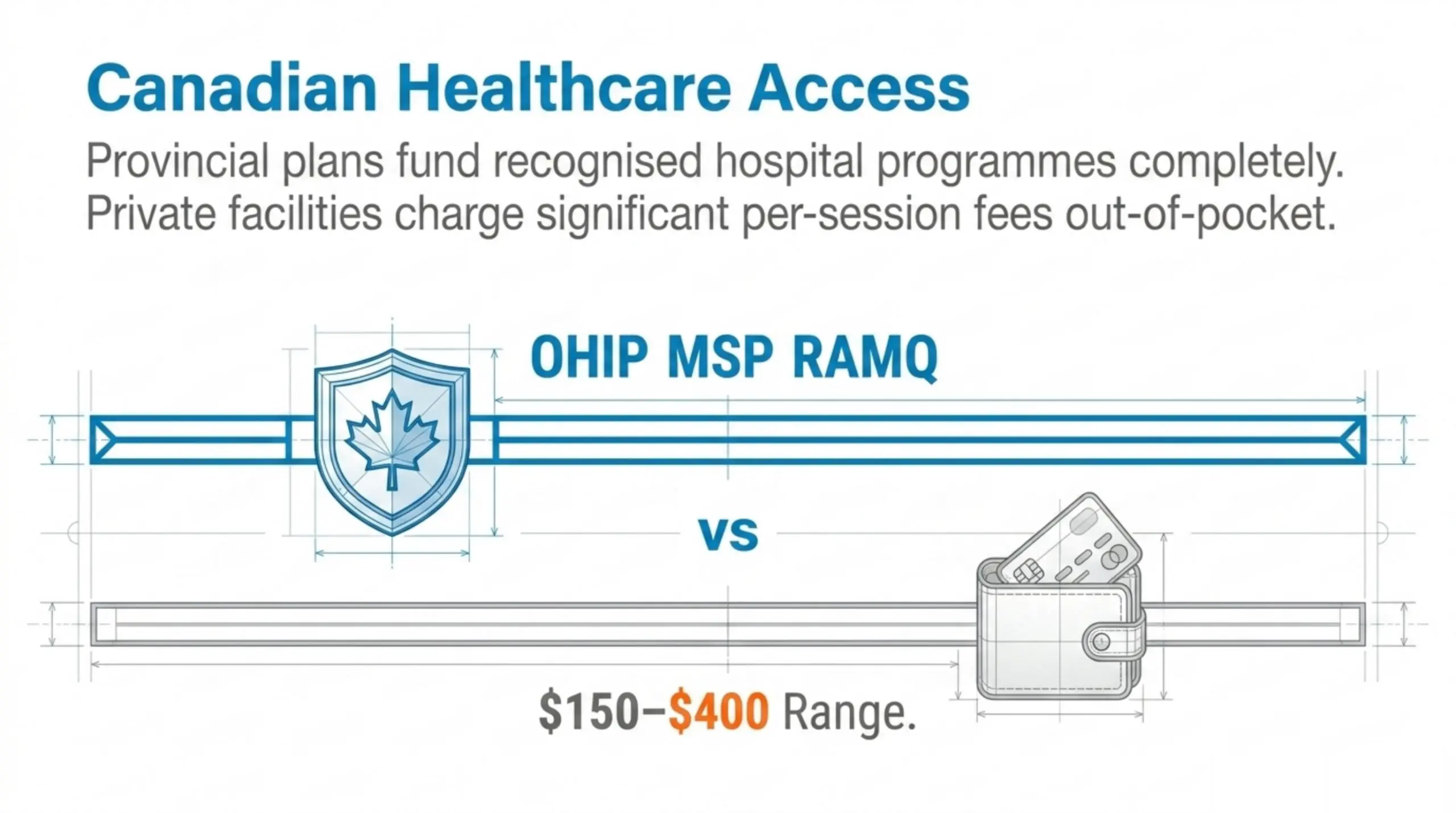
At hospital-based programs for approved indications, HBOT is covered by provincial health insurance at no direct cost to the patient. At private clinics, prices typically range from $150 to $400 per session depending on the facility, location, and chamber type. Many clinics offer package pricing, for example, a 20-session protocol may cost $3,000 to $6,000 total. Some clinics offer introductory sessions at lower rates ($79 to $150). A typical 40-session wound care protocol at a private clinic could cost $6,000 to $16,000 out-of-pocket. Always ask about package discounts and check whether your extended health insurance or workplace benefits cover any portion before committing.
Yes. OHIP covers hyperbaric oxygen therapy for the 14 recognised conditions at hospital-based programmes (Toronto General Hospital / UHN, Hamilton General Hospital, The Ottawa Hospital) with a physician referral. A limited number of Independent Health Facilities (IHFs) across Ontario are also licensed for hyperbaric services and select facilities may bill OHIP for approved indications; eligibility varies by facility and indication, so confirm directly with the treating site before booking. Private clinics that are not licensed IHFs operate on a self-pay basis ($150 to $400 per session typical). You need a physician referral and a valid OHIP card for covered treatment. WSIB may also cover HBOT for work-related injuries.
Yes, but only at one facility. The British Columbia Medical Services Plan (MSP) covers hyperbaric oxygen therapy at Vancouver General Hospital (Leon Judah Blackmore Pavilion, operated by Vancouver Coastal Health) for the 14 recognised conditions with a physician referral. VGH is the only hospital-based hyperbaric chamber in BC and provides 24/7 emergency coverage with a multiplace chamber capable of supporting ventilated critical care patients. Private hyperbaric clinics in BC (BaroMedical in Greater Vancouver, others) are not MSP-covered; treatment at these facilities is on a self-pay basis ($150 to $400 per session typical). Patients on Vancouver Island, in the Interior, or in Northern BC are coordinated to VGH through their physician and BC Patient Transfer Network for both elective and emergency care. See the BC coverage page for full details.
Alberta: Alberta Health covers HBOT at two hospital programmes, Misericordia Community Hospital in Edmonton (Covenant Health, 24/7) and Foothills Medical Centre / Arthur J.E. Child Comprehensive Cancer Centre in Calgary (AHS, weekday outpatient). The hospital billing code is 13.99I. The College of Physicians & Surgeons of Alberta (CPSA) accredits private hyperbaric clinics for safety and quality standards; CPSA accreditation does not automatically grant Alberta Health billing. Quebec: RAMQ covers hospital-based HBOT at Hôtel-Dieu de Lévis (an 18-person multiplace chamber, one of the largest in Canada) and Hôpital du Sacré-Cœur de Montréal, both 24/7. Nova Scotia: MSI covers HBOT at the QEII Health Sciences Centre in Halifax; chronic and elective wait times are commonly 12 to 18 months. Newfoundland and Labrador: MCP covers HBOT at Health Sciences Centre in St. John's. Saskatchewan: The Wigmore Regional Hospital chamber in Moose Jaw has been partially reopened with reduced hours since July 2021; many patients are referred to Calgary. Manitoba and New Brunswick: No public hospital HBOT programme; patients are referred interprovincially (Edmonton or Ontario for Manitoba; Halifax for New Brunswick). PEI, Yukon, NWT, Nunavut: No facilities; out-of-territory referral. See the Canada coverage guide for the full breakdown.
Some extended health insurance plans in Canada offer partial coverage for HBOT, but it is not standard. Coverage depends on your plan, employer, and the insurer. Plans from major providers like Sun Life, Manulife, Great-West Life, and Blue Cross may cover HBOT if it is prescribed by a physician for a recognised medical condition, but this varies widely by policy. Veterans Affairs Canada (VAC) may cover HBOT for eligible veterans. WSIB, CNESST (Quebec), and other workers' compensation boards may cover HBOT for workplace injuries. Always request a pre-authorization from your insurance provider before starting treatment, and obtain a detailed treatment prescription from your referring physician.
In Canada, medical expenses paid out-of-pocket that exceed a threshold (the lesser of 3% of net income or a set dollar amount, which changes annually) may be claimed on your income tax return via the Medical Expense Tax Credit (METC). HBOT prescribed by a licensed medical practitioner for a diagnosed condition generally qualifies as an eligible medical expense under the Income Tax Act. Keep all receipts and obtain a letter from your treating physician confirming medical necessity. Consult a tax professional or visit the CRA website for the most current thresholds and eligibility requirements, as individual circumstances vary.
Private-pay HBOT in Canada's major cities typically ranges from $150 to $400 per session, depending on chamber type and clinical complexity. Toronto and the GTA: $150 to $400 at private clinics; OHIP-covered at Toronto General Hospital and at select OHIP-eligible Independent Health Facilities. Vancouver and Greater Vancouver: $150 to $400 at private clinics (BaroMedical, others); MSP-covered only at Vancouver General Hospital. Calgary and Edmonton: $175 to $300 at private clinics; Alberta Health-covered at Foothills/AJECCC Calgary and Misericordia Edmonton. Montreal: $175 to $325 at private clinics; RAMQ-covered at Hôpital du Sacré-Cœur. Ottawa, Hamilton, Halifax, Winnipeg: covered by the relevant provincial plan at the local hospital programme; private clinic options exist in some cities. A full course of 20 to 40 daily sessions for a chronic indication typically totals $3,000 to $16,000 out-of-pocket where not covered. Most private extended health plans do not cover HBOT unless specifically listed; ask your plan administrator about extended health benefits and check whether VAC, WSIB, or CNESST applies to your situation.
At private clinics across Canada, a single HBOT session typically ranges from $150 to $400, depending on the province, facility, and type of chamber used. Hospital-based HBOT for provincially approved medical indications, such as wound healing or radiation injury, is covered by provincial health plans and available at no direct cost to the patient. Most private clinics offer package pricing for multi-session courses (commonly 10 to 40 sessions), which can reduce the per-session cost by 10 to 25%. Prices tend to be higher in major urban centres like Toronto and Vancouver, while rural or smaller-market clinics may charge less. An initial consultation or assessment, which is typically required before beginning treatment, often carries a separate fee of $100 to $250. It is worth contacting your provincial health authority or insurer in advance, as some extended health benefit plans cover a portion of privately delivered HBOT.
Soft-shell mild hyperbaric chambers operating at 1.3 to 1.5 ATA are commercially available in Canada and can be purchased from suppliers including OxyNova, a Canadian manufacturer, with prices typically ranging from $5,000 to $25,000. Health Canada has authorized soft-shell chambers only for the treatment of acute mountain sickness; any other use in a home setting falls outside their approved indication. Clinical-grade rigid chambers capable of reaching 2.0 to 3.0 ATA cost $50,000 to $200,000 or more and require trained medical supervision to operate safely. A critical distinction that buyers must understand is that home chambers operate at lower pressures and do not deliver 100% oxygen, ambient air is pressurised rather than pure O2, making them fundamentally different from and not equivalent to clinical HBOT. The therapeutic evidence base for HBOT is built on clinical-pressure, 100% oxygen protocols, and outcomes from home chambers cannot be assumed to replicate those results. Consult a qualified physician before purchasing any hyperbaric device to ensure it is appropriate for your medical situation.
From a purely financial standpoint, ownership of a mild home chamber may appear cost-effective for individuals prescribed 40 or more sessions, since cumulative clinic fees can exceed the purchase price of an entry-level soft-shell unit. However, home chambers are limited to 1.3 to 1.5 ATA and ambient air, whereas clinical HBOT delivers 100% oxygen at 2.0 to 3.0 ATA, a meaningful physiological difference that directly affects dissolved oxygen levels in the blood and tissues. The established evidence base supporting HBOT for recognised conditions is derived entirely from clinical protocols; home devices do not replicate these conditions and should not be assumed to produce comparable therapeutic outcomes. Clinical settings also provide continuous professional monitoring, emergency protocols, and the involvement of trained hyperbaric technicians and physicians, safeguards that are absent during unsupervised home use. For any UHMS- or recognised indication, clinical HBOT is strongly recommended over home alternatives, regardless of cost considerations.
Five factors drive the per-session price: chamber type (multiplace chambers cost more to operate and require an inside attendant trained in hyperbaric nursing), staffing (a registered respiratory therapist or hyperbaric technician must monitor every session), treatment pressure and duration (higher pressures and longer sessions use more medical-grade oxygen), regulatory and accreditation costs (CPSA accreditation in Alberta, equivalent provincial standards elsewhere, Health Canada device licensing), and clinic overhead. Hospital programmes have similar real costs but are funded by provincial health insurance for recognised indications.
Provincial health insurance covers HBOT at hospital-based programmes for the 14 recognised conditions with a physician referral: OHIP (Ontario), MSP (BC), AHCIP code 13.99I (Alberta), RAMQ (Quebec), MSI (Nova Scotia), Saskatchewan Health, MCP (Newfoundland). The referral pathway starts with a family physician or specialist (hyperbaric medicine, wound care, infectious disease, otolaryngology for SSHL, ophthalmology for retinal indications). The referring physician faxes the referral to the closest hospital hyperbaric unit; treatment begins after the unit's hyperbaric physician confirms appropriateness. Emergency cases bypass the elective pathway via CritiCall Ontario (1-800-668-4357) or equivalent provincial networks.
Coverage varies widely by plan. Some private extended health plans (workplace benefits, individual policies) cover specific HBOT indications when prescribed by a physician; many do not cover off-label uses. Pre-authorisation is typically required before treatment begins. Workplace health spending accounts sometimes cover all or part of private-clinic HBOT regardless of indication. Always confirm coverage with your specific plan administrator before booking, and provide the clinical indication plus proposed session count so the administrator can give a definitive answer.
HBOT is generally considered safe when administered by trained professionals in accredited facilities. The most common side effect is barotrauma, pressure-related ear or sinus discomfort, which can usually be managed with equalization techniques. Temporary myopia (nearsightedness) may occur during extended treatment courses but typically resolves within weeks after treatment ends. Rare but serious risks include oxygen toxicity seizures (fewer than 1 in 10,000 treatments) and pneumothorax. The overall adverse event rate in published literature is approximately 0.4%. A thorough medical evaluation is always performed before treatment begins to identify any individual risk factors.
The only absolute contraindication for HBOT is an untreated pneumothorax (collapsed lung). Relative contraindications that require careful evaluation include: current or recent treatment with certain chemotherapy drugs (bleomycin, cisplatin, doxorubicin), uncontrolled high fever, severe claustrophobia, uncontrolled seizure disorders, certain cardiac conditions (severe heart failure), chronic obstructive pulmonary disease (COPD) with CO2 retention, active upper respiratory infections, recent ear surgery, and pregnancy (though HBOT has been used safely for carbon monoxide poisoning in pregnant women). Some older pacemaker models may not be compatible. Your hyperbaric physician will conduct a full assessment including chest X-ray and ENT evaluation before approving treatment.
Yes, HBOT is used safely in both paediatric and geriatric populations. In children, it is commonly used for carbon monoxide poisoning, certain wounds, and is being researched for conditions like cerebral palsy and autism spectrum disorder. Paediatric patients may need a parent or caregiver present during treatment, and sessions may be shorter depending on the child's age. For elderly patients, HBOT is widely used for diabetic wound care, radiation injury, and other approved indications. Patients over 65 are more likely to experience temporary vision changes (myopia), but these are reversible. The treating physician adjusts pressure and duration based on the patient's overall health and tolerance.
Yes, in fact, diabetic wound healing is one of the most common and well-established uses of HBOT. Non-healing diabetic foot ulcers (Wagner grade 3 and above) are a recognised condition. HBOT can significantly reduce amputation rates in diabetic patients with chronic wounds. However, diabetic patients should be aware that HBOT can temporarily lower blood glucose levels, so monitoring and meal planning are important. Your care team will check blood sugar before and after sessions and may adjust insulin or medication timing. Diabetic patients are also more prone to the temporary myopia side effect. Speak with your endocrinologist and hyperbaric physician to coordinate your diabetes management plan during treatment.
A standard clinical HBOT session involves pressurising to 2.0 to 2.4 ATA over 10 to 15 minutes, breathing 100% oxygen for 60 to 90 minutes (often with short "air breaks" every 20 to 30 minutes to reduce oxygen toxicity risk), then depressurising over 10 to 15 minutes. Sessions are typically administered once or twice daily, five days per week. Total session count depends on the condition: 1 to 5 sessions for acute emergencies, 20 to 40 for chronic wounds, 30 to 60 for radiation injury. Your physician will reassess progress every 10 to 15 sessions and may order imaging or wound measurements to track response.
HBOT works through several well-characterized mechanisms. At elevated pressure, oxygen dissolves directly into blood plasma (not just haemoglobin), reaching tissues even where red blood cells cannot flow due to damaged vasculature. This hyperoxygenation triggers: angiogenesis, the growth of new blood vessels into ischaemic tissue; stem cell mobilization, an 8-fold increase in circulating stem/progenitor cells after 20 sessions; anti-inflammatory effects, suppression of pro-inflammatory cytokines and reduction of oedema; antimicrobial activity, direct bactericidal effects on anaerobic organisms and enhanced white blood cell killing capacity; and collagen synthesis, fibroblast proliferation and extracellular matrix deposition essential for wound repair. The intermittent nature of treatment (oxygen exposure followed by normal air) is itself therapeutic, creating a "hyperoxic-normoxic" cycle that upregulates growth factors.
For recognised conditions, HBOT is firmly evidence-based medicine supported by decades of randomised controlled trials, Cochrane systematic reviews, and inclusion in clinical guidelines worldwide. It is covered by provincial health systems in Canada and recognised by Health Canada as a Class III medical device therapy. However, HBOT is also marketed by some private clinics for non-approved conditions where evidence is preliminary or insufficient. The distinction matters: hospital-based HBOT for approved indications is mainstream medicine; using HBOT for unproven claims outside clinical guidelines moves into experimental or alternative territory. Always check whether a condition is recognised, and evaluate the quality of evidence (randomised trials vs. case reports) when considering HBOT for emerging applications.
Pregnancy is generally listed as a relative contraindication for elective HBOT. However, HBOT is used during pregnancy for emergency indications such as carbon monoxide poisoning, where the risk of NOT treating outweighs potential risks. Animal studies have not shown teratogenic effects at standard clinical pressures. The decision must be made on a case-by-case basis with the treating physician. Routine or elective HBOT is not recommended during pregnancy due to limited human safety data. Always disclose pregnancy status before any HBOT treatment.
After standard HBOT sessions for chronic conditions, most patients can fly within 24 hours without concern. However, if you received HBOT for decompression sickness or arterial gas embolism, military and undersea medicine guidelines recommend waiting 24 to 72 hours before air travel. The concern is that reduced cabin pressure at altitude could cause dissolved gases to form bubbles. Your hyperbaric physician will advise you on safe flying intervals based on your specific treatment. For routine HBOT sessions, there are generally no flight restrictions, but it is best practice to wait at least 12 hours.
The duration of HBOT effects varies by condition and protocol. For wound healing and tissue repair, benefits can be long-lasting or permanent as HBOT stimulates the growth of new blood vessels (angiogenesis) and tissue remodeling. For neurological conditions like TBI, some studies report sustained cognitive improvements months to years after completing treatment. Anti-inflammatory effects may diminish over weeks if the underlying condition persists, and maintenance sessions may be recommended. Most clinical protocols involve 20 to 60 sessions, with measurable benefits typically becoming apparent after 10 to 20 treatments. For chronic conditions, periodic booster sessions (monthly or quarterly) may help maintain results.
This is a critical distinction. Clinical-grade HBOT used in hospitals operates at 2.0 to 3.0 ATA with 100% oxygen, this is the pressure range supported by the vast majority of published clinical evidence and recognised conditions. Mild or "soft-shell" portable chambers operate at only 1.3 to 1.5 ATA with concentrated air (approximately 24 to 28% oxygen), delivering significantly less oxygen to tissues. At 2.4 ATA with 100% O2, blood plasma oxygen levels reach approximately 1,800 mmHg; at 1.3 ATA with ambient air, plasma oxygen reaches only about 100 to 120 mmHg, a 15-fold difference. The evidence base for approved indications like diabetic wounds, radiation injury, and decompression sickness is built entirely on clinical-grade pressures. Mild HBOT may have some benefits for general wellness, but it should not be considered equivalent to medical HBOT.
HBOT and red light therapy (photobiomodulation) work through entirely different mechanisms but are both used in recovery and wellness settings. HBOT increases dissolved oxygen in blood plasma systemically throughout the entire body, while red light therapy uses specific wavelengths (630 to 850 nm) to stimulate mitochondrial ATP production locally in targeted tissues. HBOT has a robust clinical evidence base with 14 recognised conditions and decades of randomised controlled trials; red light therapy has growing evidence for skin health, wound healing, and pain management but fewer large-scale clinical trials. Some clinics combine both therapies, as HBOT floods tissues with oxygen while red light enhances cellular energy production, potentially complementary mechanisms. HBOT requires specialized chambers and clinical oversight; red light therapy devices are widely available for home use. Neither is a replacement for the other, they address different physiological pathways.
HBOT and cryotherapy serve different roles in recovery. Cryotherapy exposes the body to extreme cold (-110°C to -140°C) for 2 to 3 minutes to trigger vasoconstriction, reduce acute inflammation, and provide pain relief, effects that are largely short-term and symptomatic. HBOT increases tissue oxygenation over 60 to 120 minute sessions, promoting angiogenesis, stem cell mobilization, collagen synthesis, and long-term tissue repair, effects that build cumulatively over multiple sessions. For acute sports injuries, cryotherapy may provide faster immediate pain relief; for chronic conditions, tissue healing, and neurological recovery, HBOT has a substantially larger evidence base. Professional athletes like LeBron James and Novak Djokovic reportedly use both modalities as part of comprehensive recovery protocols. The choice depends on the goal: short-term symptom relief (cryotherapy) versus deep tissue healing and systemic recovery (HBOT).
Emerging research suggests HBOT and stem cell therapy may have synergistic effects. HBOT has been shown to mobilize endogenous stem cells from bone marrow, a single HBOT session can increase circulating stem/progenitor cells by up to 800% according to a study published in the American Journal of Physiology. When combined with exogenous stem cell treatments, HBOT may enhance stem cell survival, engraftment, and differentiation by improving the oxygen environment in target tissues. Several longevity clinics now offer combined HBOT and stem cell protocols, particularly for neurological conditions and anti-aging. However, this combination remains experimental and is not part of standard clinical guidelines. Patients interested in combined therapy should seek providers with expertise in both modalities and ensure treatments are conducted under proper medical supervision.
HBOT is increasingly used as an adjunct to accelerate post-surgical healing. By dramatically increasing tissue oxygenation, HBOT promotes collagen synthesis, reduces oedema and bruising, enhances immune function to lower infection risk, and accelerates wound closure. For compromised skin grafts and flaps, a recognised condition, HBOT is standard of care. In plastic and cosmetic surgery, some surgeons recommend pre- and post-operative HBOT protocols to improve outcomes, particularly for facelifts, abdominoplasty, and breast reconstruction. Studies have shown reduced post-operative complications and faster return to normal activities. While not all surgical procedures require HBOT, it may be particularly beneficial for patients with compromised healing (diabetics, smokers, irradiated tissue) or following complex reconstructive surgery.
Common side effects (in roughly 1 in 5 to 1 in 10 patients) are middle-ear barotrauma during compression, sinus pressure or congestion, transient claustrophobia in monoplace chambers, and short-term myopia (nearsightedness) that develops over a long course and reverses within weeks of finishing. Less common are dental barotrauma if an existing filling has trapped air, fatigue, and reversible cataract progression in patients having very long courses. Serious adverse events (oxygen seizures, chamber-related pneumothorax) are uncommon at clinical pressures and well-managed by trained chamber operators.
The only absolute contraindication is untreated pneumothorax (trapped air in the chest expands on decompression and can cause tension pneumothorax); concurrent bleomycin chemotherapy (oxygen-induced pulmonary fibrosis risk) and concurrent disulfiram (interferes with superoxide dismutase, the enzyme that neutralises hyperbaric-oxygen-generated free radicals) are treated as effectively absolute at most programmes, though the UHMS classifies them as relative. Relative contraindications include severe haemodynamic instability requiring continuous high-dose vasopressor titration, uncontrolled seizure disorder, severe COPD with bullous lung disease, recent middle-ear or sinus surgery, and uncontrolled claustrophobia. Pregnancy is not a contraindication; HBOT is the standard of care for severe carbon monoxide poisoning in pregnant patients.
Pregnancy is not a contraindication to hyperbaric oxygen therapy. HBOT is the standard of care for severe carbon monoxide poisoning in pregnant patients, where the foetus is at higher CO risk than the mother due to foetal haemoglobin's slower CO-clearance kinetics. For elective and chronic indications, treatment during pregnancy is decided case-by-case with the referring obstetrician and the hyperbaric unit; routine elective indications are usually deferred until after delivery unless the clinical benefit clearly outweighs the unknown long-term foetal exposure.
HBOT for TBI and concussion is one of the most actively researched emerging applications. Studies by Harch et al. (2012) demonstrated improvements in symptoms, cognitive testing, and SPECT brain imaging in military patients with blast-induced TBI. Israeli researchers led by Efrati have published multiple studies showing HBOT can promote neuroplasticity even years after injury. A 2025 double-blind RCT in Scientific Reports found significant improvements in olfaction, anxiety, and sleep. However, results across trials have been mixed, and HBOT for TBI is not yet a recognised condition. This is particularly relevant in Canada given the prevalence of contact sports including hockey. The evidence base continues to grow.
Emerging evidence is promising. A 2022 randomised, sham-controlled, double-blind trial published in Scientific Reports found that 40 HBOT sessions significantly improved global cognitive function, attention, executive function, energy levels, sleep quality, and psychiatric symptoms in post-COVID patients. A 2022 Canadian review by the CDA-AMC identified HBOT as an emerging therapy for post-COVID-19 condition. The proposed mechanisms include reducing neuroinflammation, improving cerebral blood flow, and promoting tissue repair in organs damaged by the virus. However, HBOT for long COVID is not yet a recognised condition, and larger multi-centre trials are ongoing. Several Canadian clinics are offering HBOT for long COVID on an off-label basis.
Diabetic wound healing is one of the recognised applications of HBOT. The Kranke et al. Cochrane review (2015) and multiple RCTs show HBOT improves healing rates for chronic diabetic foot ulcers (Wagner grade 3+). Evidence on amputation reduction is mixed: Kranke Cochrane was supportive, while Fedorko et al. 2016 (Canadian RCT, Diabetes Care) found no amputation benefit. HBOT is a recognised condition for non-healing diabetic wounds when standard wound care has failed. In Canada, hospital-based HBOT for diabetic wounds is covered by provincial health insurance when medically indicated. With over 3.7 million Canadians living with diagnosed diabetes (Diabetes Canada), this remains an important application of hyperbaric medicine.
A multicentre, randomised, double-blind controlled trial (Rossignol et al., 2009, BMC Pediatrics, PMID 19284641) of 62 children with autism found that 40 HBOT sessions at 1.3 atm led to significant improvements in overall functioning, receptive language, social interaction, and eye contact, 80% of treated children improved versus 38% of controls. The proposed mechanism involves reducing neuroinflammation observed in the brains of children with ASD. However, subsequent studies have produced mixed results, and HBOT for autism is not a recognised condition. Health Canada and major medical organisations do not currently endorse HBOT for ASD. Families considering this option should discuss the evidence carefully with their healthcare team.
HBOT does not treat or cure cancer itself. However, it plays an important evidence-based role in managing radiation injury, a common side effect of cancer treatment. HBOT is a recognised condition for delayed radiation injury affecting the soft tissues, bones (osteoradionecrosis), bladder (radiation cystitis), bowel (radiation proctitis), and other organs. A Cochrane systematic review (2023, 18 studies, 1,071 participants) confirmed HBOT may result in complete resolution or significant improvement of late radiation tissue injury in head, neck, bladder, and rectum. Recent trials include the HONEY RCT (2024, JAMA Oncology) showing measurable improvements in irradiated breast tissue, and RICH-ART 5-year follow-up (2025) confirming sustained benefit for radiation-induced cystitis. Some preclinical research suggests HBOT may sensitize tumour cells to radiation and chemotherapy, but this is not yet established in clinical practice. Importantly, systematic reviews have found no evidence that HBOT promotes tumour growth, addressing a common historical concern. For specific cancer types (glioblastoma, breast cancer wound complications, head and neck osteoradionecrosis), see the dedicated questions below.
Glioblastoma is not on the Canadian list of 14 recognised conditions for HBOT, and HBOT is not a standard or publicly funded treatment for the disease in Canada. Research interest has focused on HBOT as a potential radiosensitiser when given immediately before radiotherapy, on the rationale that increasing tumour oxygenation may make hypoxic glioma cells more responsive to radiation. Small early-phase trials (notably from Stenström and colleagues, and several Japanese centres) have explored HBOT plus radiotherapy for newly diagnosed glioblastoma, with mixed results and modest sample sizes. A separate, established and recognised use of HBOT in this patient population is for delayed radiation injury to the brain following cranial radiotherapy (radiation necrosis, soft-tissue radiation necrosis); this indication is publicly funded at hospital programmes and is supported by the 2023 Cochrane review. Patients considering HBOT alongside glioblastoma treatment should discuss it with their neuro-oncology team; in Canada, glioblastoma-directed HBOT would generally be available only on a research-protocol or self-pay basis.
Yes. Hyperbaric oxygen therapy is an established, evidence-based treatment for radiation cystitis (also called haemorrhagic radiation cystitis), a delayed complication of pelvic radiotherapy that can cause persistent urinary bleeding, urgency, frequency, and pain. Radiation cystitis falls under "soft tissue radiation necrosis," one of the 14 recognised conditions, and is publicly funded at hospital hyperbaric programmes across Canada with a physician referral. The strongest evidence comes from the RICH-ART randomised controlled trial; the 2025 5-year follow-up published in EClinicalMedicine confirmed sustained benefit of HBOT for radiation-induced cystitis. The 2023 Cochrane systematic review of late radiation tissue injury (18 studies, 1,071 participants) similarly found that HBOT may result in complete resolution or significant improvement of bladder and rectal radiation injury. A typical course is 30 to 60 daily sessions at 2.0 to 2.4 ATA. Patients with radiation cystitis should ask their oncology or urology team for a referral to the nearest hospital hyperbaric programme; see the conditions page for the full Canadian programme list.
Yes. Necrotizing soft-tissue infection (which includes necrotizing fasciitis) is one of Canada's 14 recognised conditions for HBOT and is the most time-critical infectious indication. Adjunctive hyperbaric oxygen therapy is delivered alongside the mainstays of treatment, urgent surgical debridement and broad-spectrum intravenous antibiotics, on the rationale that high tissue oxygen tension inhibits anaerobic organisms (especially Clostridium species), restores neutrophil oxidative killing, and may reduce the extent of further surgical excision. Treatment is provided at hospital hyperbaric programmes (Toronto General / UHN, Hamilton General, The Ottawa Hospital, Vancouver General, Misericordia Edmonton, Foothills Calgary, Hôtel-Dieu de Lévis, Hôpital du Sacré-Cœur de Montréal, QEII Halifax, Health Sciences Centre St. John's) under provincial coverage, typically as 1 to 2 daily sessions for the first several days of admission with a multiplace chamber capable of supporting critical care patients. For suspected necrotizing fasciitis, call 911 immediately; the receiving emergency department coordinates urgent surgery, antibiotics, and hyperbaric transfer through CritiCall Ontario or the equivalent provincial transfer network.
Yes. Osteoradionecrosis (ORN), most commonly of the mandible, is one of the longest-established uses of HBOT and is included on Canada's 14 recognised conditions as "radiation damage affecting bone." The clinical concept of ORN as a problem of hypoxic, hypocellular, hypovascular tissue, and the rationale for adjunctive HBOT, was set out in the foundational papers by Marx (J Oral Maxillofac Surg 1983; PMID 6572704 and 6574217). Two main protocols are used in Canada: therapeutic for established ORN (commonly 30 to 40 sessions, with additional sessions if surgical resection is planned), and prophylactic before dental extractions or surgery in previously irradiated tissue (commonly 20 to 30 pre-operative sessions plus 10 post-operative). A large 276-patient Australasian study (Tahir et al. 2014, DOI 10.1111/ajco.12289) reported an 86% overall response rate for established mandibular ORN and a 96% response rate for prophylactic HBOT. ORN of less common sites such as the ribs, sternum, or femoral head is also covered under the same recognised indication. Treatment is publicly funded at hospital hyperbaric programmes with a referral from oral surgery, otolaryngology, radiation oncology, or orthopaedics.
A widely publicized 2020 study by Hachmo et al. (Aging, PMID 33206062) found that 60 sessions of HBOT in healthy adults over 64 increased telomere length by up to 20% and reduced senescent cells by up to 37%, two key biological markers of aging. A 2021 study showed skin improvements including increased collagen density and reduced wrinkle area. A Frontiers in Aging review (2024) explored HBOT's regenerative potential against age-related vascular cognitive decline. However, these findings are from small studies and have not yet been replicated in large-scale clinical trials. Anti-aging is not a recognised condition. Claims that HBOT can "reverse aging" should be viewed with scientific caution, though the research is generating significant interest in the longevity science community.
A prospective clinical trial by Efrati et al. (2015, PLoS One, PMID 26010952) of 60 female fibromyalgia patients found that 40 HBOT sessions at 2 ATA significantly improved all fibromyalgia symptoms and quality of life. SPECT brain imaging confirmed that HBOT corrected abnormal brain activity in pain-processing regions. Additional studies have shown similar results, though sample sizes remain small. Fibromyalgia is not a recognised condition, and HBOT for chronic pain is considered experimental. The proposed mechanism involves modulating central sensitization in the brain rather than treating peripheral tissue. Patients interested in HBOT for fibromyalgia should discuss the evidence with their rheumatologist and understand that treatment will be out-of-pocket at a private clinic.
Growing research suggests HBOT may benefit mental health conditions. An RCT of 190 post-stroke depression patients (Guo et al., 2023, World J Psychiatry) found HBOT combined with antidepressants significantly outperformed medication alone, also reducing inflammatory markers. For PTSD, studies in military veterans showed 52% of those meeting PTSD criteria no longer met diagnostic thresholds after HBOT. A double-blind trial found improvements in anxiety and sleep. The proposed mechanisms include reducing neuroinflammation, improving cerebral perfusion, and promoting neuroplasticity. However, HBOT for psychiatric conditions is not yet recognised, evidence comes primarily from small trials, and this application is considered experimental. Patients should not discontinue prescribed psychiatric medications in favour of HBOT.
The evidence for HBOT in stroke is mixed and depends on timing. For chronic post-stroke patients, the Efrati et al. 2013 RCT (PLoS ONE, 74 patients, 6-36 months post-stroke) demonstrated neurological improvements with HBOT at 2.0 ATA over 40 sessions. A 2020 retrospective analysis of 162 post-stroke patients reported 86% clinically significant cognitive improvement. For acute ischaemic stroke, however, a 2024 meta-analysis (BMC Neurology, 8 RCTs, 493 patients) found no statistically significant benefit from HBOT. The proposed mechanism for chronic benefit involves stimulating neuronal activity in the "penumbral zone", brain tissue that is metabolically impaired but not yet dead. HBOT for stroke is not currently a recognised condition under Canadian provincial coverage, and timing of treatment (acute versus chronic phase) remains a subject of active research.
A 2021 systematic review and meta-analysis (Singh et al., Eur J Gastroenterol Hepatol, PMID 33905214) of 18 studies found overall response rates of 83% for HBOT in ulcerative colitis and 82% in Crohn's disease. For fistulizing Crohn's disease, complete fistula healing was achieved in 48% of patients. Most adverse events were minor. HBOT may help by reducing intestinal inflammation, promoting mucosal healing, and enhancing oxygen delivery to inflamed bowel tissue. IBD is not a recognised condition, and HBOT is considered adjunctive, not a replacement for standard IBD therapy (biologics, immunosuppressants). However, for patients with refractory disease who have failed conventional treatments, HBOT may be worth discussing with a gastroenterologist.
Yes, idiopathic sudden sensorineural hearing loss (ISSNHL) is a recognised condition for HBOT. A 2022 JAMA Otolaryngology meta-analysis (Joshua et al., PMID 34709348) found HBOT as combination treatment was significantly associated with improved hearing, with mean gains of 10.3 dB and an odds ratio of 4.3 for recovery. The key factor is timing: HBOT is most effective when started within 14 days of symptom onset, ideally combined with corticosteroids. After 3 months, the benefit diminishes significantly. If you experience sudden hearing loss in one ear, seek medical attention immediately, this is a medical emergency, and early HBOT referral can make a meaningful difference in outcomes.
HBOT is increasingly used by professional athletes for accelerated recovery from soft tissue injuries, fractures, and concussions. NHL players, NFL athletes, and Olympic competitors have publicly used HBOT. Former NHL player Daniel Carcillo has been a prominent advocate for HBOT in post-concussion syndrome recovery. The proposed benefits for athletes include reduced inflammation and oedema, faster tissue repair, decreased muscle fatigue, and improved return-to-play timelines. However, most evidence for sports recovery comes from case reports and small studies rather than large RCTs. HBOT for general sports recovery is not a recognised condition. In Canada, athletes typically access HBOT through private clinics.
A 2021 review in Frontiers in Aging (Balasubramanian et al., PMID 35821996) examined HBOT's role against age-related cerebromicrovascular pathologies contributing to vascular cognitive impairment and dementia. HBOT may protect the microvasculature, reduce amyloid plaque burden (in animal models), and improve cerebral blood flow. Case reports have shown cognitive improvements in individual Alzheimer's patients after HBOT. However, Alzheimer's and dementia are not recognised conditions, and no large-scale human RCTs have been completed. With approximately 771,939 Canadians living with dementia as of January 2025 (Alzheimer Society of Canada), this is an area of significant research interest. Clinical trials are underway, but it is too early to recommend HBOT as a standard treatment for dementia.
A study by Akarsu et al. (2013, Undersea Hyperb Med, PMID 23682549) of 16 CFS patients found that 15 HBOT sessions over three weeks significantly improved fatigue severity and quality of life (p<0.005). The overlap between CFS/ME and long COVID symptoms has renewed interest in HBOT for this population. Proposed mechanisms include improving mitochondrial function, reducing neuroinflammation, and enhancing tissue oxygenation. However, evidence is limited to small studies, and ME/CFS is not a recognised condition. Given the lack of effective conventional treatments for CFS, some patients pursue HBOT privately, but expectations should be calibrated to the preliminary nature of the evidence.
HBOT has been explored for chronic Lyme disease (post-treatment Lyme disease syndrome) based on its antimicrobial and anti-inflammatory properties. In vitro research by Sapi et al. (2017) demonstrated that hyperbaric oxygen can eliminate Borrelia burgdorferi biofilms in laboratory settings. Some patients with persistent Lyme symptoms report symptomatic improvement after HBOT. However, there are no published randomised controlled trials on HBOT for Lyme disease, and it is not a recognised condition. With Lyme disease expanding in Canada, particularly in Ontario, Quebec, Nova Scotia, and Manitoba, there is interest in adjunctive therapies, but the evidence for HBOT remains preclinical and anecdotal. Standard antibiotic treatment remains the first-line approach.
A Cochrane systematic review found no consistent evidence that HBOT provides clinically significant benefit for multiple sclerosis. Early studies in the 1980s showed some promise for bladder dysfunction, but randomised controlled trials have not demonstrated sustained improvement in disability, fatigue, or relapse rates. HBOT is not a recognised condition for MS and is not recommended by the MS Society of Canada as a standard treatment. Some patients report subjective symptom relief, but this has not been replicated in controlled settings. The largest trial (New England Journal of Medicine, 1983) found no meaningful difference between HBOT and placebo groups.
The evidence for HBOT in cerebral palsy is limited and controversial. A landmark Canadian RCT (Collet et al., 2001, The Lancet) found that both hyperbaric oxygen and pressurised air groups showed improvements, but there was no significant difference between the two, suggesting a possible pressure effect rather than an oxygen-specific benefit. HBOT is not a recognised condition for cerebral palsy, and some expert reviews have concluded there is no proven benefit and potential for harm (barotrauma). Some families pursue HBOT for children with CP through private clinics, but major paediatric organisations do not endorse it as standard therapy. More research is needed before evidence-based recommendations can be made.
Peripheral neuropathy, particularly diabetic neuropathy, is an area of growing HBOT research. Several studies suggest HBOT may improve nerve conduction velocity, reduce neuropathic pain, and promote nerve fiber regeneration through enhanced tissue oxygenation and growth factor stimulation. A 2010 study in Diabetes Care showed that HBOT improved sensory perception in diabetic patients with foot ulcers. For chemotherapy-induced peripheral neuropathy (CIPN), preliminary case series have shown some symptom improvement. However, neuropathy is not currently a recognised condition, and large-scale randomised trials are still needed. HBOT may be most beneficial as an adjunct in patients with neuropathy secondary to diabetic wounds, a recognised condition.
HBOT is most effective for tinnitus when it accompanies idiopathic sudden sensorineural hearing loss (ISSHL), a recognised condition. For acute tinnitus (onset within 3 months), studies report improvement in up to 70% of patients when HBOT is started promptly. A Cochrane review found that HBOT may improve hearing for acute ISSHL when administered early, particularly within 2 weeks of onset. However, for chronic tinnitus lasting more than 3 to 6 months, the evidence does not support HBOT, a Cochrane review found no beneficial effect for chronic tinnitus. The key factor is timing: early intervention is critical. If you experience sudden hearing loss or acute tinnitus, seek medical attention immediately, HBOT may be part of the treatment protocol if initiated within the first few weeks.
Research on HBOT for migraines is limited but intriguing. A small number of clinical studies have shown that HBOT may reduce migraine frequency and intensity, potentially through its anti-inflammatory effects and modulation of nitric oxide pathways. A 2009 Cochrane review examined hyperbaric oxygen for migraine and cluster headache, finding some evidence that HBOT could terminate acute migraine attacks, but insufficient evidence to support its routine use. Cluster headaches have shown more promising responses to HBOT in case reports. Migraine and headache disorders are not recognised conditions, and HBOT is not a first-line treatment, standard pharmacological therapies remain the primary approach. Patients with refractory migraines unresponsive to conventional treatment may wish to discuss HBOT with their neurologist.
HBOT is being investigated for autoimmune and rheumatic conditions based on its anti-inflammatory and immunomodulatory properties. A 2025 review in Frontiers in Medicine examined HBOT for rheumatoid arthritis, systemic lupus erythematosus, and other autoimmune conditions, finding that hyperbaric oxygen can modulate cytokine production, reduce oxidative stress, and suppress overactive immune responses. Some case reports and small studies have shown improvements in joint inflammation and pain scores. However, there are no large-scale randomised controlled trials for any autoimmune condition, and HBOT is not a recognised condition for autoimmune diseases. Concerns exist about theoretically stimulating immune activity in some autoimmune conditions. This remains an early-stage research area, and patients should discuss potential risks and benefits with their rheumatologist.
Emerging research suggests HBOT may benefit erectile dysfunction (ED) through its ability to promote angiogenesis (new blood vessel growth) and improve endothelial function in penile tissue. A 2018 pilot study published in the International Journal of Impotence Research reported significant improvements in erectile function scores in men who completed 40 HBOT sessions at 2.0 ATA. The proposed mechanism involves enhanced nitric oxide production and restoration of blood flow to cavernosal tissue. HBOT has also shown promise in treating ED secondary to radiation therapy for prostate cancer, radiation injury being a recognised condition. However, ED itself is not a recognised condition for HBOT, and larger randomised controlled trials are needed. Patients should consider HBOT as an experimental option to discuss with their urologist, not a replacement for established ED treatments.
Limited but emerging evidence suggests HBOT may support hair growth through increased scalp blood flow, oxygen delivery to hair follicles, and stimulation of growth factors. Oxygen is essential for the metabolic activity of hair follicle cells, and the hypoxic environment of damaged or thinning scalps may contribute to hair loss. Some case reports and small studies have noted improved hair density following HBOT protocols, particularly in patients with alopecia areata (autoimmune hair loss). HBOT may also benefit hair transplant outcomes by enhancing graft survival and wound healing. However, hair loss is not a recognised condition, clinical evidence is very limited, and HBOT should not be considered a proven treatment for pattern baldness or other common forms of hair loss. More rigorous clinical trials are needed before any evidence-based recommendations can be made.
Research suggests HBOT may positively affect metabolic parameters, though it is not a weight loss treatment per se. A study published in Diabetes/Metabolism Research and Reviews showed that HBOT increased peripheral insulin sensitivity by approximately 37 to 40% in overweight men with and without type 2 diabetes. HBOT may enhance glucose and lipid metabolism in skeletal muscle and reduce adipose tissue inflammation. Animal studies have demonstrated reduced body weight and fat accumulation following hyperbaric oxygen exposure. However, HBOT is not a recognised condition for obesity or metabolic syndrome, and it should not be viewed as a substitute for diet, exercise, and established metabolic therapies. The metabolic effects of HBOT are a promising research area, particularly as an adjunct for patients with diabetes and metabolic syndrome.
Preliminary research on HBOT and fertility is emerging. A pilot study in Fertility and Sterility investigated HBOT as an adjunct to IVF, finding that it was well tolerated and showed a decreased cycle cancellation rate. HBOT may benefit fertility through improved endometrial blood flow, enhanced oocyte quality (demonstrated in animal models), and improved uterine receptivity. For male fertility, a 2025 systematic review and meta-analysis found significant improvements in sperm survival, density, morphology, and motility following HBOT. HBOT has also been explored for patients with resistant thin endometrium during frozen embryo transfer. However, fertility is not a recognised condition, evidence is preliminary, and larger randomised controlled trials are needed before HBOT can be recommended as a standard fertility adjunct.
Yes, carbon monoxide (CO) poisoning is one of the original and most well-established recognised conditions for HBOT. Carbon monoxide binds to haemoglobin with approximately 250 times the affinity of oxygen, forming carboxyhaemoglobin and preventing oxygen delivery to tissues. HBOT at 2.5 to 3.0 ATA reduces the half-life of carboxyhaemoglobin from 4 to 6 hours (breathing room air) to approximately 15 to 23 minutes, rapidly restoring oxygen transport. HBOT also addresses CO poisoning at the cellular level by displacing CO from cytochrome c oxidase and reducing lipid peroxidation in the brain. Clinical guidelines recommend HBOT for patients with significant CO poisoning, including loss of consciousness, neurological symptoms, cardiac involvement, or carboxyhaemoglobin levels above 25%. In Canada, emergency HBOT for CO poisoning is available at major hospital-based hyperbaric centres and is covered by provincial health insurance.
Thermal burns are a recognised condition for HBOT. HBOT enhances burn wound healing by increasing tissue oxygen levels in the hypoxic zone surrounding the burn, promoting neovascularization, reducing oedema through vasoconstriction (while maintaining oxygenation), and enhancing white blood cell bactericidal activity. Studies have shown that adjunctive HBOT for burns can reduce healing time, decrease the need for skin grafting, lower infection rates, and improve survival in severe burn cases. HBOT is typically initiated within 24 hours of the burn injury and continued daily alongside standard burn care. For chronic non-healing wounds beyond burns, including surgical wounds, pressure ulcers, and traumatic injuries, HBOT is also well-supported as an adjunctive therapy. In Canadian burn centres, HBOT availability varies by facility, but it is recognised as part of comprehensive burn management protocols.
Some HBOT patients report improved sleep quality as a secondary benefit of treatment, though the evidence for HBOT as a primary sleep therapy is limited. The proposed mechanisms include reduced neuroinflammation, improved cerebral blood flow, and modulation of neurotransmitter systems involved in sleep regulation. A study in long COVID patients treated with HBOT noted significant improvements in sleep quality scores as part of overall symptom improvement. HBOT's effects on the autonomic nervous system, shifting toward parasympathetic dominance, may contribute to improved sleep architecture. However, insomnia and sleep disorders are not recognised conditions, and HBOT should not be considered a first-line treatment for sleep problems. Patients who notice sleep improvements during HBOT are likely benefiting from treatment of an underlying condition that was disrupting their sleep.
HBOT has established applications in dental and oral surgery, particularly for osteoradionecrosis (bone death in the jaw following radiation therapy), a recognised condition. For dental implants, HBOT may enhance osseointegration (the bonding of implant to bone) by increasing oxygen delivery to the surgical site and promoting bone formation. Experimental studies have shown that HBOT stimulates effective bone formation around implants placed in irradiated bone. HBOT is also used to treat medication-related osteonecrosis of the jaw (MRONJ), a complication sometimes seen with bisphosphonate therapy. For routine dental implants in healthy patients, HBOT is generally not necessary, but it may be particularly beneficial for patients with compromised healing, such as those with prior head/neck radiation, diabetes, or heavy smoking history. Consult with your oral surgeon about whether HBOT could benefit your specific situation.
Yes, veterinary hyperbaric oxygen therapy is a growing field. HBOT is used in veterinary medicine for many of the same conditions as in humans, including wound healing, post-surgical recovery, snake bites, spinal cord injuries (intervertebral disc disease), smoke inhalation, burns, and soft tissue infections. Dogs, cats, and even rabbits can receive HBOT, and most animals do not require sedation, many dogs relax and even sleep during treatments once acclimated to the chamber. A 2021 Frontiers in Veterinary Science study analyzing 2,792 treatment sessions reported a very low adverse event rate. Veterinary HBOT facilities exist in Canada and the United States, typically at specialty veterinary hospitals and referral centres. If your pet has a condition that might benefit from enhanced oxygen delivery, speak with your veterinarian about whether HBOT is available and appropriate.
Health Canada does not maintain its own clinical indications list. It licenses hyperbaric chambers as Class III medical devices under the Canadian Medical Devices Regulations and defers to the Undersea and Hyperbaric Medical Society (UHMS) for recognised indications. The UHMS Indications Manual (15th Edition, 2024) lists 15 indications, having added avascular necrosis as the 15th. In Canada, provincial plans publicly fund 14 of these conditions at hospital programmes (the exact covered list varies slightly by province); UHMS-listed indications not routinely funded (such as intracranial abscess in some provincial pathways) may still be treated case-by-case. Always confirm with the receiving hospital and the referring physician.
To find the nearest hyperbaric oxygen therapy facility, use our facilities directory: enter your postal code or browse the interactive map showing all 33 verified hyperbaric facilities across Canada (11 hospital programmes and 22 private clinics in 9 provinces). City-level guides are also available for Toronto, Vancouver, Calgary, Edmonton, Montreal, Ottawa, Hamilton, Halifax, Winnipeg, and 13 other Canadian cities; each lists the nearest facilities, their contact details, and whether they bill the provincial health plan or operate self-pay. Patients in Prince Edward Island, Yukon, Northwest Territories, or Nunavut have no in-territory chamber and are referred to the closest out-of-province facility (most commonly QEII Halifax, VGH Vancouver, Misericordia Edmonton, or The Ottawa Hospital). For emergency hyperbaric needs (carbon monoxide poisoning, gas embolism, severe necrotising infection), call 911 first; the receiving emergency department coordinates urgent transfer.
Canada has both hospital-based and private hyperbaric facilities across the country. Hospital programmes include: Ontario, Toronto General Hospital, Hamilton General Hospital, and The Ottawa Hospital; British Columbia, Vancouver General Hospital; Quebec, Sacré-Coeur Hospital (Montreal), Hôtel-Dieu de Lévis; Nova Scotia, QEII Health Sciences Centre (Halifax); Alberta, Arthur J.E. Child Comprehensive Cancer Centre / Foothills Medical Centre (Calgary), Misericordia Hospital (Edmonton); Saskatchewan, Dr. F.H. Wigmore Regional Hospital (Moose Jaw, subject to staffing availability, confirm current status with SHA before planning travel); Newfoundland & Labrador, Health Sciences Centre (St. John's). Additionally, a growing number of private clinics operate in Toronto, the GTA, Greater Vancouver, Edmonton, Montreal, Ottawa, and other cities. The Canadian Armed Forces also operates hyperbaric chambers at CFB Esquimalt and other locations. See our facilities directory for the full listing.
When evaluating a hyperbaric facility, consider: Accreditation, Is the facility accredited or affiliated with a hospital system? Does it follow UHMS or CSA (Canadian Standards Association) guidelines? Medical oversight, Is there a physician trained in hyperbaric medicine on staff or supervising? Look for UHMS certification or fellowship training. Chamber type, Clinical-grade monoplace or multiplace chambers that reach 2.0+ ATA with 100% oxygen are standard; be cautious of facilities using only soft-shell/portable chambers. Emergency protocols, Does the facility have written emergency procedures and trained hyperbaric technicians? Transparency, A reputable facility will clearly distinguish between recognised and experimental indications and will not make unsubstantiated cure claims.
Hyperbaric access in Northern and rural Canada is limited but growing. A small number of private clinics in Northern Ontario and other remote regions operate modern clinical-grade chambers (including Perry Baromedical and similar hard-shell systems) to serve remote populations. Some Canadian Armed Forces installations and offshore diving operations in northern regions also have hyperbaric capabilities. For most patients in remote areas, accessing HBOT requires travel to a major urban centre with a hospital programme. Provincial health authorities may arrange interprovincial referrals and cover travel costs for emergency indications like carbon monoxide poisoning or decompression sickness. Telemedicine consultations with hyperbaric physicians are becoming more available, helping northern patients determine whether travel for HBOT is warranted for their condition.
Hospital-based programs operate within accredited hospitals, are staffed by physicians with hyperbaric training, typically treat recognised conditions, accept provincial health insurance, and have access to full emergency medical support. Wait times may be longer, and treatment is limited to recognised medical indications. Approved independent facilities are regulated private clinics that meet provincial accreditation standards. In Ontario, select some eligible independent facilities may bill OHIP for approved indications; confirm eligibility directly with the treating site for covered indications. In Alberta, CPSA accredits private HBOT clinics; contact individual facilities regarding billing arrangements. Non-approved private clinics in other provinces offer faster access and more flexible scheduling, but costs are out of pocket (typically $150 to $400 per session) unless covered by private insurance. Both hospital and approved independent facilities use clinical-grade chambers and are subject to regulatory oversight. The best choice depends on your province, condition, and coverage eligibility.
Canada has 33 hyperbaric oxygen therapy facilities across 9 provinces: 11 hospital-based programmes (Ontario, BC, Alberta, Quebec, Nova Scotia, Saskatchewan, Newfoundland) and 22 private clinics. Provinces without an in-province hospital programme (Manitoba, New Brunswick, PEI, the territories) refer publicly funded patients interprovincially. The closest facility depends on your postal code and on whether you need hospital coverage (for one of the 14 recognised conditions with referral) or private self-pay treatment. See our facilities directory for the complete list by province.
Hospital-based hyperbaric programmes treat the 14 recognised conditions at no out-of-pocket cost to patients with valid provincial health insurance and a physician referral. They operate clinical-grade multiplace or monoplace chambers, provide 24/7 emergency coverage in most cases, and accept interprovincial referrals where in-province hospital capacity is absent. Wait times for elective and chronic indications can range from weeks to months depending on province. Private clinics are self-pay (or covered by extended health benefits where the plan applies), charge $150 to $400 per session, typically operate during business hours, and offer faster access for elective and off-label indications. Both must use Health Canada-licensed chamber equipment.
Health Canada classifies hyperbaric chambers as Class III medical devices under the Medical Devices Regulations (SOR/98-282). This means they require pre-market review and licensing before being sold or used in Canada. Chambers must meet Canadian Standards Association (CSA) standards and the facility must comply with fire safety codes. Health Canada licenses hyperbaric chambers as Class III medical devices for 14 recognised conditions. Clinical practice decisions are guided by professional medical societies (like UHMS) and provincial health authorities. Health Canada has issued advisories warning consumers about unproven claims for HBOT, particularly from non-medical providers. The full Health Canada information page on HBOT is available at canada.ca.
In Canada, 14 conditions are publicly funded for HBOT at hospital programmes. The canonical Ottawa Hospital OHIP-covered list is: (1) Air or gas embolism, (2) Carbon monoxide poisoning, (3) Gas gangrene, (4) Crush injury, compartment syndrome & acute traumatic ischaemia, (5) Decompression sickness, (6) Enhancement of healing in selected problem wounds, (7) Exceptional blood loss (anaemia), (8) Necrotizing soft tissue infections, (9) Chronic osteomyelitis, (10) Soft tissue radiation necrosis, (11) Radiation damage affecting bone, (12) Compromised skin grafts & flaps, (13) Thermal burns, and (14) Sudden sensorineural hearing loss. The UHMS maintains a broader list including additional indications such as intracranial abscess and central retinal artery occlusion; some provinces (Alberta, BC, Quebec) recognise intracranial abscess under provincial coverage. These lists are reviewed and updated periodically by their respective bodies.
When evaluating HBOT claims, consider the evidence hierarchy: Strongest: Cochrane systematic reviews, large multi-centre RCTs, and meta-analyses published in peer-reviewed journals. Moderate: Single-centre RCTs, prospective cohort studies. Weakest: Case reports, case series, animal studies, and testimonials. Key questions to ask: Is the condition a recognised condition? Was the study published in a peer-reviewed journal indexed on PubMed? Did it use a sham/placebo control group? What was the sample size? Has it been replicated? Be cautious of clinics that cite only animal studies, single case reports, or unpublished data to justify treatment for a condition. Our Research Database includes over 100 peer-reviewed studies you can review directly.
The Canadian Undersea and Hyperbaric Medical Association (CUHMA) is Canada's national professional society for hyperbaric and diving medicine, aligned with international peers including the Undersea and Hyperbaric Medical Society (UHMS). Founded to promote excellence through education, best practices, and patient advocacy, CUHMA holds an annual scientific meeting (virtual in 2026 on May 2) and publishes a monthly e-newsletter. CUHMA members include physicians, researchers, nurses, hyperbaric technicians, and other professionals involved in undersea and hyperbaric medicine across Canada. For patients, CUHMA can be a resource for finding qualified hyperbaric physicians and accredited facilities. Visit cuhma.ca for more information.
Hyperbaric chambers are classified as Class III medical devices under the Canadian Medical Devices Regulations and are licensed by Health Canada. The licensing framework references the UHMS HBO Indications list when evaluating applications. Provincial Colleges of Physicians and Surgeons regulate clinical practice (CPSA in Alberta, CPSO in Ontario, equivalents in other provinces). CUHMA (Canadian Undersea and Hyperbaric Medical Association) publishes Standards of Practice Guidelines that hospital programmes and CPSA-accredited private clinics follow. Health Canada licenses devices (chambers), not facilities; "Health Canada approved" should be applied only to specific licensed chamber equipment, not to clinics.
Not necessarily. Many high-profile recreational chambers operate at 1.3 ATA or less ("mild" or "soft" hyperbaric chambers) and are not Health Canada-licensed for the 14 recognised clinical indications. Clinical-grade HBOT operates at 2.0 to 2.8 ATA on 100 per cent oxygen in Health Canada-licensed chambers under physician supervision. The evidence base supporting HBOT for the recognised indications references the clinical-grade pressures, not the mild-pressure protocols. Athletes and patients using mild chambers should understand the pressure and oxygen-concentration differences before extrapolating clinical-research outcomes.
93 questions across 6 categories: select a topic above to explore
Further Reading
How to Talk to Your Doctor About Hyperbaric Oxygen Therapy: A Step-by-Step Guide for Canadian Patients
TL;DR: If you think hyperbaric oxygen therapy (HBOT) might help you, the most reliable first step is an…
HBOT, Oxygen Toxicity and Seizure Risk: A Safety Screening Guide for Canadian Referring Physicians
TL;DR: Hyperbaric oxygen therapy (HBOT) is well tolerated by most patients, and the only absolute contraindication is an…
How Many Hyperbaric Oxygen Therapy Sessions Are Needed? A Patient FAQ for Canadians
TL;DR: Most people need a course of hyperbaric oxygen therapy (HBOT), not a single visit. The number of…
How to Prevent and Manage Middle Ear Barotrauma in Your Hyperbaric Clinic: A Protocol Guide for Canadian Clinic Owners
TL;DR: Middle ear barotrauma is the most common side effect of hyperbaric oxygen therapy, and most cases are…