Delayed Radiation Injury (Soft Tissue and Bony Necrosis) and HBOT
Hyperbaric oxygen therapy promotes permanent new blood-vessel growth in radiation-damaged tissue, partially reversing the progressive vascular failure that drives osteoradionecrosis, radiation cystitis, radiation proctitis, soft-tissue necrosis, and brain radiation injury. It is one of the best-evidenced and most-prescribed non-emergency hyperbaric indications in Canada and is recognised by Health Canada as one of the 14 conditions for which provincial health insurance covers HBOT at hospital-based programmes.
Quick Answer
Does HBOT help delayed radiation injury (soft tissue and bony necrosis)? Hyperbaric oxygen therapy promotes permanent new blood-vessel growth in radiation-damaged tissue, partially reversing the progressive vascular failure that drives osteoradionecrosis, radiation cystitis, radiation proctitis, soft-tissue necrosis, and brain radiation injury. It is one of the best-evidenced and most-prescribed non-emergency hyperbaric indications in Canada and is recognised by Health Canada as one of the 14 conditions for which provincial health insurance covers HBOT at hospital-based programmes.
What Is Delayed Radiation Injury (Soft Tissue and Bony Necrosis)?
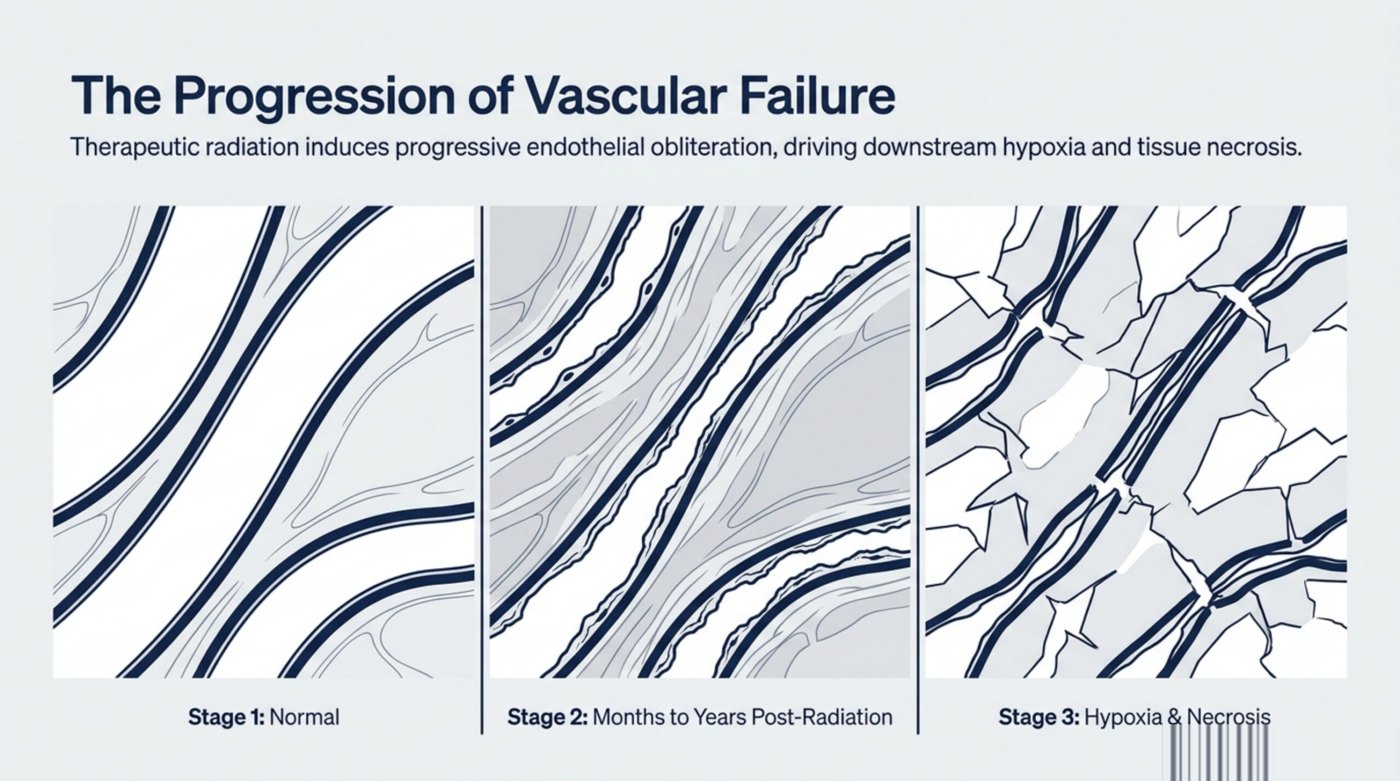
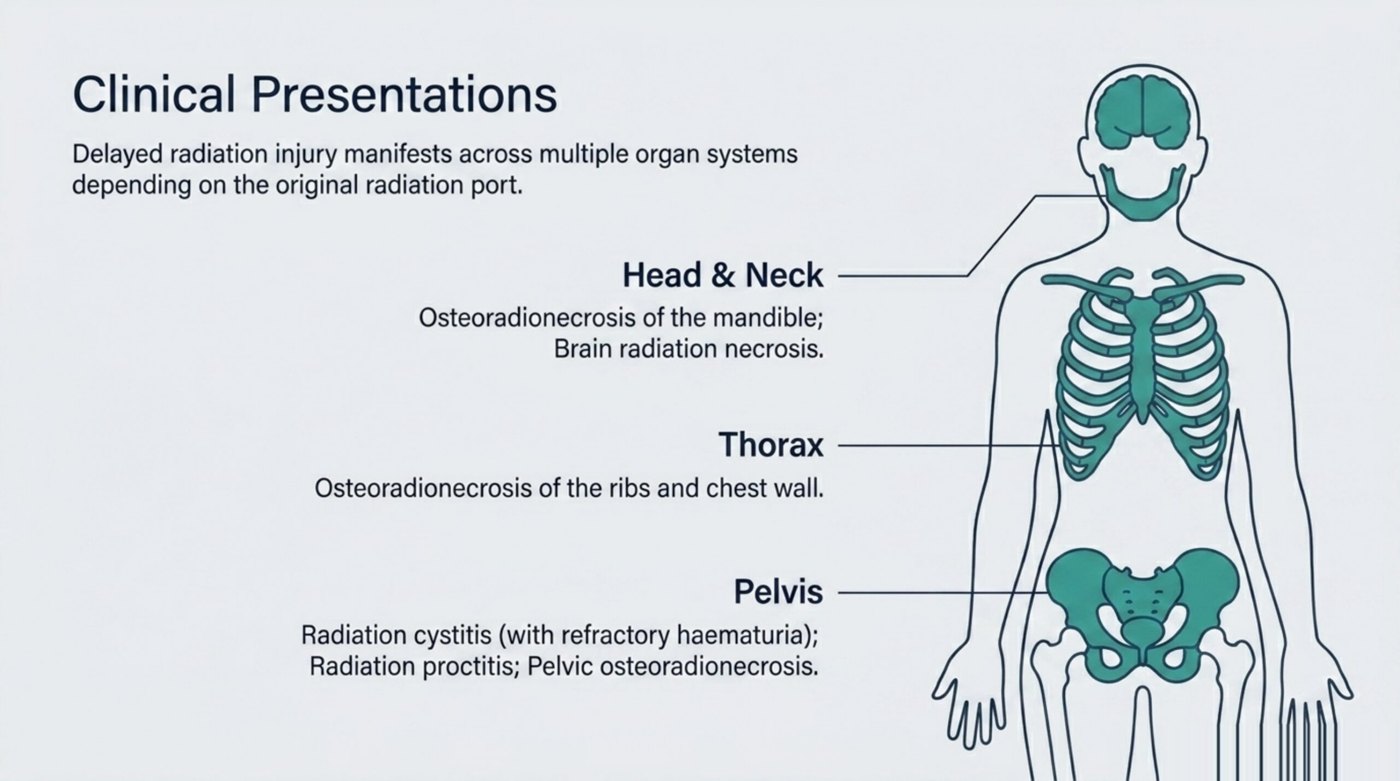
Delayed radiation injury is the umbrella term for chronic tissue damage that develops months to years after radiation therapy for cancer. Modern radiation oncology is highly precise, but every therapeutic dose still affects normal tissue inside the treatment field. Over time, the small blood vessels in that field undergo progressive endothelial damage, narrowing, and obliteration. The tissue downstream of those failing vessels becomes hypoxic, fibrotic, and eventually necrotic. The clinical picture depends entirely on which organ was inside the radiation port, but the underlying vascular pathology is the same.
The most-treated presentations in Canadian hyperbaric programmes are osteoradionecrosis of the mandible (the leading single category, after head-and-neck radiation for oral, oropharyngeal, or laryngeal cancers), radiation cystitis with refractory hematuria (after pelvic radiation for prostate, cervical, or bladder cancer), radiation proctitis with rectal bleeding or pain (after pelvic radiation), osteoradionecrosis of the ribs and chest wall (after thoracic or breast-cancer radiation), osteoradionecrosis of the pelvis (after gynaecologic, prostate, or rectal radiation), brain radiation necrosis (after radiation for primary or metastatic brain tumours), and soft-tissue radiation necrosis with non-healing ulceration in any irradiated field.
Delayed radiation injury affects approximately 5 to 15 percent of patients who receive curative-intent radiation, and the incidence is climbing as cancer survival rates improve and patients live long enough to manifest the late vascular failure. The injuries are progressive without intervention, often debilitating, and historically were managed with palliative measures and salvage surgery. Hyperbaric oxygen therapy, supported by Marx's mandibular work in the 1980s and a sustained body of randomised evidence in the decades since, is one of the few treatments that can address the underlying vascular pathology rather than just managing symptoms.
How HBOT Helps
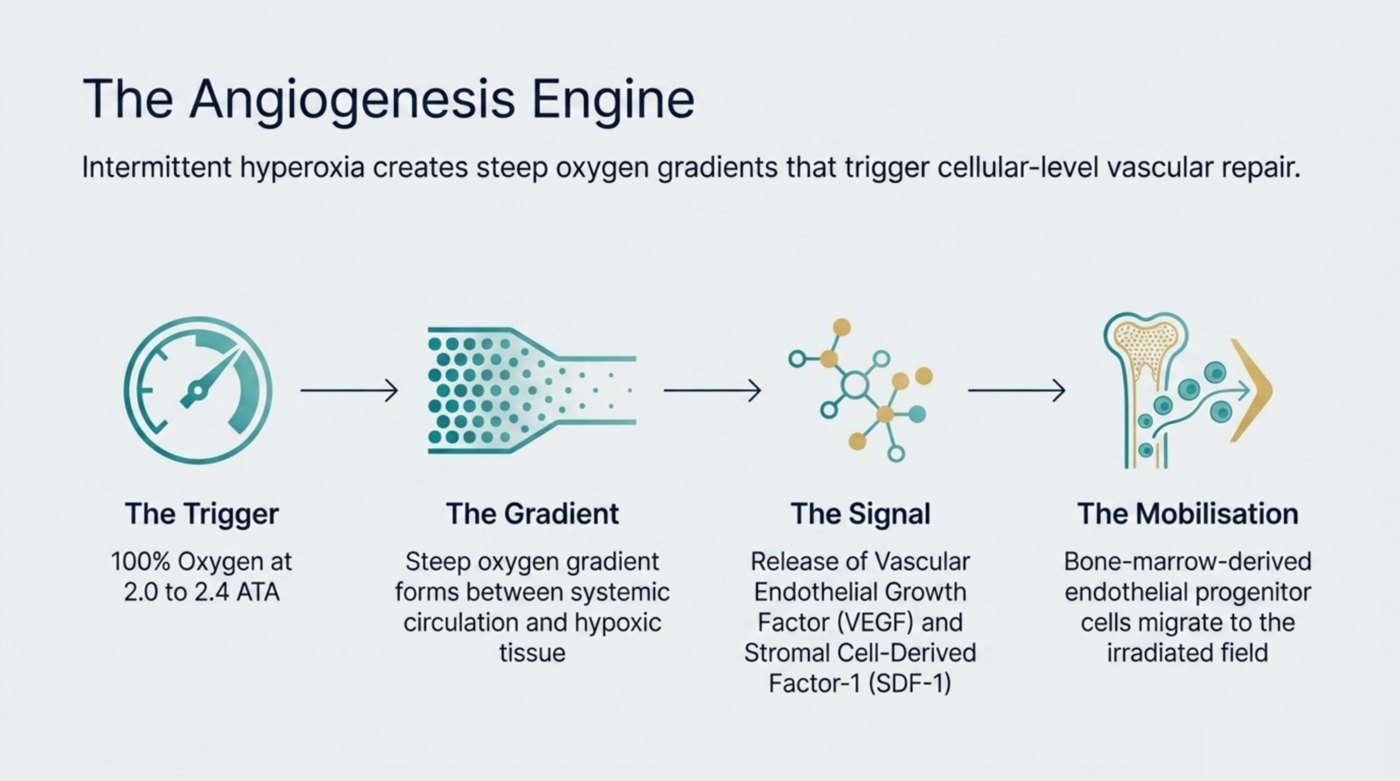
Hyperbaric oxygen therapy treats radiation injury by stimulating angiogenesis, the growth of new blood vessels in the irradiated tissue. The biology is grounded in Marx's foundational work: irradiated tissue retains the cellular machinery for new vessel formation, but the trigger for that machinery (a sustained, large oxygen gradient between the tissue and the systemic circulation) is missing because the existing vessels are too few and too narrow. Repeated intermittent hyperoxia at 2.0 to 2.4 ATA on 100 percent oxygen creates exactly that gradient. Vascular endothelial growth factor (VEGF), stromal cell-derived factor-1 (SDF-1), and other pro-angiogenic signals rise during and after each session, recruiting bone-marrow-derived endothelial progenitor cells to the irradiated field.
Over a course of 20 to 30 daily sessions, capillary density at the irradiated site increases substantially. Marx's classic histology series in irradiated mandibles showed vascular density rising from approximately 20 to 25 percent of non-irradiated bone before treatment to approximately 75 to 80 percent after a full HBOT course, with the new vessels persisting on biopsy years later. This permanent neovascularisation is the central rationale for HBOT in radiation injury, and it explains why benefit is sustained beyond the end of the treatment course rather than disappearing when the chamber sessions stop.
In parallel with angiogenesis, HBOT supports collagen synthesis, restores oxygen-dependent neutrophil bacterial killing in tissue prone to chronic infection, enhances the activity of certain antibiotics in hypoxic bone (notably aminoglycosides and fluoroquinolones, which are oxygen-dependent for tissue uptake), and modulates the chronic inflammatory cascade that drives radiation-induced fibrosis. For osteoradionecrosis specifically, HBOT supports both osteoblast activity (new bone formation) and osteoclast activity (controlled removal of dead bone), allowing the bone-remodelling machinery to resume function in tissue that had stalled in a state of chronic inflammation and necrosis.
Typical Treatment Protocol
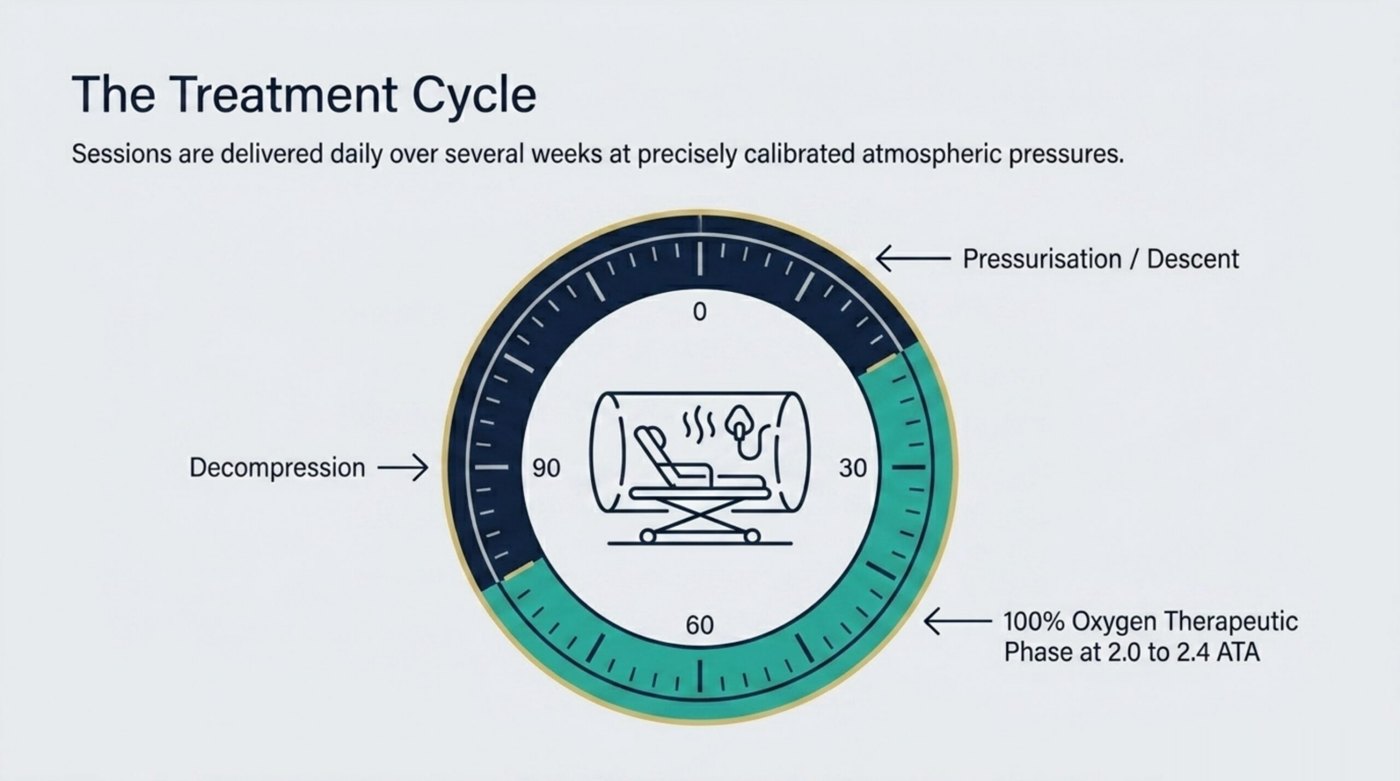
Standard course is 2.0 to 2.4 ATA for 90 minutes per session, delivered five days per week. The total number of sessions depends on the clinical pattern. For established osteoradionecrosis of the mandible, the Marx protocol delivers 30 sessions before any planned surgery, then 10 additional sessions afterward (the so-called "30-and-10" approach), with the option of further courses if response is incomplete. For prophylactic use before dental extractions or implant placement in a previously irradiated jaw, the Marx protocol delivers 20 pre-operative and 10 post-operative sessions. For radiation cystitis or proctitis, 30 to 60 sessions is the typical range, with response measured by symptom improvement, bleeding cessation, and (where applicable) cystoscopic or endoscopic findings. For brain radiation necrosis, 30 to 60 sessions is standard, often combined with corticosteroids and bevacizumab. For non-mandibular osteoradionecrosis (ribs, pelvis, skull) and soft-tissue radionecrosis, 30 to 40 sessions is typical, with extension to 60 if response continues but is incomplete at the first reassessment.
Evidence Summary
Level A - Strong Evidence
Supported by high-quality RCTs and systematic reviews
Key Research Findings
-
The Marx protocol (Marx 1983, J Oral Maxillofac Surg, the foundational work) established HBOT as the standard of care for prevention of osteoradionecrosis before dental work in irradiated jaws. The 30-and-10 protocol (30 pre-operative sessions and 10 post-operative) and the 20-and-10 prophylactic protocol remain the two most widely used HBOT regimens in Canadian hospital programmes today.
-
Marx histology series demonstrated that vascular density in irradiated mandibles rose from approximately 20 to 25 percent of normal before HBOT to approximately 75 to 80 percent after a full course, with the new vessels persisting on biopsy years later. This is the strongest mechanistic evidence for the permanent-neovascularisation rationale for HBOT in radiation injury.
-
Multiple randomised and observational studies show HBOT significantly improves symptoms in radiation cystitis. The RICH-ART trial (Oscarsson et al, Lancet Oncology 2019, 79 patients with late radiation cystitis randomised across five Nordic university hospitals) showed a 10.1-point absolute improvement in the EPIC urinary total score at six-to-eight months in the HBOT group compared with standard care (95% CI 2.2 to 18.1; p=0.013), with HBOT delivered at 240 to 250 kPa for 80 to 90 minutes per session over 30 to 40 sessions.
-
The Clarke et al. RCT (Clarke 2008, IJROBP, 120 evaluable patients with refractory radiation proctitis) and the Sidik et al. RCT (2007, Acta Med Indones, 65 patients) showed significant symptom improvement with HBOT for radiation proctitis. The UK Glover et al. HOT2 RCT (2016, Lancet Oncology, PMID 26703894) examined HBOT for chronic bowel dysfunction after pelvic radiotherapy and did not show overall benefit, providing important counter-evidence that informs current Canadian referral practice.
-
A Cochrane Review of HBOT for late radiation tissue injury (Bennett 2016, 14 RCTs and 753 participants, updated by Lin and Bennett in 2023 to 18 studies and 1,071 participants) concluded that HBOT improves outcomes in osteoradionecrosis of the mandible, radiation proctitis, and radiation cystitis, and is associated with improved wound healing in irradiated tissue. The review noted heterogeneity in protocols across trials and called for standardised reporting.
-
No clinical evidence demonstrates that HBOT promotes cancer growth or recurrence, and the UHMS position statement explicitly endorses HBOT as safe for cancer survivors. Several large registry studies have failed to find any signal of increased recurrence risk in irradiated cancer survivors who received HBOT for late radiation injury.
-
Brain radiation necrosis evidence remains more limited than for the bone and pelvic indications, but combined HBOT plus bevacizumab plus corticosteroid protocols have shown radiographic and clinical improvement in published case series. The Princess Margaret Cancer Centre / UHN in Toronto is among the leading Canadian programmes investigating this combination.
-
Key supporting studies in the Canada Hyperbarics research database: PMID 41627499, PMID 41223393, PMID 40259026.
Top studies in our database
Highest-evidence-tier studies tagged to this condition in the Canada Hyperbarics research database, ranked by evidence tier (1 = meta-analysis or RCT, 2 = cohort, 3 = case series), most recent first.
-
Tier 1Systematic Review of Hyperbaric Oxygen for Late Radiation Tissue Injury (Bowel, Bladder)
Undersea Hyperb Med · 2025 · Systematic Review
-
Tier 1
-
Tier 1Treatment approaches in cases of mandibular osteoradionecrosis: A systematic meta-analysis
J Stomatol Oral Maxillofac Surg · 2025 · Meta-Analysis
-
Tier 1Presentation and Optimal Management of Anterior and Central Skull Base Osteoradionecrosis: Systematic Review and Meta-Analysis
Laryngoscope · 2025 · Meta-Analysis
-
Tier 1Hyperbaric oxygen therapy for late radiation tissue toxicity injury after head and neck cancer: a systematic review of the literature
Radiat Oncol · 2025 · Systematic Review
Registered trials (ClinicalTrials.gov)
Studies in our database that include a ClinicalTrials.gov registration. Trial registration is a marker of methodological rigour because the protocol, primary outcome, and analysis plan are deposited before enrolment begins.
-
Radiation-induced cystitis treated with hyperbaric oxygen therapy (RICH-ART): long-term follow-up of a randomised controlled, phase 2-3 trial.
EClinicalMedicine · 2025 · RCT · PMID 40291346
-
Efficacy and safety of hyperbaric oxygen therapy for radiation-induced dermatitis in patients with breast cancer: a randomized pilot study
Support Care Cancer · 2025 · RCT · PMID 40259026
-
Hyperbaric oxygen therapy and late local toxic effects in patients with irradiated breast cancer: the HONEY randomized clinical trial
JAMA Oncol · 2024 · RCT · PMID 38329746
-
Symptom burden and health-related quality of life six months after hyperbaric oxygen therapy in cancer survivors with pelvic radiation injuries.
Supportive care in cancer : official journal of the Multinational Association of Supportive Care in Cancer · 2022 · Clinical Study · PMID 35320424
-
The impact of hyperbaric oxygen therapy on late radiation toxicity and quality of life in breast cancer patients.
Breast cancer research and treatment · 2021 · Clinical Study · PMID 34279734
Active Canadian Trials
The following hyperbaric oxygen trials related to delayed radiation injury (soft tissue and bony necrosis) are currently recruiting or active at Canadian sites. Data is pulled live from ClinicalTrials.gov (refreshed every 24 hours). Speak with your physician about whether you might be eligible.
-
Sponsor: Sunnybrook Health Sciences Centre · Phase: PHASE3 · Canadian site: Toronto, Ontario
Data source: ClinicalTrials.gov. Trial status updates daily. Eligibility, exclusion criteria, and consent should be discussed with your physician and the trial's principal investigator.
What to Expect from Treatment
Most patients are referred to a hospital hyperbaric programme by their cancer-care team, dental surgeon, urologist, or wound-care specialist after a definitive diagnosis of radiation injury, often supported by imaging (orthopantomogram or CT for bone, cystoscopy for bladder, endoscopy for bowel) and biopsy where infection or recurrence needs to be excluded. The hyperbaric medicine team confirms eligibility (the diagnosis, the radiation history, the absence of active recurrent malignancy in the planned treatment field, and the absence of absolute contraindications), reviews the planned protocol, and books the treatment course. Many programmes also coordinate dental clearance, surgical timing, and oncology follow-up at this stage.
Daily sessions begin within one to four weeks of consultation, with timing often driven by surgical scheduling for prophylactic Marx-protocol cases. You change into cotton scrubs (no synthetic fabrics, no skin lotions, no jewellery), enter the chamber, breathe pure oxygen during the 90-minute treatment phase, and decompress back to surface pressure. Most programmes deliver in monoplace chambers (one patient at a time, you lie on a stretcher) or multiplace chambers (multiple patients in a shared chamber, you sit in a recliner and breathe oxygen by hood or mask). Total time on-site is typically two to three hours per visit including check-in.
Response is measured periodically against the clinical endpoint that prompted the referral. Mandibular osteoradionecrosis cases are reassessed by the dental surgeon at the midpoint and at completion, with imaging where indicated. Radiation cystitis is followed by symptom diary and, where bleeding was the presenting issue, by haemoglobin and transfusion-frequency tracking. Brain radiation necrosis is followed by serial MRI and neurocognitive assessment. Most patients tolerate the full course well; common side effects are temporary near-sightedness during treatment (usually resolves within a few weeks of stopping), ear barotrauma (managed with pressure-equalisation techniques), and mild fatigue.
Accessing HBOT for Delayed Radiation Injury (Soft Tissue and Bony Necrosis) in Canada
Delayed radiation injury is one of the most-referred non-emergency hyperbaric indications in Canada and is covered by every provincial health-insurance plan at hospital-based programmes. In Ontario, OHIP covers treatment at the three hospital programmes (Toronto General / UHN, Hamilton General Hospital, The Ottawa Hospital). The Princess Margaret Cancer Centre / UHN is the leading Canadian centre for HBOT research in radiation injury, particularly brain radiation necrosis. Select eligible Independent Health Facilities may also bill OHIP for approved indications, with eligibility varying by facility and indication. Confirm directly with the IHF before booking.
Alberta Health (AHCIP) covers treatment at the two hospital programmes: Misericordia Community Hospital in Edmonton (operated by Covenant Health) and the Foothills Medical Centre / Arthur J.E. Child Comprehensive Cancer Centre in Calgary (operated by Alberta Health Services). The Alberta hospital billing code for HBOT detention time is 13.99I (per 15 minutes). CPSA accreditation of private hyperbaric clinics is a safety and quality standard; CPSA accreditation alone does not grant Alberta Health billing eligibility for radiation-injury HBOT.
British Columbia (MSP) covers treatment at Vancouver General Hospital's Leon Judah Blackmore Pavilion. Quebec (RAMQ) covers treatment at Hôpital du Sacré-Cœur de Montréal and Hôtel-Dieu de Lévis. Nova Scotia (MSI) and Newfoundland and Labrador (MCP) also cover hospital-delivered radiation-injury treatment. Saskatchewan Health covers the indication in principle, but the province's only hospital chamber (Dr. F.H. Wigmore Regional Hospital, Moose Jaw) has had disrupted, reduced availability since a July 2021 staffing closure, so confirm current in-province capacity before relying on it.
For patients in provinces or territories without an in-province hospital programme (Manitoba, New Brunswick, Prince Edward Island, Yukon, Northwest Territories, Nunavut), publicly funded HBOT is accessed through inter-provincial referral coordinated by the family physician, oncologist, or surgeon. Inter-provincial billing arrangements typically cover the medically necessary treatment cost; travel and accommodation for the four to eight weeks of daily sessions are usually the patient's responsibility unless the home province operates a medical-travel assistance programme. Some programmes coordinate with provincial cancer-care navigators and patient-support charities for assistance with travel logistics.
Provincial Access for Delayed Radiation Injury (Soft Tissue and Bony Necrosis)
Hyperbaric oxygen therapy for the 14 Health Canada-recognised conditions, including Delayed Radiation Injury (Soft Tissue and Bony Necrosis), is delivered at the 11 hospital hyperbaric programmes located in seven provinces (Ontario, Quebec, British Columbia, Alberta, Nova Scotia, Newfoundland and Labrador, and Saskatchewan). The six provinces and territories without an in-province hospital programme (Manitoba, New Brunswick, Prince Edward Island, Yukon, Northwest Territories, and Nunavut) route patients to the nearest receiving hospital programme. Use the links below for province-specific coverage, referral pathway, and emergency routing details.
Hospital + Private
OHIP (Ontario Health Insurance Plan)
Hospital Only
MSP (Medical Services Plan)
Hospital + Private
Alberta Health / AHCIP
Hospital Only
RAMQ
Disrupted
Saskatchewan Health Authority
No Hospital Chamber
Manitoba Health
Hospital Only
MSI (Medical Services Insurance)
No Hospital Chamber
Medicare NB
Hospital Only
MCP (Medical Care Plan)
Out-of-Province Referral
Health PEI
Out-of-Province Referral
Yukon Health and Social Services
Out-of-Province Referral
NWT Health and Social Services
Out-of-Province Referral
Nunavut Department of Health
For acute or emergency presentations of Delayed Radiation Injury (Soft Tissue and Bony Necrosis), call 911 first. The receiving emergency department coordinates urgent transfer to the nearest hospital hyperbaric programme through the relevant provincial transfer network (CritiCall Ontario at 1-800-668-4357, BC Patient Transfer Network, EHS Nova Scotia, or equivalent). For diving-related emergencies, the Divers Alert Network (DAN) emergency hotline is 1-919-684-9111.
Risks and Contraindications
Absolute contraindications to HBOT include untreated pneumothorax (because trapped intrathoracic air expands on decompression and can cause tension pneumothorax), concurrent bleomycin chemotherapy (because hyperbaric oxygen can trigger or accelerate oxygen-induced pulmonary fibrosis), and concurrent disulfiram (because it inhibits superoxide dismutase, the enzyme that neutralises hyperbaric-oxygen-generated free radicals). Prior bleomycin exposure with documented pulmonary clearance is a relative contraindication that requires individualised pulmonary-function review before HBOT. Active recurrent malignancy in the planned treatment field is a relative contraindication; while no clinical evidence demonstrates that HBOT promotes cancer growth, most Canadian programmes prefer to confirm absence of recurrence before committing to a long course of treatment, particularly for mandibular and brain radiation injury where biopsy is feasible. Relative contraindications, weighed against expected benefit on a per-patient basis, include severe chronic obstructive pulmonary disease with bullous lung disease, uncontrolled seizure disorder, claustrophobia (manageable in monoplace chambers and with behavioural strategies), recent middle-ear or sinus surgery, and uncontrolled hypertension. Cardiac function should be assessed in patients with congestive heart failure because the increase in plasma oxygen content can transiently increase left-ventricular afterload. Patients with active intracranial recurrence and elevated intracranial pressure require neurosurgical clearance before HBOT for brain radiation necrosis.
Frequently Asked Questions
Delayed radiation injury typically appears 6 months to several years after radiation therapy. Some patients develop symptoms decades after treatment. The risk increases over time as radiation-damaged blood vessels progressively fail. Mandibular osteoradionecrosis often presents 6 to 24 months after radiation, frequently triggered by a dental extraction in an irradiated jaw. Radiation cystitis and proctitis often present 12 to 36 months after pelvic radiation. Soft-tissue and chest-wall radionecrosis can appear at any point but most commonly 1 to 5 years after treatment.
HBOT promotes permanent neovascularisation in irradiated tissue, which can reverse or halt the progression of radiation damage. Many patients experience significant improvement; complete resolution depends on the severity and location of the injury. Mandibular osteoradionecrosis and radiation cystitis have the highest published response rates. Brain radiation necrosis and severe soft-tissue radionecrosis tend to have more variable responses, often requiring combined HBOT plus medical therapy.
Yes, at hospital-based hyperbaric programmes under provincial health insurance. OHIP covers treatment at the three Ontario hospital programmes (Toronto General, Hamilton General, The Ottawa Hospital), with select eligible IHFs also able to bill OHIP for approved indications. Alberta Health (code 13.99I) covers treatment at Misericordia Edmonton and Foothills/AJECCC Calgary. MSP covers Vancouver General Hospital. RAMQ covers the two Quebec hospital programmes. MSI, MCP, and Saskatchewan Health each cover their respective hospital programmes. Private clinic treatment is typically self-pay.
There is no clinical evidence that HBOT promotes cancer growth or recurrence. Multiple cohort studies and the UHMS position statement confirm that HBOT is safe for cancer survivors. Active recurrent malignancy in the planned treatment field is a relative contraindication, and most Canadian programmes confirm absence of recurrence before starting a long HBOT course, but a remote history of cancer is not a barrier to treatment.
Yes. Osteoradionecrosis of the ribs and chest wall is a recognised late effect of thoracic radiation (commonly seen after breast cancer, lung cancer, or chest-wall radiation) and is one of the indications for which Canadian hospital hyperbaric programmes accept referrals. Standard treatment is 30 to 40 daily sessions at 2.0 to 2.4 ATA, each lasting 90 minutes, with an additional 10 sessions if surgical resection of necrotic bone is planned (Marx-protocol approach extended to non-mandibular bone). Treatment is covered by OHIP, RAMQ, MSP, AHCIP, MSI, MCP, and Saskatchewan Health at hospital programmes with a physician referral. Symptoms that should prompt referral include localised chest-wall pain in a previously irradiated field, palpable bony irregularity, draining sinuses, or pathological rib fracture.
Yes, radiation cystitis is a recognised late effect of pelvic radiation for prostate cancer (and for gynaecologic, bladder, and rectal cancers). Hematuria, often refractory to standard urological measures, is the most common presenting symptom. HBOT is well-evidenced for radiation cystitis, with consistent improvement reported in randomised and observational data. The RICH-ART trial (Oscarsson et al, Lancet Oncology 2019), a multi-centre Nordic randomised trial of 79 patients with late radiation cystitis, showed a statistically significant improvement in patient-reported urinary symptoms (EPIC urinary score) at six-to-eight months in the HBOT group compared with standard care. Standard course is 30 to 60 sessions. Speak with your urologist about referral to a hospital hyperbaric programme.
The Marx protocol is a prophylactic HBOT regimen designed to reduce the risk of osteoradionecrosis (ORN) when dental extractions or implant placement are needed in a previously irradiated jaw. The standard regimen is 20 HBOT sessions before the planned dental procedure and 10 sessions afterward, each at 2.0 to 2.4 ATA for 90 minutes. The pre-operative sessions stimulate angiogenesis to support healing of the extraction socket; the post-operative sessions support continued vascularisation during the critical healing window. The protocol was established by Marx in 1983 and remains the standard prophylactic regimen at Canadian hospital hyperbaric programmes today. Coverage is provincial.
Yes. Radiation proctitis with rectal bleeding, pain, or tenesmus is a recognised HBOT indication and has been studied in randomised trials. Clarke 2008 (IJROBP) and Sidik 2007 (Acta Med Indones) reported significant symptom improvement with HBOT, while the UK Glover 2016 HOT2 RCT (Lancet Oncology) did not show overall benefit for chronic bowel dysfunction after pelvic radiotherapy. Standard course is 30 to 60 sessions at 2.0 to 2.4 ATA for 90 minutes. Most patients see measurable improvement in bleeding and pain by the midpoint. Endoscopic reassessment is used to confirm mucosal healing in cases where bleeding was the presenting issue.
Brain radiation necrosis (also called radiation-induced leukoencephalopathy) is a recognised HBOT indication, although the evidence base is more limited than for mandibular ORN, radiation cystitis, or radiation proctitis. Most published case series describe HBOT used in combination with corticosteroids and bevacizumab. The Princess Margaret Cancer Centre / UHN in Toronto is among the leading Canadian centres investigating this combination. Standard HBOT course is 30 to 60 sessions. Speak with your neuro-oncologist or radiation oncologist about referral.
You change into cotton scrubs, enter the chamber, and lie down (in a monoplace chamber) or sit in a recliner (in a multiplace chamber with multiple patients). Pressurisation takes five to ten minutes and feels like the descent in an aircraft. Most people clear their ears with the same technique used in flying. During the 90-minute treatment phase you breathe pure oxygen, often through a hood or mask, while reading, watching a screen, or sleeping. Decompression takes another five to ten minutes. The most common sensation during a session is a feeling of warmth.
The most common side effect is ear barotrauma during pressurisation, which is managed with pressure-equalisation techniques and resolves between sessions. Other relatively common effects are temporary near-sightedness (myopia) during the course (vision usually returns to baseline within a few weeks of stopping), fatigue, and rare confinement anxiety. Serious complications including pneumothorax, oxygen toxicity seizures, and cardiac decompensation are uncommon at the standard 2.0 to 2.4 ATA pressures used for radiation injury.
For osteoradionecrosis of the mandible, the standard Marx protocol delivers 30 sessions before any planned surgery and 10 sessions afterward (the 30-and-10 approach), with the option of further courses if response is incomplete. For prophylactic dental work in irradiated jaws, the protocol is 20 sessions before and 10 after (the 20-and-10 approach). For radiation cystitis, proctitis, or non-mandibular osteoradionecrosis, 30 to 60 sessions is the typical range. Daily sessions over 6 to 12 weeks is the practical reality for most patients.
Yes, this is one of the central mechanistic findings underpinning the use of HBOT for radiation injury. Marx demonstrated in histology series in irradiated mandibles that the new capillary network created during a 20 to 30 session course persists on biopsy years after treatment. This permanent neovascularisation is why HBOT can produce sustained improvement in radiation-injured tissue rather than just a temporary effect during the chamber sessions.
Speak with your oncology team, radiation oncologist, dental surgeon (for mandibular cases), urologist (for cystitis), gastroenterologist (for proctitis), or wound-care specialist. Document the radiation history (dose, fractionation, treatment field), the diagnosis (with imaging or endoscopy as appropriate), and the absence of active recurrent malignancy in the planned field. The referring physician sends a request to the nearest hospital hyperbaric programme, which typically schedules a consultation within two to six weeks and treatment shortly after if you meet eligibility criteria.
The Canada Hyperbarics verified directory at canadahyperbarics.ca/facilities/ lists all 11 hospital programmes alongside their phone numbers, websites, and current chamber status. Coverage details for every province are at canadahyperbarics.ca/hbot-coverage-canada/. The Princess Margaret Cancer Centre / UHN in Toronto, the Misericordia Edmonton, and Vancouver General Hospital are among the most-referred Canadian programmes for delayed radiation injury.
In Canada, delayed radiation injury is one of the 14 Health Canada-recognised conditions for HBOT, so treatment at hospital-based programmes is covered by provincial health insurance (OHIP, MSP, AHCIP, RAMQ, MSI, Saskatchewan Health, MCP) with a physician referral, at no out-of-pocket cost. The only absolute contraindication to HBOT is untreated pneumothorax (trapped intrathoracic air expands on decompression); concurrent bleomycin chemotherapy (oxygen-induced pulmonary fibrosis risk) and concurrent disulfiram (interferes with superoxide dismutase, the enzyme that neutralises hyperbaric-oxygen-generated free radicals) are treated as effectively absolute at most programmes, though the UHMS classifies them as relative contraindications. Relative contraindications include severe haemodynamic instability requiring continuous high-dose vasopressor titration, uncontrolled seizure disorder, severe COPD with bullous lung disease, and uncontrolled claustrophobia. Pregnancy is not a contraindication.
Related conditions: HBOT for Chondroradionecrosis, HBOT and Glioblastoma in Canada
Latest Articles
Hyperbaric Oxygen Therapy for Radiation Cystitis: A 2026 Evidence Review for Researchers
TL;DR: Radiation cystitis is a chronic bladder injury that affects an estimated 5 to 10 percent of people…
HBOT for Osteoradionecrosis of the Jaw: A 2026 Evidence and Referral Guide for Canadian Physicians
TL;DR: Osteoradionecrosis (ORN) of the jaw is a late complication of head and neck radiotherapy. Hyperbaric oxygen therapy…
Hyperbaric Oxygen Therapy as Adjunctive Cancer Care: A 2024-2026 Evidence Review for Researchers
TL;DR: The 2024-2026 evidence base positions hyperbaric oxygen therapy as a meaningful adjunct in oncology care, not as…
Does HBOT Feed Cancer? Separating the Myth From the Evidence: A Daffodil Month Guide
TL;DR: The fear that hyperbaric oxygen therapy (HBOT) might “feed” cancer comes from a real piece of biology,…