
TL;DR: Carbon monoxide (CO) poisoning is a leading cause of poisoning death in Canada, and hyperbaric oxygen therapy (HBOT) is an established option for severe cases. Every CO-poisoned patient needs 100% normobaric oxygen immediately and emergency assessment first. Hyperbaric medicine societies recommend considering HBOT for acute symptomatic poisoning, particularly with loss of consciousness, neurological or cardiac involvement, a high carboxyhaemoglobin (COHb) level, or pregnancy. Observational data link earlier treatment to better recovery, while randomised-trial evidence remains mixed. This guide for Canadian referring physicians covers when to refer, how fast, how severity is judged, and where to send patients.
Carbon monoxide poisoning is a form of tissue hypoxia caused by inhaling carbon monoxide, a colourless, odourless gas that binds haemoglobin more than 200 times more avidly than oxygen and disrupts cellular respiration at the mitochondrial level. For a referring physician, the pressing questions are rarely about pathophysiology. They are about triage: which patient needs hyperbaric oxygen therapy, how quickly, and where to send them. This guide answers those questions for Canadian practice, with the evidence stated plainly and the uncertainty left intact.
Carbon monoxide poisoning sits on both major indication lists. It is one of the 14 conditions publicly funded in Canada for hyperbaric chamber licensing, and it is a UHMS-recognised indication for hyperbaric oxygen. These are two separate lists that overlap on CO. The practical takeaway is that HBOT for CO poisoning is a mainstream, on-label use, not an experimental one.
Why does carbon monoxide threaten the brain and heart?
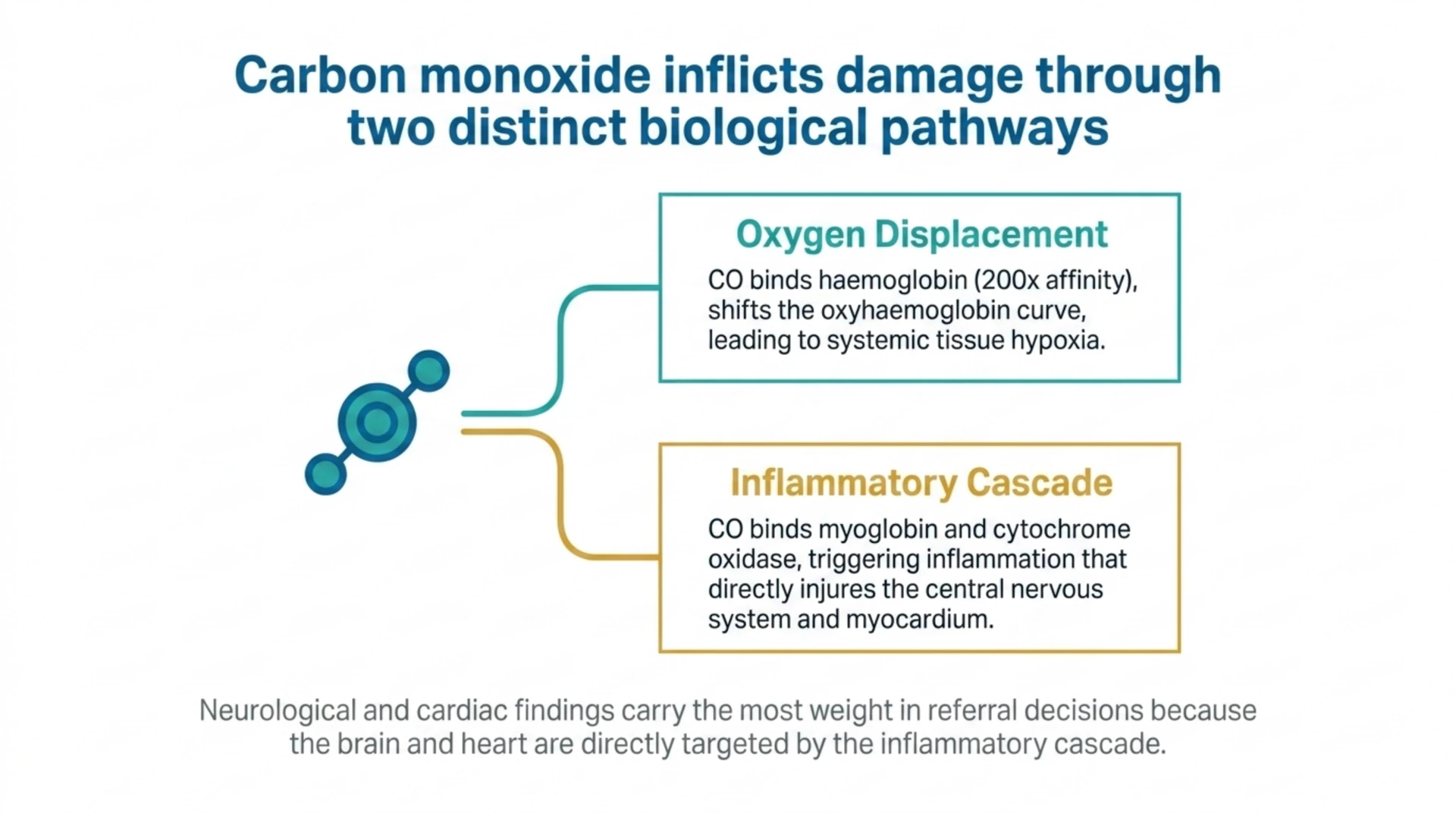
Carbon monoxide harms patients through more than simple oxygen displacement. It shifts the oxyhaemoglobin dissociation curve, binds myoglobin and cytochrome oxidase, and triggers an inflammatory cascade that injures the brain and heart hours to days after exposure. The two organs that drive prognosis are the central nervous system and the myocardium, which is why neurological and cardiac findings carry so much weight in referral decisions.
The most feared outcome is delayed neuropsychiatric sequelae (DNS), also called delayed encephalopathy. Patients can appear to recover, then return days to weeks later with cognitive impairment, movement disorders, personality change, or parkinsonism. A 2026 case report described delayed-onset parkinsonism after CO poisoning (Ingiardi and colleagues, PubMed | Our Assessment), a reminder that the consequences are not always obvious in the emergency department. Reducing the risk of DNS is the central rationale for hyperbaric referral. Canada Hyperbarics maintains a plain-language overview of this condition on our carbon monoxide poisoning condition page.
When should you refer a CO-poisoned patient for hyperbaric oxygen?
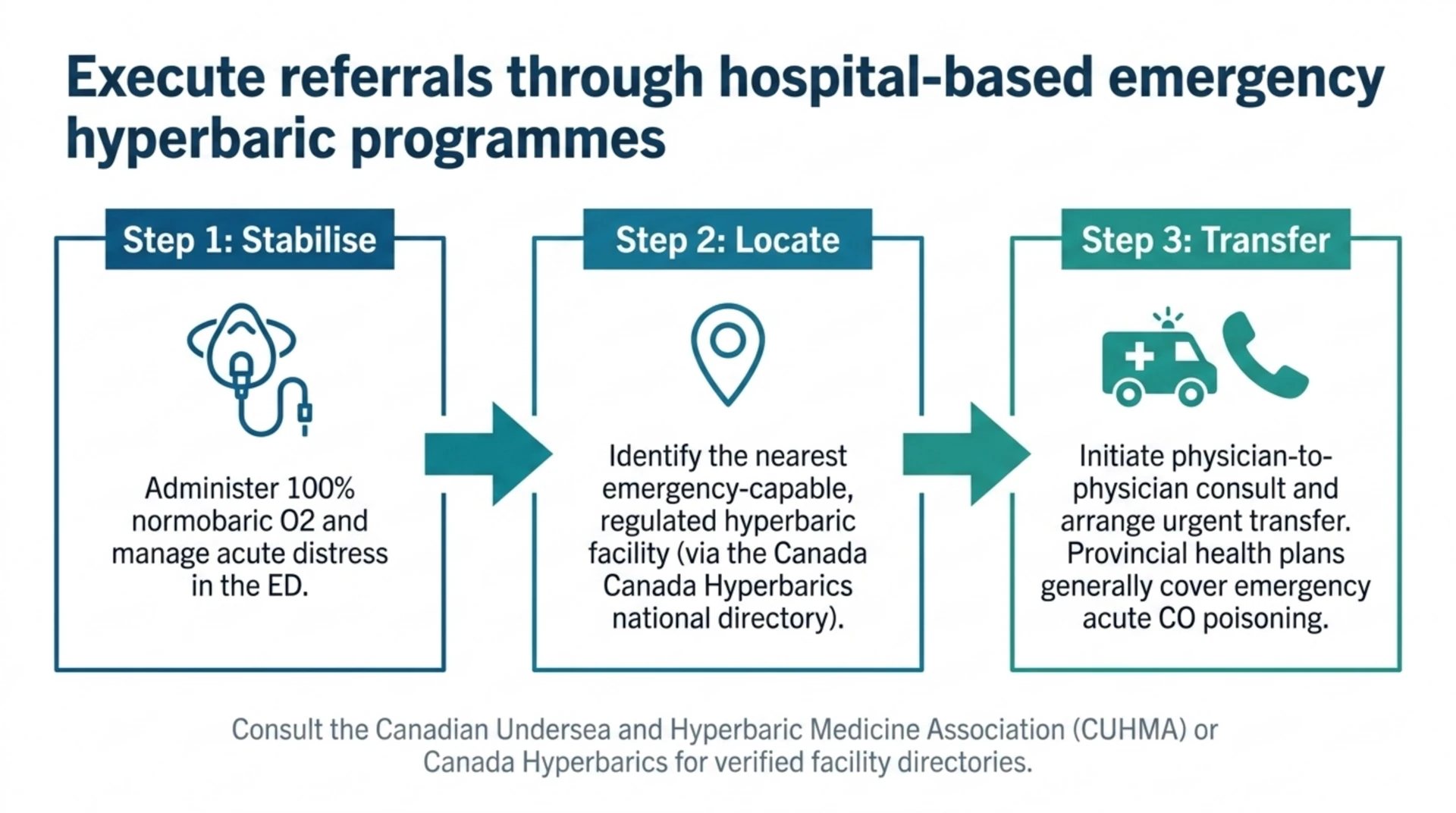
First principle: every patient with suspected CO poisoning should receive high-flow 100% normobaric oxygen at once and be moved to emergency care. Normobaric oxygen shortens the half-life of carboxyhaemoglobin and is the universal first step. Hyperbaric oxygen is the escalation for patients at higher risk of poor outcomes.
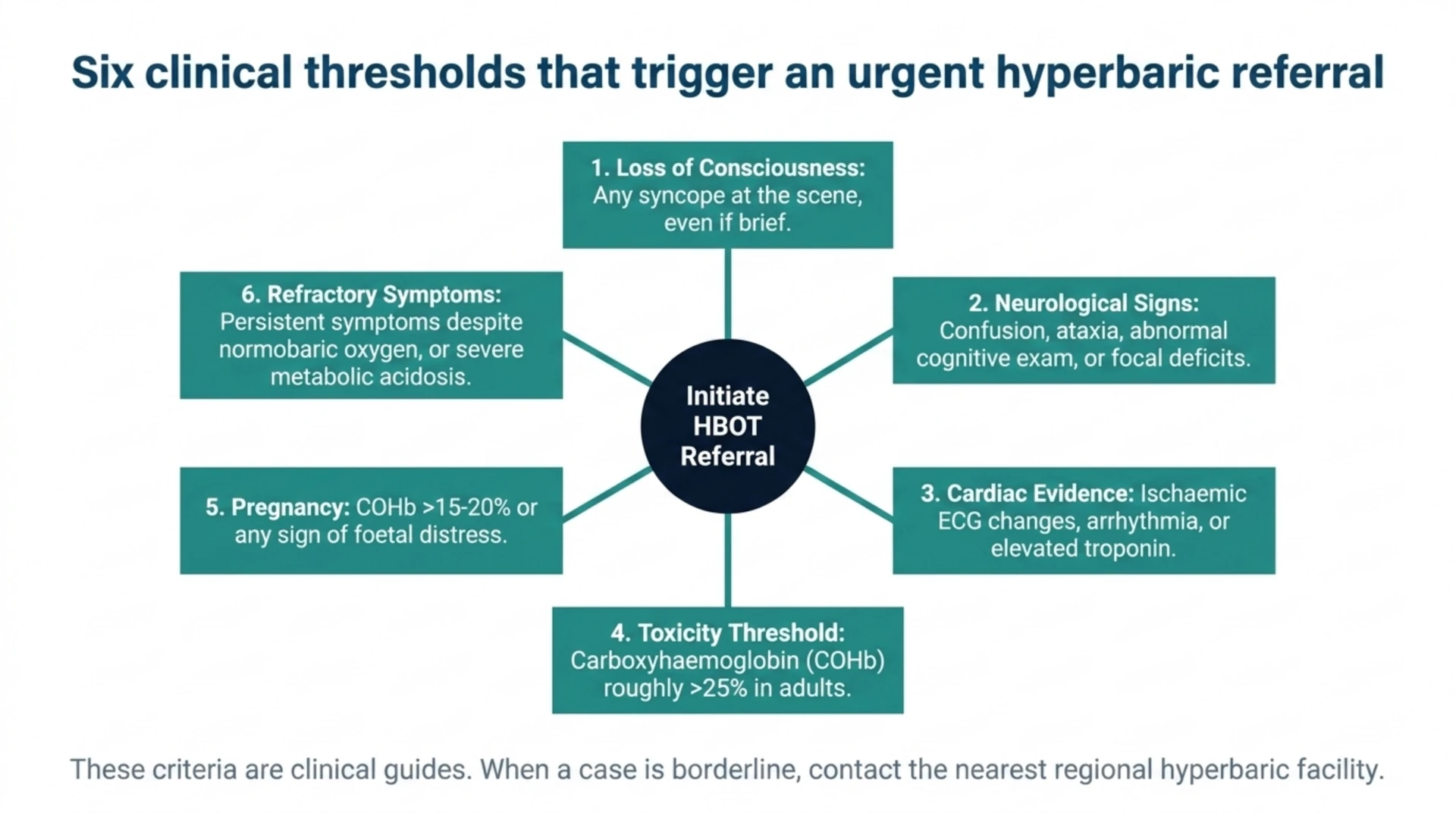
The Undersea and Hyperbaric Medical Society states that hyperbaric oxygen should be considered for all cases of acute symptomatic CO poisoning. In day-to-day Canadian practice, hyperbaric units and emergency physicians most often apply the following criteria when deciding whom to refer:
- Any loss of consciousness or syncope at the scene, even if brief.
- Neurological signs or an abnormal cognitive examination, including confusion, ataxia, or focal deficits.
- Evidence of cardiac involvement, such as ischaemic ECG changes, arrhythmia, or elevated troponin.
- A carboxyhaemoglobin level above roughly 25% in adults.
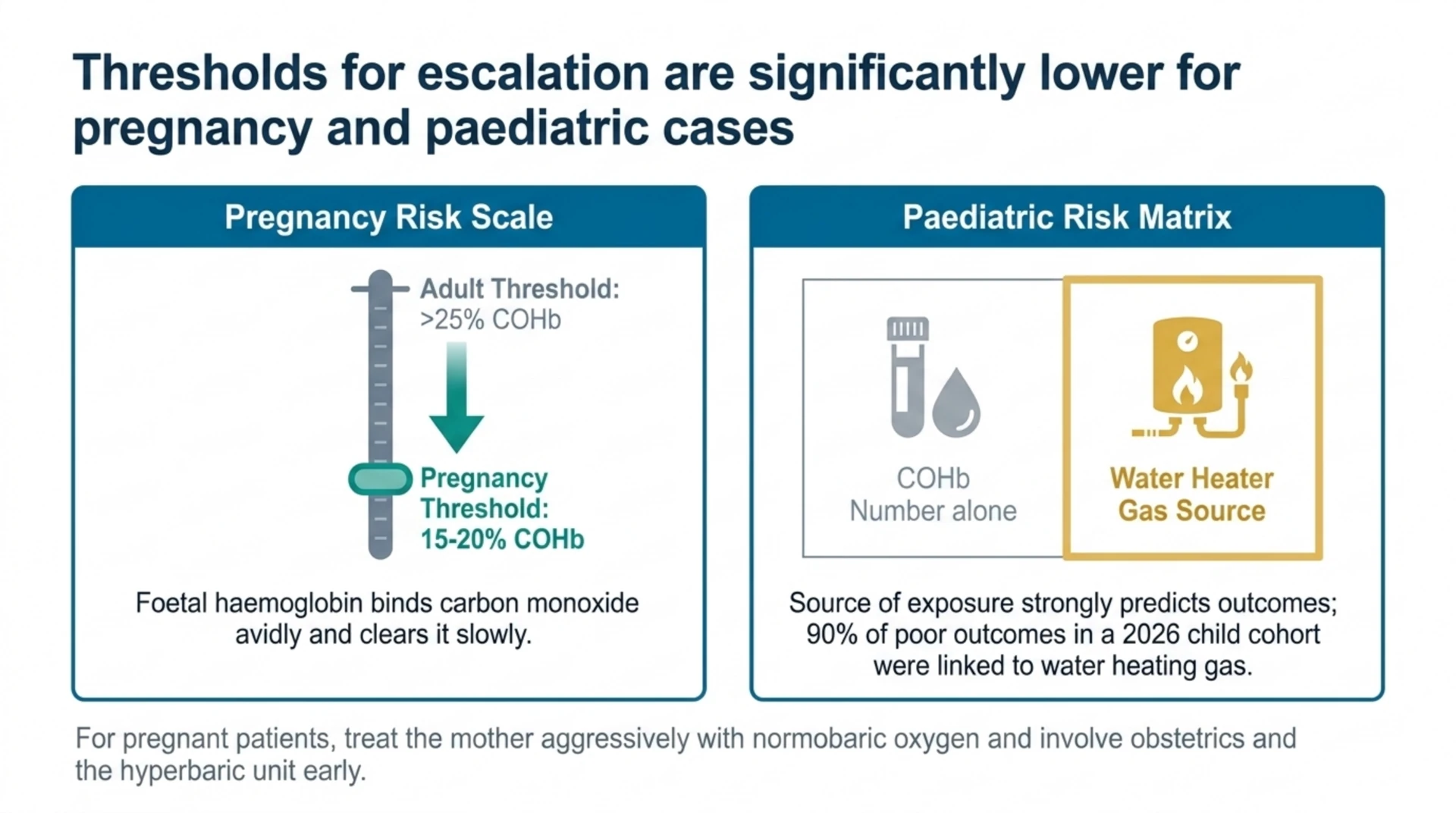
- Pregnancy with a COHb above about 15% to 20%, or any sign of foetal distress.
- Persistent symptoms despite an adequate trial of normobaric oxygen, or severe metabolic acidosis.
These criteria are guides, not rigid rules. The decision is clinical, and a phone call to your nearest hyperbaric facility is always reasonable when a case is borderline. A retrospective cohort of 272 adults found that lower Glasgow Coma Scale scores, ischaemic ECG findings, and lactate were independently associated with the decision to use HBOT (Yüceer, PubMed | Our Assessment), which mirrors how most clinicians weigh severity in real practice.
Why does timing matter so much for HBOT referral?
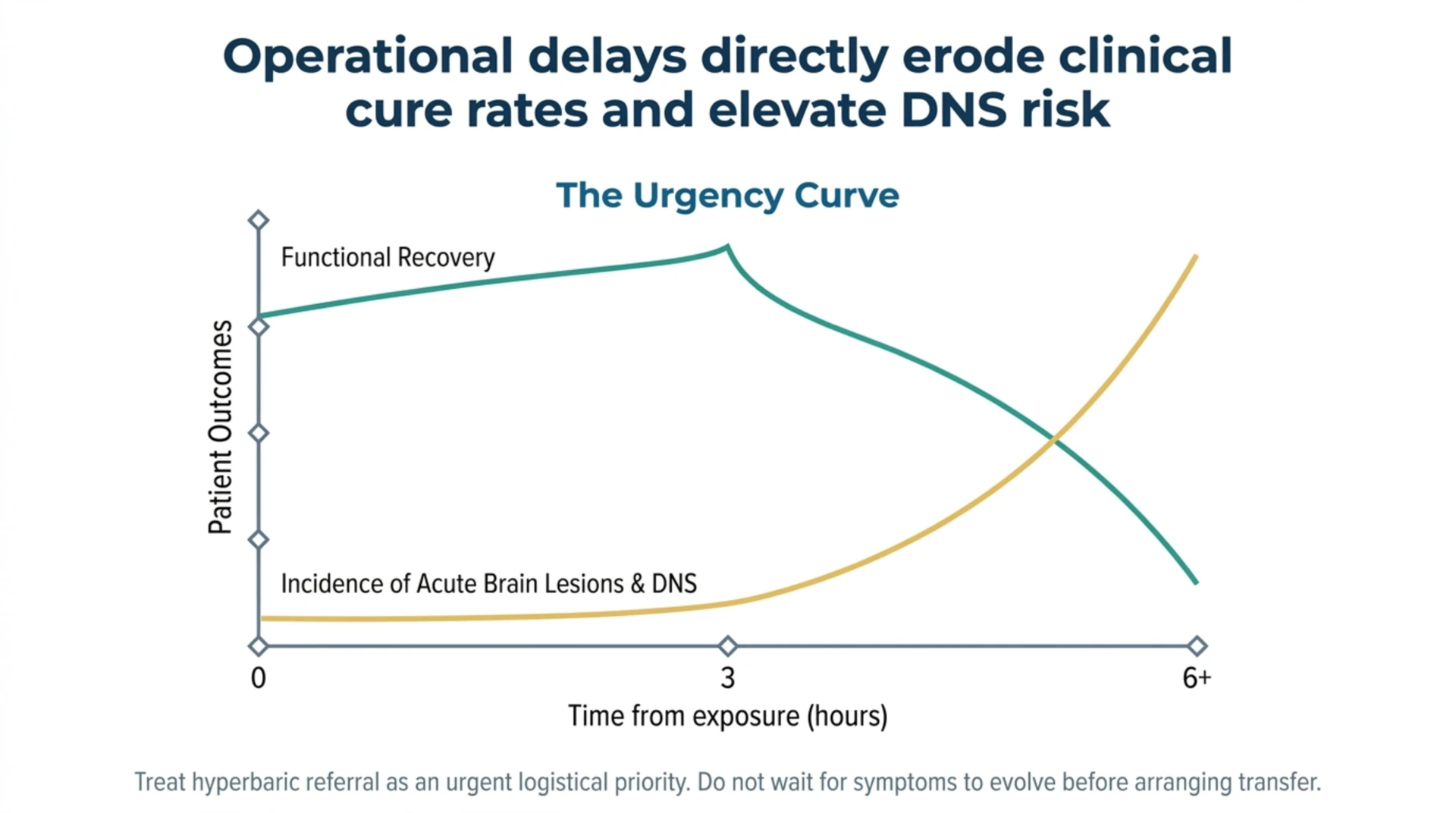
The strongest practical message in the recent CO literature is that delay appears to cost the patient. A 2026 retrospective cohort reported that acute brain lesions on MRI and a delay to hyperbaric oxygen of more than six hours were each associated with a lower clinical cure rate and a higher incidence of delayed encephalopathy (Jia and colleagues, PubMed | Our Assessment). Because this is observational data, it shows association rather than proof of causation, but the direction is consistent with the long-standing teaching that earlier treatment is better.
A small 2026 retrospective study of 12 patients with moderate-to-severe poisoning reported that starting HBOT within three hours was associated with faster functional recovery and that early lactate clearance tracked with better neurological outcomes (Xu and colleagues, PubMed | Our Assessment). The authors describe these findings as exploratory given the small sample and the absence of a non-HBOT control group. For a referring physician, the lesson is operational: when a patient meets referral criteria, treat the referral as urgent and arrange transfer without waiting for symptoms to evolve.
What does the evidence actually say about HBOT for CO poisoning?
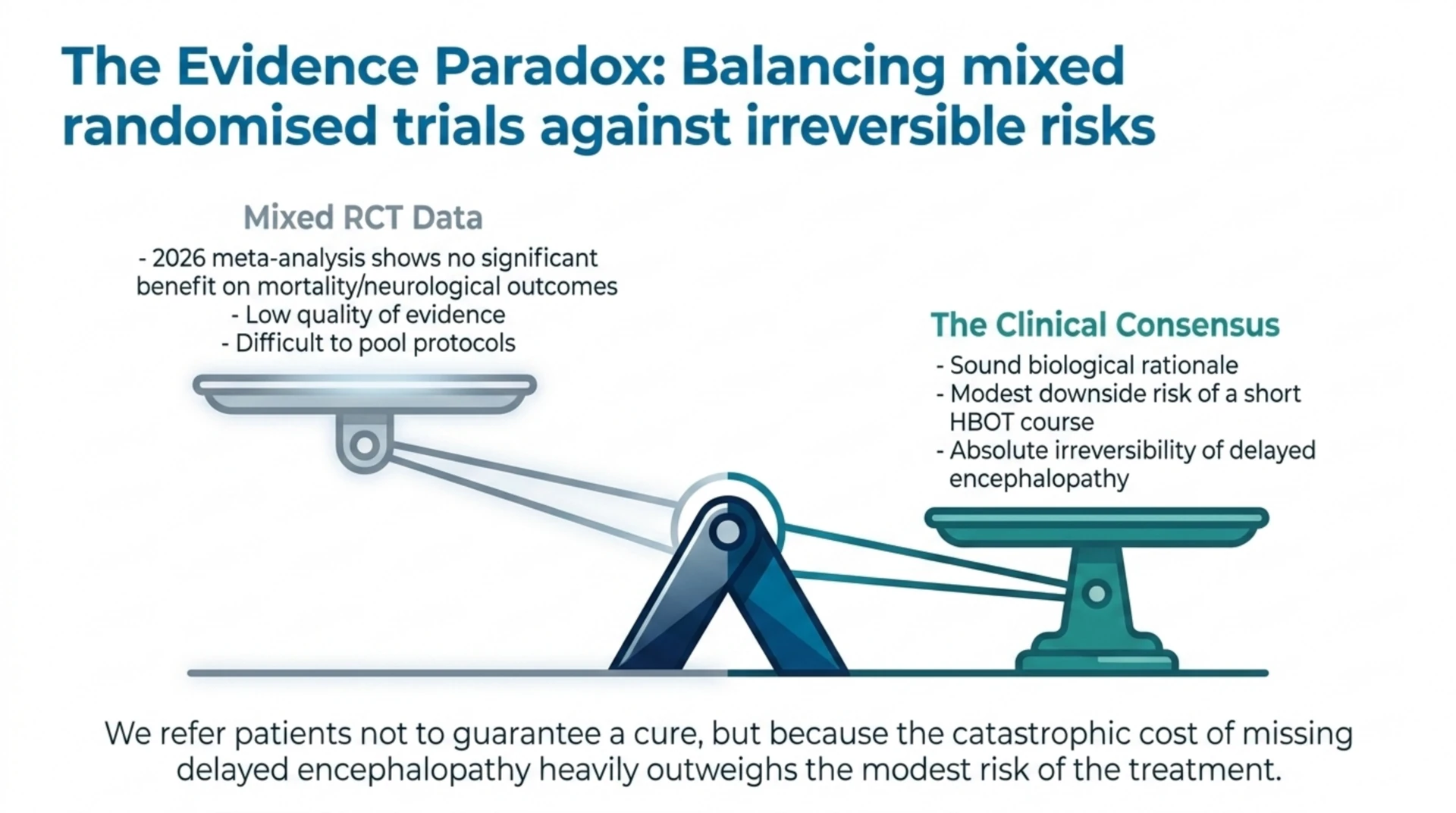
Honest counselling of patients and colleagues requires acknowledging that the randomised evidence is mixed. Some randomised trials have reported reduced cognitive sequelae with hyperbaric oxygen, while others have not, and differences in protocols, timing, and outcome measures make pooling difficult. A 2026 systematic review and meta-analysis of randomised controlled trials found no significant benefit of hyperbaric oxygen on mortality or neurological outcomes, and a subgroup analysis of treatments at or above 2.5 ATA showed no significant advantage either (Fujita and colleagues, PubMed | Our Assessment). The authors rated the quality of evidence as low to very low and noted that potential benefits may still exist but remain unproven.
How should a referring physician hold these two facts together: a mainstream indication on one hand, and a null meta-analysis on the other? The reasonable position is the one most hyperbaric units take. Hyperbaric oxygen is offered for severe symptomatic CO poisoning because the biological rationale is sound, the downside risk of a short course is modest, and the most serious outcome, delayed encephalopathy, is one we cannot reliably reverse once it appears. A 2025 review of CO poisoning diagnosis and management reached a similar practical conclusion, noting that HBOT remains the primary advanced treatment but is not always accessible (Afzal and colleagues, PubMed | Our Assessment). Refer when criteria are met, and be candid with the patient that the goal is to reduce risk, not to guarantee a result.
How is severity assessed before referral?
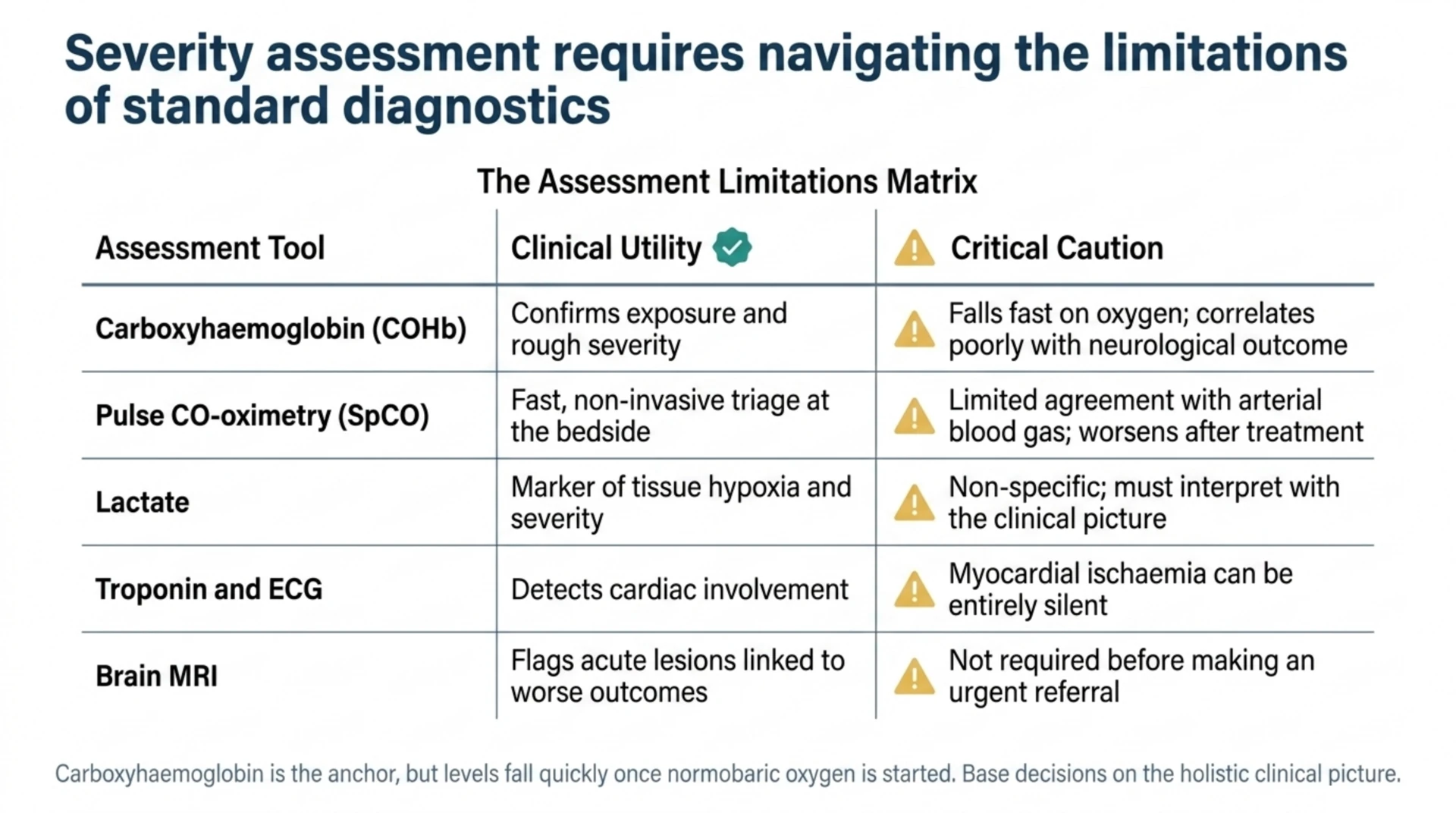
Severity assessment combines history, examination, and a few targeted investigations. Carboxyhaemoglobin remains the anchor, but it is an imperfect one: levels fall quickly once oxygen is started and correlate poorly with the eventual neurological outcome. A 2026 prospective study of 81 patients found that non-invasive pulse CO-oximetry (SpCO) showed only limited agreement with arterial COHb, with a positive bias and wide limits of agreement that worsened after treatment (Lee and colleagues, PubMed | Our Assessment). Use bedside SpCO for triage, but confirm with a blood gas when the number will change management.
| Assessment | What it adds | Caution |
|---|---|---|
| Carboxyhaemoglobin (COHb) | Confirms exposure and rough severity | Falls fast on oxygen; weak link to outcome |
| Pulse CO-oximetry (SpCO) | Fast, non-invasive triage at the bedside | Limited agreement with arterial COHb |
| Lactate | Marker of tissue hypoxia and severity | Non-specific; interpret with the picture |
| Troponin and ECG | Detects cardiac involvement | Ischaemia can be silent |
| Brain MRI | Flags acute lesions linked to worse outcome | Not needed before urgent referral |
Lactate is a useful adjunct. A 2026 retrospective study of 169 patients identified a lactate above 2.8 mmol/L as predictive of the need for hyperbaric oxygen, with an area under the curve of 0.71 (Satilmis and colleagues, PubMed | Our Assessment). No single number decides the case, but a raised lactate alongside neurological or cardiac signs strengthens the argument for referral.
Can we predict who will develop delayed encephalopathy?
Risk stratification for DNS is an active research area, and it bears directly on referral because the patients at highest risk are exactly the ones a hyperbaric unit most wants to see early. A 2026 study built a predictive model for delayed encephalopathy in 102 patients and reported strong discrimination, with an area under the curve of 0.93 (Gong and colleagues, PubMed | Our Assessment). Length of stay, comorbidities such as hypertension and diabetes, and carboxyhaemoglobin were among the contributing variables.
The hyperbaric protocol itself may also matter. A retrospective comparison of four treatment regimens across 312 patients found that patients treated at 2.8 ATA had a lower rate of delayed neuropsychiatric sequelae than those treated at 2.0 ATA, at 19% versus 36% (Gur and colleagues, PubMed | Our Assessment). This is a within-study observational comparison, so it informs protocol discussions at hyperbaric units rather than the referral decision itself. For the referring physician, the message is simply that protocol choice is part of why prompt specialist involvement is valuable.
Are there special considerations for children and pregnancy?
Pregnancy lowers the threshold to treat. Foetal haemoglobin binds carbon monoxide avidly and clears it slowly, so most protocols recommend considering hyperbaric oxygen at a lower maternal COHb and with any evidence of foetal compromise. Treat the mother, give normobaric oxygen generously, and involve obstetrics and the hyperbaric unit early.
Children deserve the same vigilance. A 2026 retrospective cohort of 95 children with a COHb above 5% found that poor outcomes were most frequent among those exposed through gas used for water heating, at 90% in that group (Kaplan and colleagues, PubMed | Our Assessment). Source of exposure and clinical severity, not the COHb number alone, should guide how aggressively a paediatric case is escalated.
Where can Canadian physicians refer patients for HBOT?
For an acutely poisoned patient, the safest first step is emergency services and the nearest emergency department, which can begin normobaric oxygen and contact the regional hyperbaric programme. Acute carbon monoxide poisoning is treated in hospitals and regulated facilities with emergency-capable hyperbaric chambers, and access varies by region. Canada Hyperbarics maintains a national directory of hyperbaric facilities across Canada so referring physicians can identify the closest appropriate unit and confirm its emergency capability in advance.
The Canadian Undersea and Hyperbaric Medicine Association is the national professional body for the field and is a useful reference point for standards and facility contacts. For prevention messaging to share with patients and families, Health Canada’s carbon monoxide resources remain the authoritative Canadian source. Physicians who want to review the underlying studies can also browse our research library, which links each summary back to its primary source on PubMed.
Frequently asked questions from referring physicians
Is hyperbaric oxygen mandatory for every CO-poisoned patient?
No. Normobaric oxygen is universal and first-line. Hyperbaric oxygen is reserved for patients with higher-risk features such as loss of consciousness, neurological or cardiac involvement, a high carboxyhaemoglobin level, or pregnancy. Mild, asymptomatic exposures are usually managed with normobaric oxygen and observation.
How quickly should HBOT be started?
As soon as feasible. Observational studies associate shorter delays with better outcomes, and a delay beyond six hours has been linked to a higher rate of delayed encephalopathy. Treat referral as urgent rather than elective once criteria are met, and arrange transfer early.
Does a normal carboxyhaemoglobin level rule out the need for referral?
No. Carboxyhaemoglobin falls rapidly once oxygen is given and correlates poorly with neurological outcome. Base the referral decision on the clinical picture, including symptoms at the scene, examination findings, and cardiac markers, rather than the COHb number alone.
Is carbon monoxide poisoning covered by provincial health plans?
Acute CO poisoning is treated as a medical emergency in hospital, and emergency hyperbaric care is delivered through hospital-based programmes. Carbon monoxide poisoning is one of the conditions publicly funded in Canada and is included on provincial hyperbaric coverage lists such as Ontario’s OHIP-funded indications. Confirm specifics with the treating hospital and the patient’s provincial plan.
What is delayed neuropsychiatric sequelae, and why does it matter?
Delayed neuropsychiatric sequelae, also called delayed encephalopathy, is the late onset of cognitive, psychiatric, or movement problems days to weeks after apparent recovery. Because it can be difficult to reverse, reducing its risk is the main reason hyperbaric oxygen is considered for severe poisoning, and it is the outcome most prediction models try to anticipate.
Should I refer if the patient already feels better after normobaric oxygen?
Possibly. Symptomatic improvement is reassuring but does not exclude the risk of delayed sequelae, especially after loss of consciousness, cardiac involvement, or a high exposure. When higher-risk features were present, a discussion with the hyperbaric unit is worthwhile even if the patient looks well.
The bottom line for referring physicians
Carbon monoxide poisoning is common, dangerous, and time-sensitive. Give normobaric oxygen to everyone, assess severity with the clinical picture rather than the COHb number alone, and refer promptly when loss of consciousness, neurological or cardiac involvement, a high COHb, or pregnancy is present. The randomised evidence is genuinely mixed, but the established indication, the sound rationale, and the irreversibility of delayed encephalopathy together justify urgent referral for severe cases. When in doubt, phone your regional hyperbaric programme. Canada Hyperbarics keeps an up-to-date directory of hospitals and regulated facilities to help you find the right one quickly.
This content is for informational purposes only and does not constitute medical advice. It is intended to support, not replace, the clinical judgement of qualified health professionals. Management of carbon monoxide poisoning should follow local emergency protocols and specialist guidance.