Exceptional blood loss anaemia is a severe drop in red blood cells caused by major bleeding, in a patient who cannot receive a blood transfusion. Hyperbaric oxygen therapy (HBOT) is a recognised supportive treatment for this condition. It works by dissolving extra oxygen directly into the blood plasma, so tissues can keep receiving oxygen even when red blood cell levels are dangerously low.
- Exceptional blood loss anaemia happens when a patient has lost a large amount of blood and cannot get a transfusion, whether by choice, medical necessity, or lack of a matching blood supply.
- HBOT increases the amount of oxygen carried in the blood plasma itself, separate from red blood cells, helping tissues survive a low-haemoglobin crisis.
- This is one of the accepted uses of HBOT recognised by hyperbaric medicine organizations, typically used alongside standard emergency and critical care, not instead of it.
- It is most often used in hospital settings for patients such as Jehovah’s Witnesses who decline transfusion, or people with rare antibodies or blood types.
- This article is educational. Always speak with a physician about whether HBOT is appropriate for a specific medical situation.
What is exceptional blood loss anaemia?
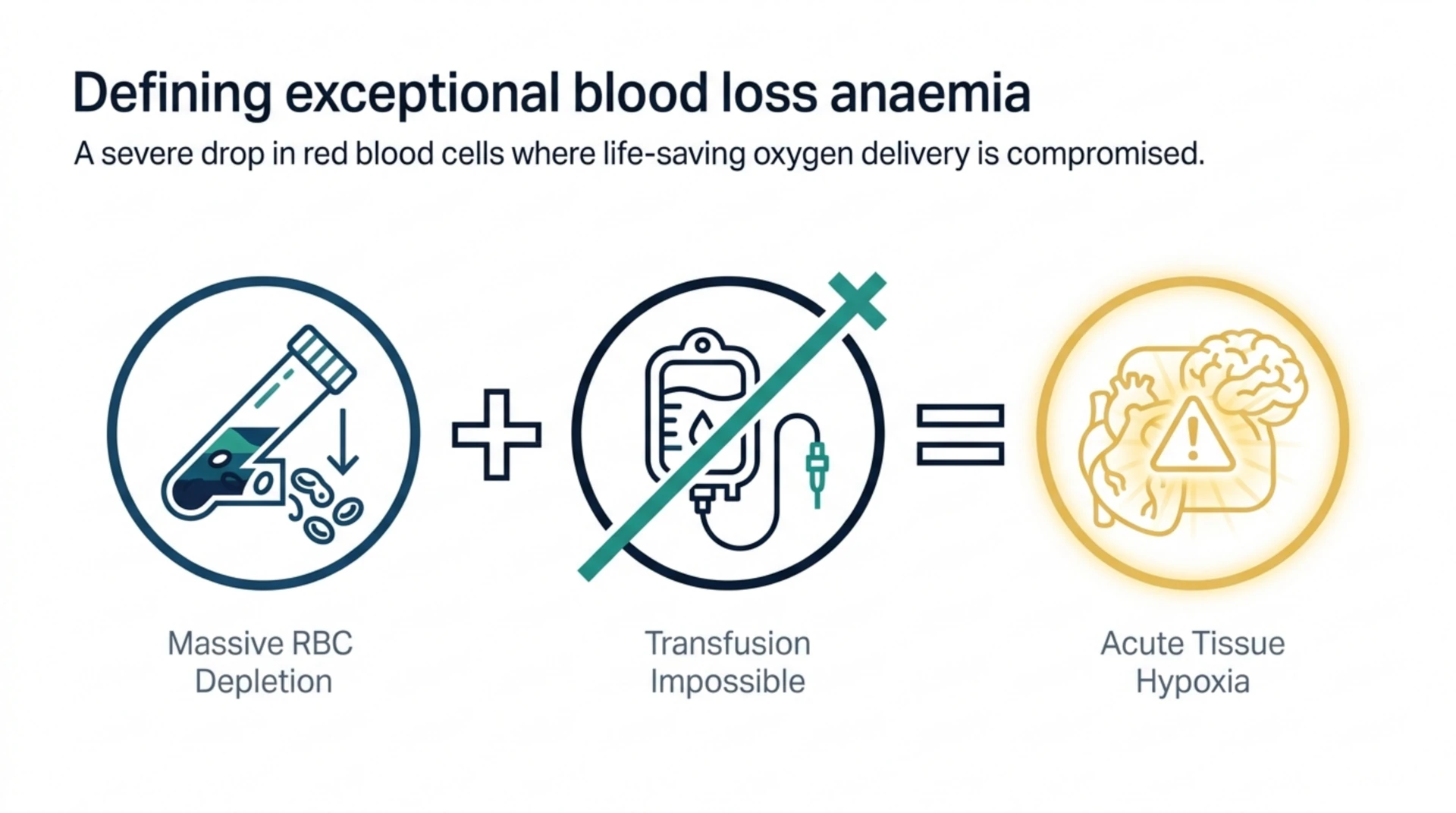
Anaemia means the blood has fewer red blood cells, or less haemoglobin, than normal. Haemoglobin is the protein inside red blood cells that carries oxygen from the lungs to the rest of the body. Exceptional blood loss anaemia is a specific and severe version of this problem. It occurs after major bleeding, from trauma, surgery, or a medical condition, when the patient’s haemoglobin drops to a critically low level and a blood transfusion is not possible.
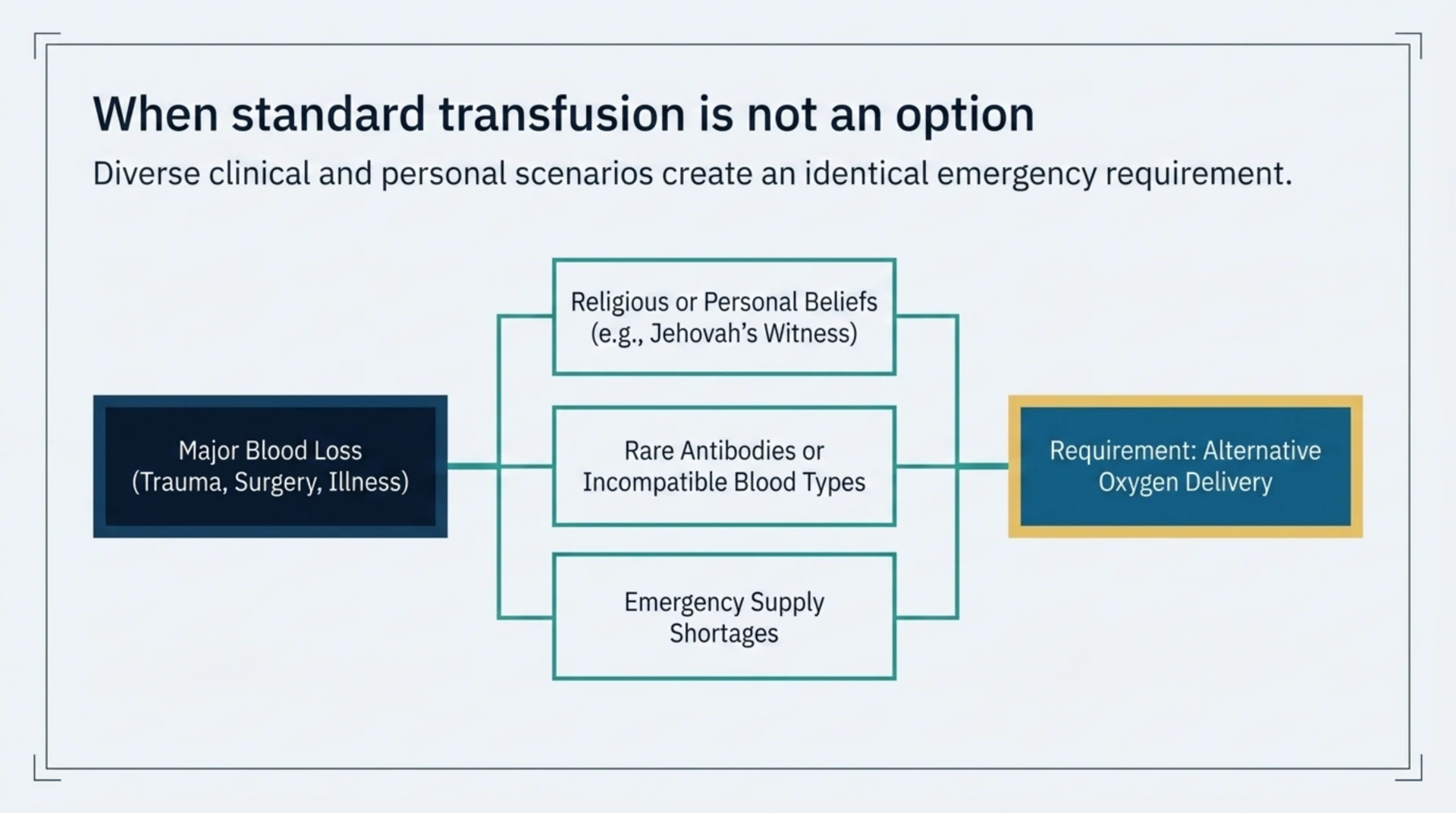
A transfusion might not be possible for a few reasons. Some patients decline transfusion for religious or personal beliefs. Others have rare blood types or antibodies that make it hard to find compatible donor blood. In some emergencies, supply simply is not available quickly enough. Whatever the reason, doctors still need a way to keep the patient’s organs supplied with oxygen while the body rebuilds its own red blood cells, a process that can take days to weeks.
Why does oxygen therapy help when blood transfusion is not an option?
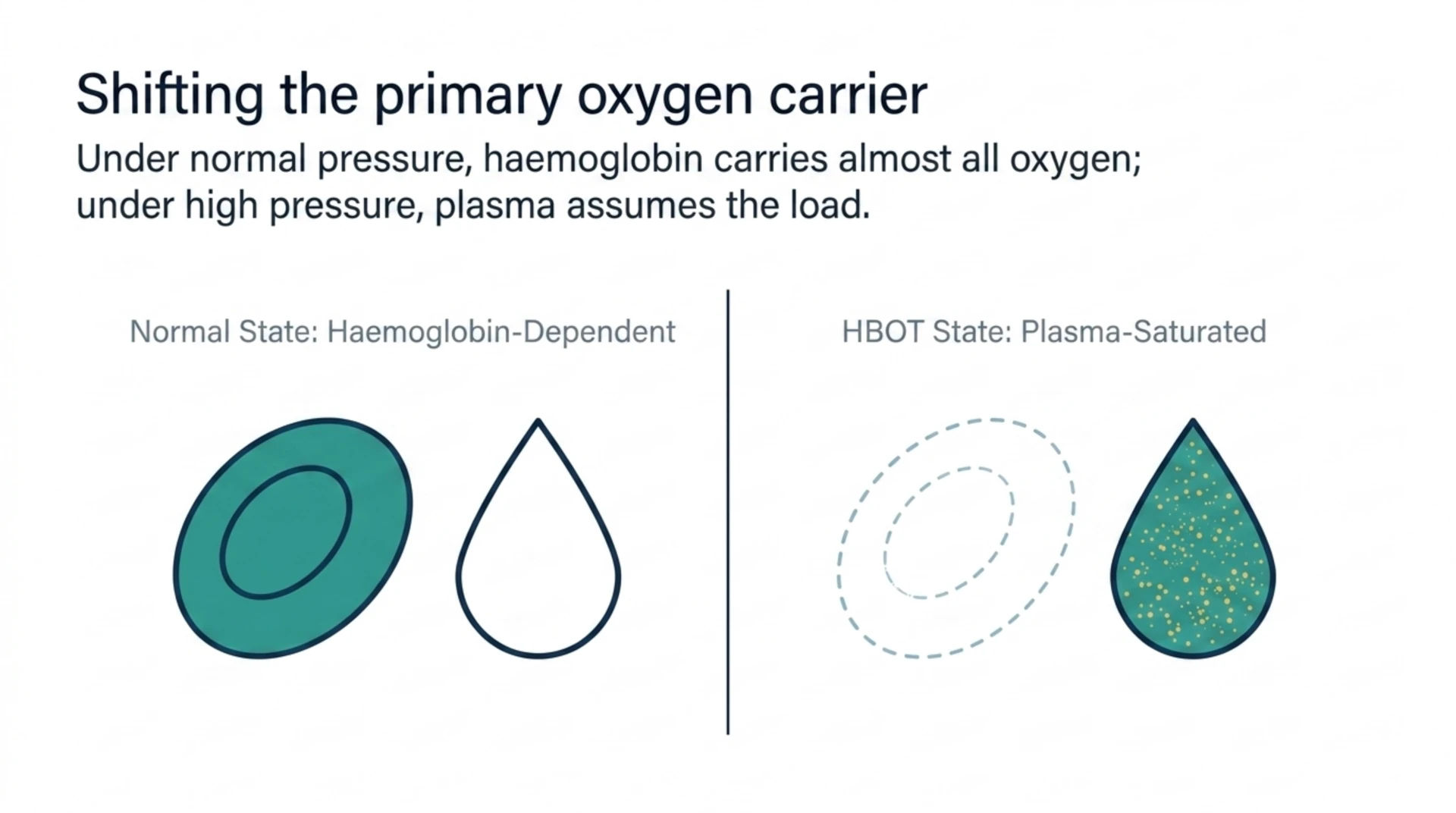
Under normal air pressure, almost all the oxygen in blood is carried by haemoglobin inside red blood cells. Only a tiny amount dissolves directly in the plasma, the liquid part of blood. When a patient has very few red blood cells left, that tiny dissolved amount becomes much more important.
Inside a hyperbaric oxygen chamber, a patient breathes 100 percent oxygen at a pressure greater than normal atmospheric pressure. This dramatically increases the amount of oxygen that dissolves in the plasma, following a well-established principle of gas physics. At high enough pressure, the plasma alone can sometimes carry enough dissolved oxygen to meet the body’s basic needs, even with very few functioning red blood cells. This buys the body time to produce new red blood cells and recover.
How is HBOT used for this condition in practice?
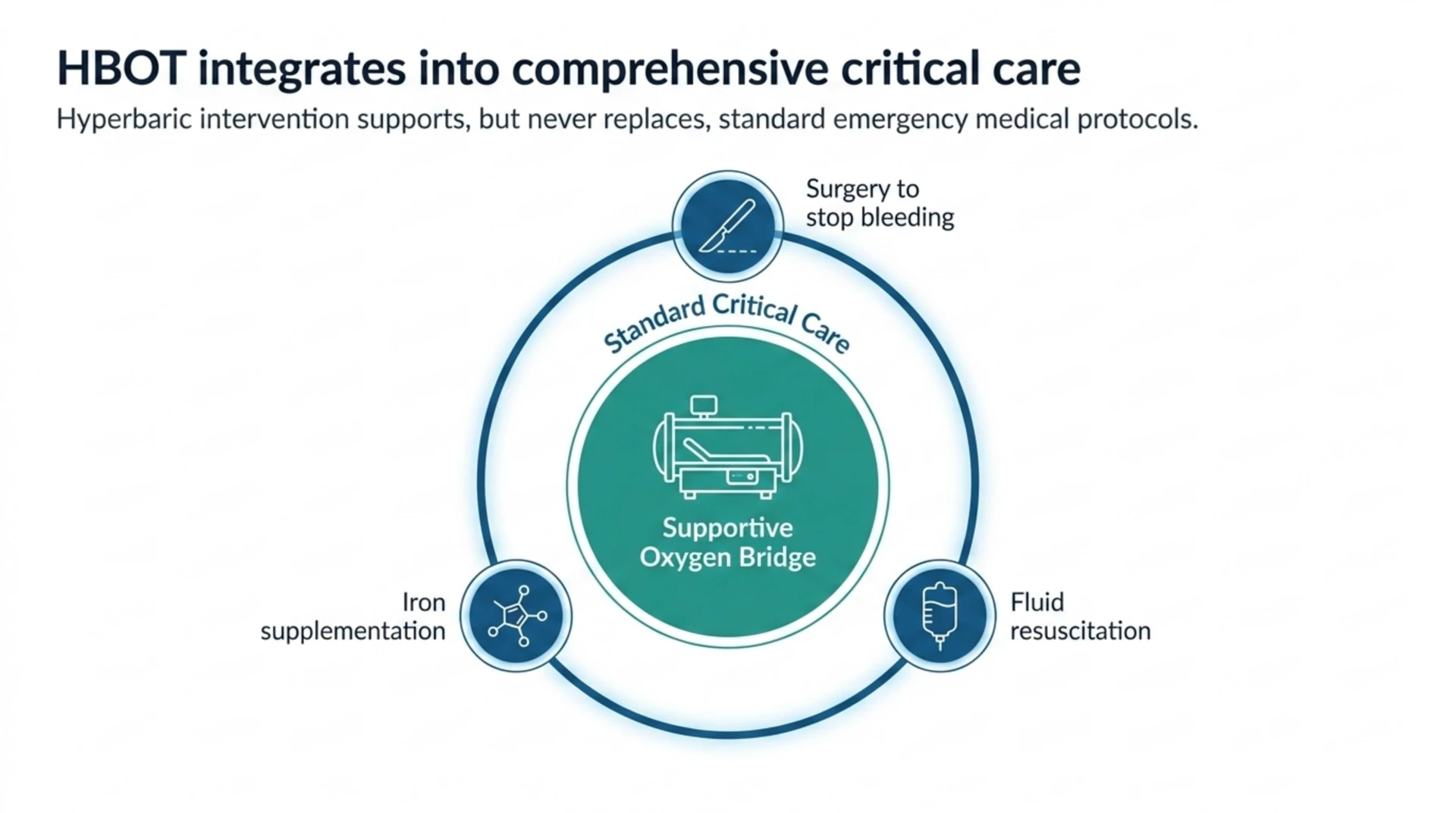
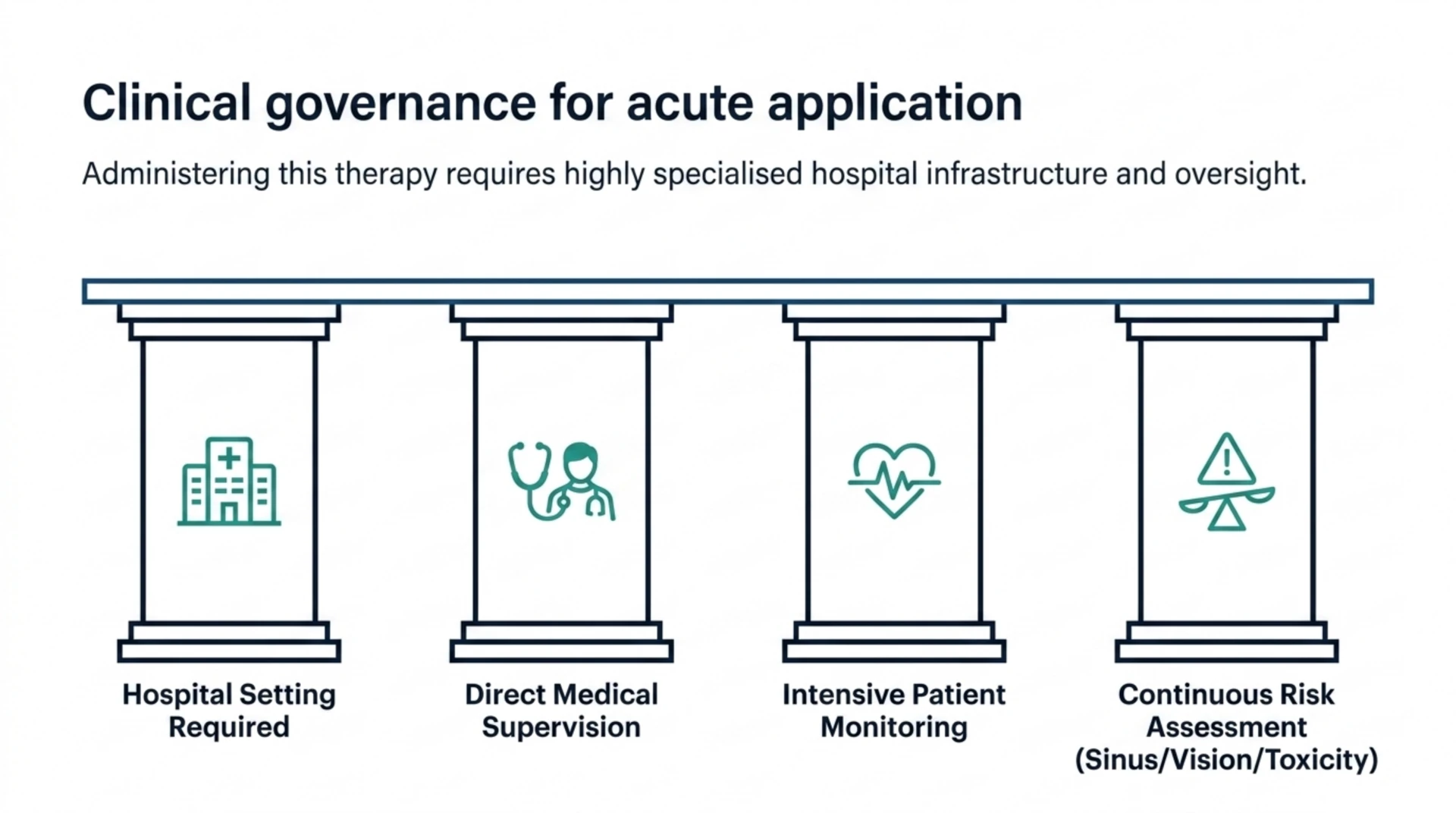
HBOT for exceptional blood loss anaemia is almost always delivered in a hospital setting, as part of a broader critical care plan. It is a supportive therapy, not a replacement for surgery to stop bleeding, fluid resuscitation, iron supplementation, or other standard treatments. A physician monitors the patient closely and decides on the pressure, session length, and number of sessions based on the severity of the anaemia and how the patient responds.
Because this use of HBOT applies to acute, life-threatening situations, it looks different from more routine outpatient hyperbaric treatments. Sessions may be more frequent in the early, most critical period, then taper off as the patient’s own red blood cell count recovers.
| Aspect | Detail |
|---|---|
| Who it applies to | Patients with severe blood loss anaemia who cannot or will not receive a transfusion |
| How it helps | Increases oxygen dissolved directly in blood plasma, independent of red blood cells |
| Setting | Typically hospital-based, alongside standard emergency and critical care |
| Goal | Maintain organ oxygen supply until the body rebuilds its own red blood cells |
| Recognition | Listed as an accepted indication by hyperbaric medicine organizations |
Who typically needs this treatment?
The most commonly discussed group is Jehovah’s Witness patients, whose religious beliefs generally do not permit blood transfusion. Hyperbaric medicine has been used to support these patients through major surgery or trauma when blood loss is significant. Beyond this group, the treatment can apply to anyone with rare blood antibodies, an incompatible blood type in an emergency, or a personal medical reason to avoid transfusion.
It is important to be clear that this is a specific, medically supervised use of HBOT for a defined emergency situation. It is not a general anaemia treatment for common causes like iron deficiency, vitamin deficiency, or chronic disease, which are managed with different, well-established treatments.
Is HBOT safe for this use?
Hyperbaric oxygen therapy is generally considered safe when delivered by trained staff in a properly equipped chamber, with monitoring appropriate to the patient’s condition. As with any medical treatment, there are possible side effects, including ear or sinus pressure discomfort, temporary changes in vision, and, rarely, oxygen toxicity effects. In a critical care setting, the treating medical team weighs these risks against the risk of the anaemia itself, which in exceptional blood loss cases can be life-threatening if untreated.
Patients considering hyperbaric care for any condition should ask their care team about the facility’s equipment, staff training, and monitoring protocols. You can learn more about how a hyperbaric facility should be equipped and staffed on our facilities page.
Where does the evidence stand today?
Exceptional blood loss anaemia is recognised as an accepted indication for hyperbaric oxygen therapy by major hyperbaric medicine organizations, based on decades of clinical experience and the well-understood physiology of dissolved plasma oxygen. As with many emergency and critical care applications, the supporting evidence comes largely from case reports and clinical experience rather than large randomised trials, since it would not be ethical to withhold a potentially life-saving therapy from a critically ill patient to run a controlled study.
This means the treatment is grounded in sound physiological reasoning and real clinical use, while researchers continue to study and refine best practices. Readers interested in the broader research landscape around hyperbaric medicine can visit our research section for more general background on how HBOT is studied and applied.
What should patients and families know?
If you or a family member is facing a situation involving major blood loss and transfusion is not an option, hyperbaric oxygen therapy may be raised by the treating medical team as a supportive option. This decision belongs with the hospital’s physicians, who can weigh the specific clinical picture, chamber availability, and timing. Bringing up the option early, before a crisis, can help ensure a care plan is in place if it is ever needed.
Frequently Asked Questions
Can hyperbaric oxygen therapy replace a blood transfusion?
No. HBOT does not replace the red blood cells lost during major bleeding. It temporarily increases the oxygen carried in the blood plasma to help support the body while it produces new red blood cells or while other treatments take effect.
How long does someone need HBOT for exceptional blood loss anaemia?
This varies by patient and is decided by the treating medical team. Treatment is usually most intensive during the acute, most critical period after major blood loss, and is reduced as the patient’s own red blood cell count recovers.
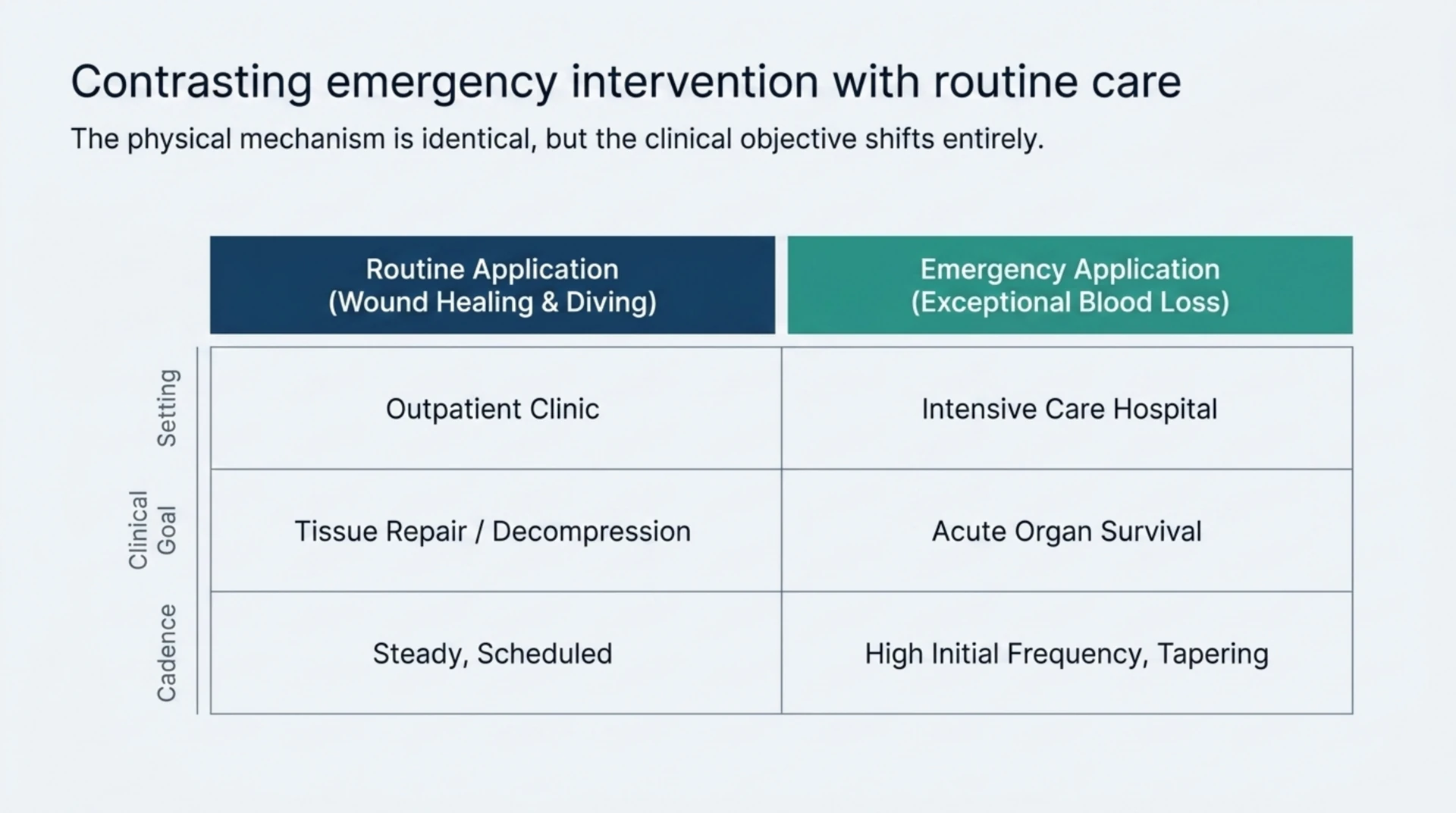
Is this the same as HBOT used for wound healing or diving injuries?
The basic principle of breathing pressurized oxygen is the same, but the clinical goal is different. Exceptional blood loss anaemia is an emergency use aimed at maintaining oxygen delivery to organs, usually in a hospital, while other HBOT uses focus on things like wound healing or decompression illness.
Can any hyperbaric facility provide this treatment?
This use requires a facility equipped and staffed for critical, hospital-level care, with a medical team able to monitor a critically ill patient closely. Not every hyperbaric facility is set up for this. Our facilities page explains what to look for in a properly equipped centre.
This content is for informational purposes only and is not medical advice.