
TL;DR: Osteoradionecrosis (ORN) of the jaw is a late complication of head and neck radiotherapy. Hyperbaric oxygen therapy is one component of multidisciplinary management alongside antibiotics, the PENTOCLO protocol, and surgical reconstruction. Recent evidence is heterogeneous: HBOT is associated with high response rates in some radiation injuries (notably haemorrhagic cystitis), while data for established mandibular ORN are mixed. This guide summarises the 2025-2026 evidence base and outlines the referral pathway for Canadian physicians.
Osteoradionecrosis of the jaw is one of the most challenging late toxicities of head and neck cancer treatment. For Canadian referring physicians, the decision about when to involve hyperbaric oxygen therapy (HBOT) has evolved with the 2025-2026 evidence: the older Marx prevention protocol is no longer the unquestioned default, and high-quality reviews now place HBOT inside a wider multidisciplinary framework. This guide summarises what the recent literature says, outlines the Canada Hyperbarics referral pathway, and flags the screening considerations Canadian referrers should keep in mind.
What is osteoradionecrosis of the jaw?
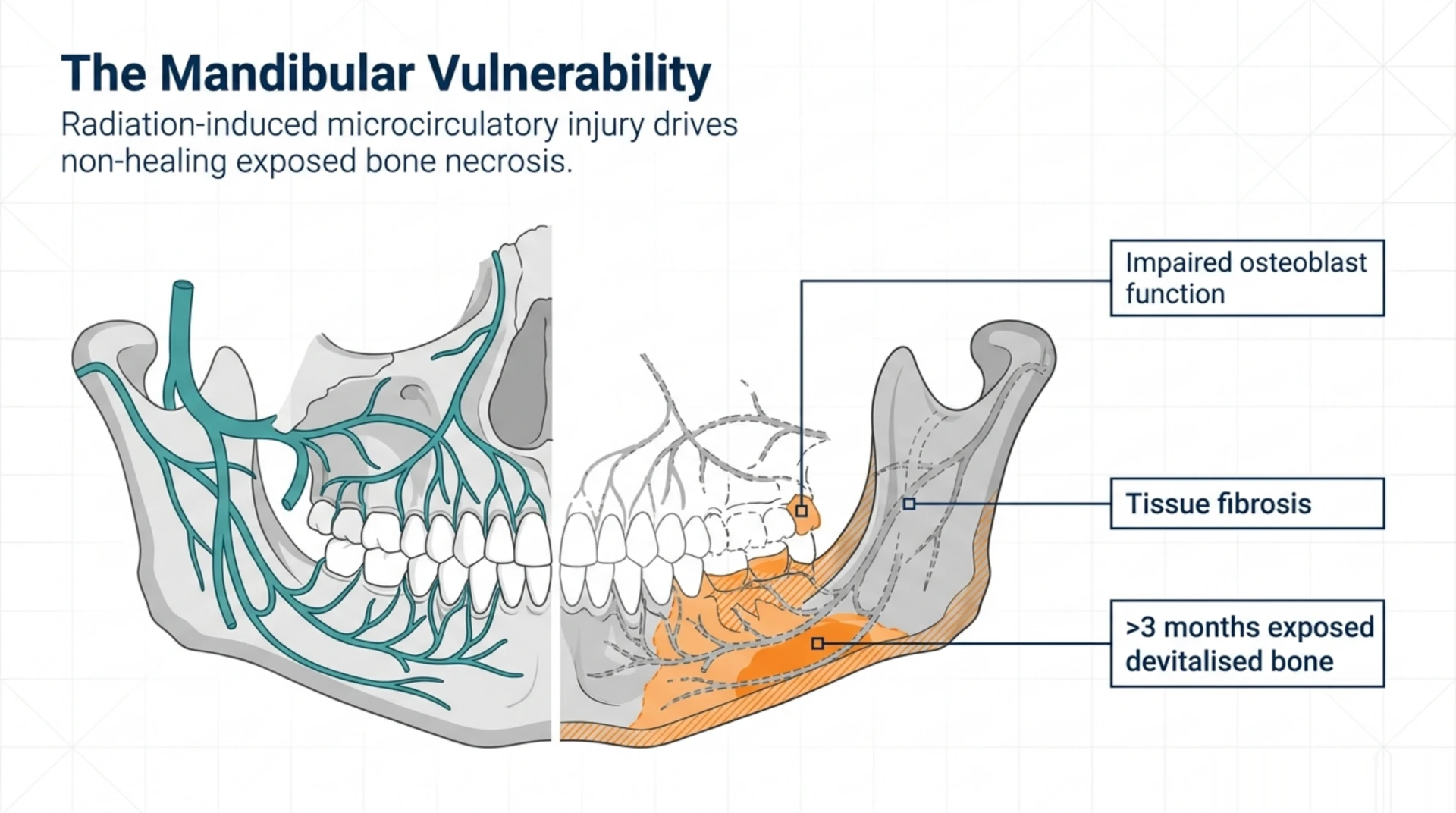
Osteoradionecrosis of the jaw is a non-healing, exposed-bone necrosis of the mandible or maxilla that develops months to years after therapeutic ionising radiation. It is driven by radiation-induced microcirculatory injury, fibrosis, and impaired osteoblast function in previously irradiated tissue. The classic presentation is exposed devitalised bone that persists for more than three months in a previously irradiated field without evidence of recurrent malignancy.
Incidence varies by primary site, radiation dose, fractionation, and dental status. A 2026 narrative review in Stem Cells by Liu and colleagues (PubMed | Our Assessment) reports an ORN incidence of 1.2% to 40% in patients receiving more than 60 Gy, particularly when concurrent dental trauma is present. The mandible is more commonly affected than the maxilla because of its denser cortical bone and comparatively limited collateral circulation.
How does hyperbaric oxygen therapy fit into the management framework?
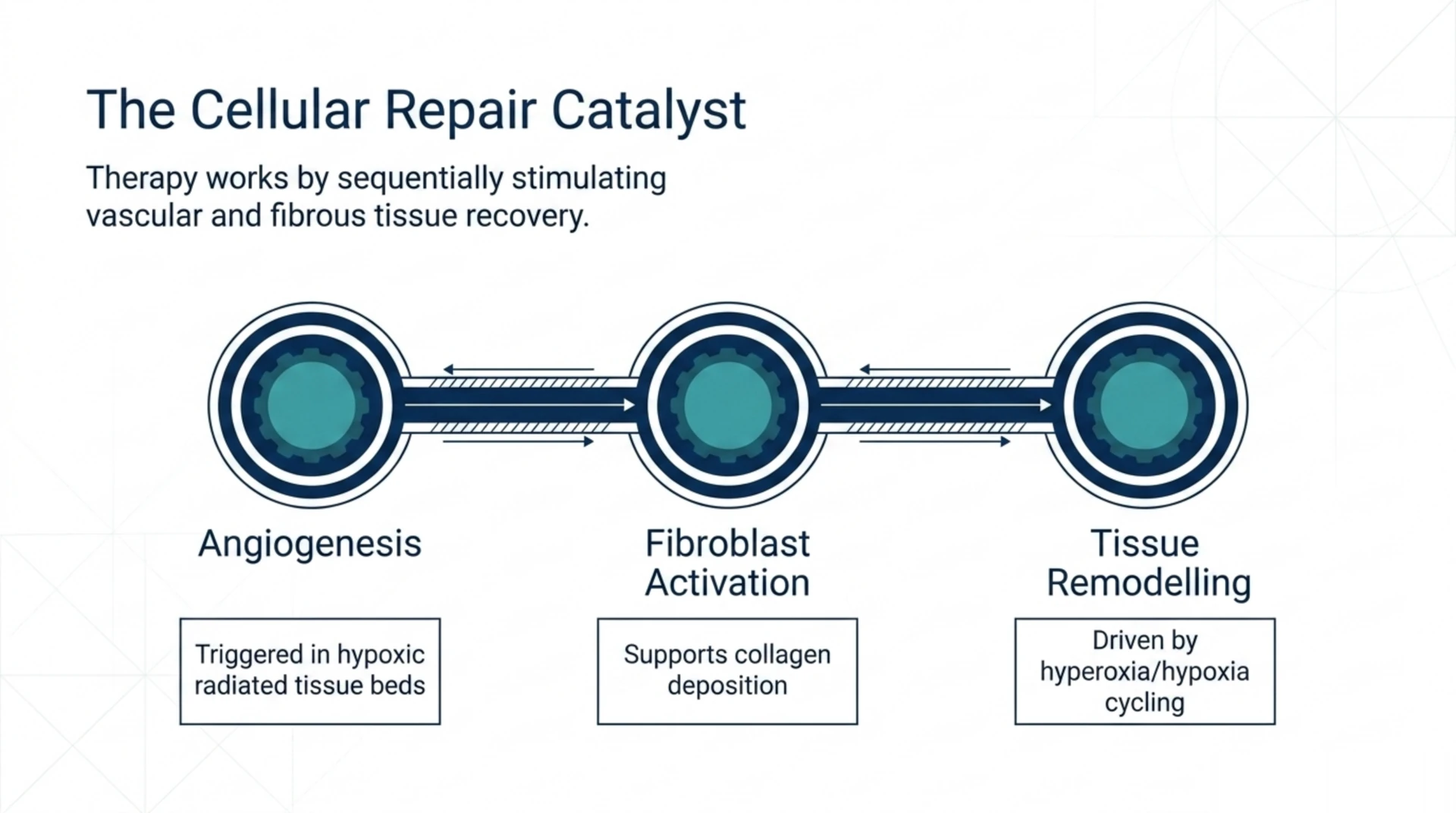
The therapeutic rationale for HBOT in radiation-injured tissue rests on three mechanisms: promotion of angiogenesis in hypoxic radiated tissue beds, fibroblast activation supporting collagen deposition, and tissue remodelling driven by repeated hyperoxia followed by relative hypoxia between sessions. A 2026 clinically focused review in CA: A Cancer Journal for Clinicians by Dejonckheere and colleagues (PubMed | Our Assessment) characterises HBOT as a potential adjunctive treatment for chronic radiation sequelae including skin fibrosis, bone necrosis, radiation cystitis, and proctitis. The authors note that high-quality randomised data remain limited and outline open questions in patient selection, optimal protocols, and long-term outcomes.
In clinical practice, HBOT is used in three contexts for jaw ORN:
- Prevention before dental extraction in patients with prior head and neck radiotherapy who require removal of teeth in the radiated field
- Treatment of established ORN, either alone in early-stage disease or combined with surgical debridement and reconstruction in advanced disease
- Adjunct to reconstructive surgery when free flap or bone graft reconstruction is required in the radiated bed
The Undersea and Hyperbaric Medical Society lists delayed radiation injury (soft tissue and bony necrosis) among its recognised indications for HBOT, which is the framework most Canadian hyperbaric facilities use when assessing referrals for ORN.
What does the 2025-2026 evidence actually show?
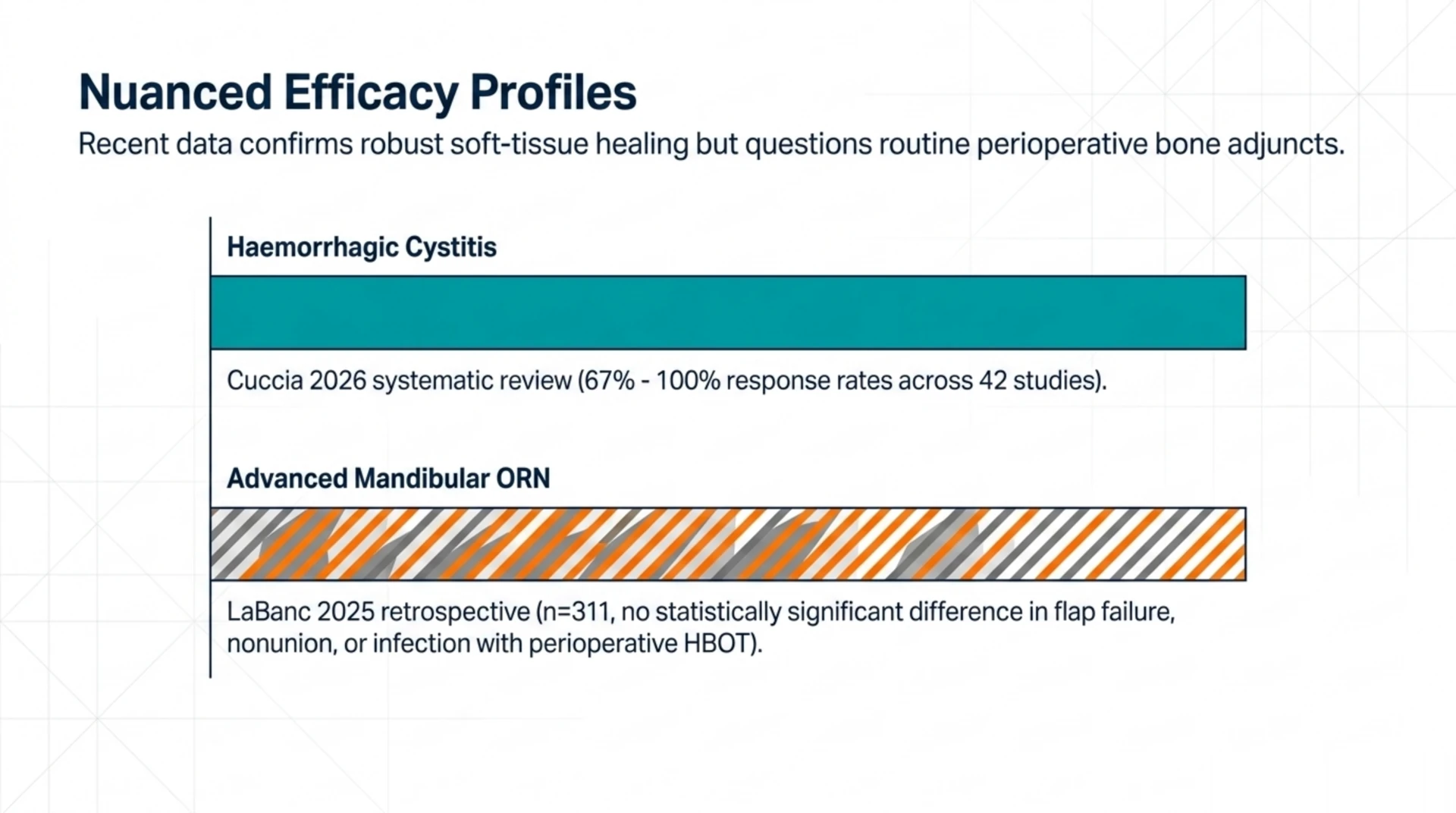
The most important update for referring physicians is that the evidence base is now more nuanced than the older Marx protocol literature suggested. A 2026 systematic review in Supportive Care in Cancer by Cuccia and colleagues (PubMed | Our Assessment) pooled 42 studies covering 2,785 patients, of which 28 were retrospective and only 5 were randomised controlled trials. The review reported high response rates (67% to 100%) for haemorrhagic cystitis, but found that randomised trials in breast and head and neck cancer failed to demonstrate consistent benefit. Median HBOT exposure across the included studies was 34.5 sessions at 2.45 atmospheres absolute.
For mandibular ORN specifically, a 2025 retrospective cohort study in Facial Plastic Surgery & Aesthetic Medicine by LaBanc and colleagues (PubMed | Our Assessment) compared 311 patients with advanced mandibular ORN treated with segmental mandibulectomy and free flap reconstruction. The HBO group (n=131) received hyperbaric oxygen pre- and post-operatively; the comparator group (n=180) did not. The authors found no statistically significant difference between groups in flap failure, nonunion, plate exposure, or postoperative infection rates. This finding tempers earlier enthusiasm about perioperative HBOT for free-flap reconstruction in established ORN and reinforces that HBOT is not a guaranteed surgical adjunct in this setting.
At the same time, a 2026 chapter by Feldmeier and colleagues in Undersea and Hyperbaric Medicine (PubMed | Our Assessment) notes that delayed radiation injuries remain the most frequent indication for hyperbaric treatment in the United States, accounting for roughly 40% of all CMS HBOT billings. The authors emphasise that HBOT should not be the sole modality for bone-involving radiation injury and that surgical technique, including tissue flaps and microvascular reconstruction, must be optimised in parallel.
How does HBOT compare to conservative and surgical management?
A 2025 prospective clinical study in the Journal of Pharmacy and Bioallied Sciences by Rao and colleagues (PubMed | Our Assessment) compared 60 ORN patients split into conservative management (antibiotics, HBOT, pentoxifylline, and tocopherol) and surgical management (sequestrectomy, resection, or free flap reconstruction). Pain relief was reported in 70% of the conservative group versus 90% of the surgical group, and the conservative approach had a higher recurrence rate. The authors concluded that conservative management is reasonable in early-stage disease but that surgical resection remains the gold standard for advanced ORN.
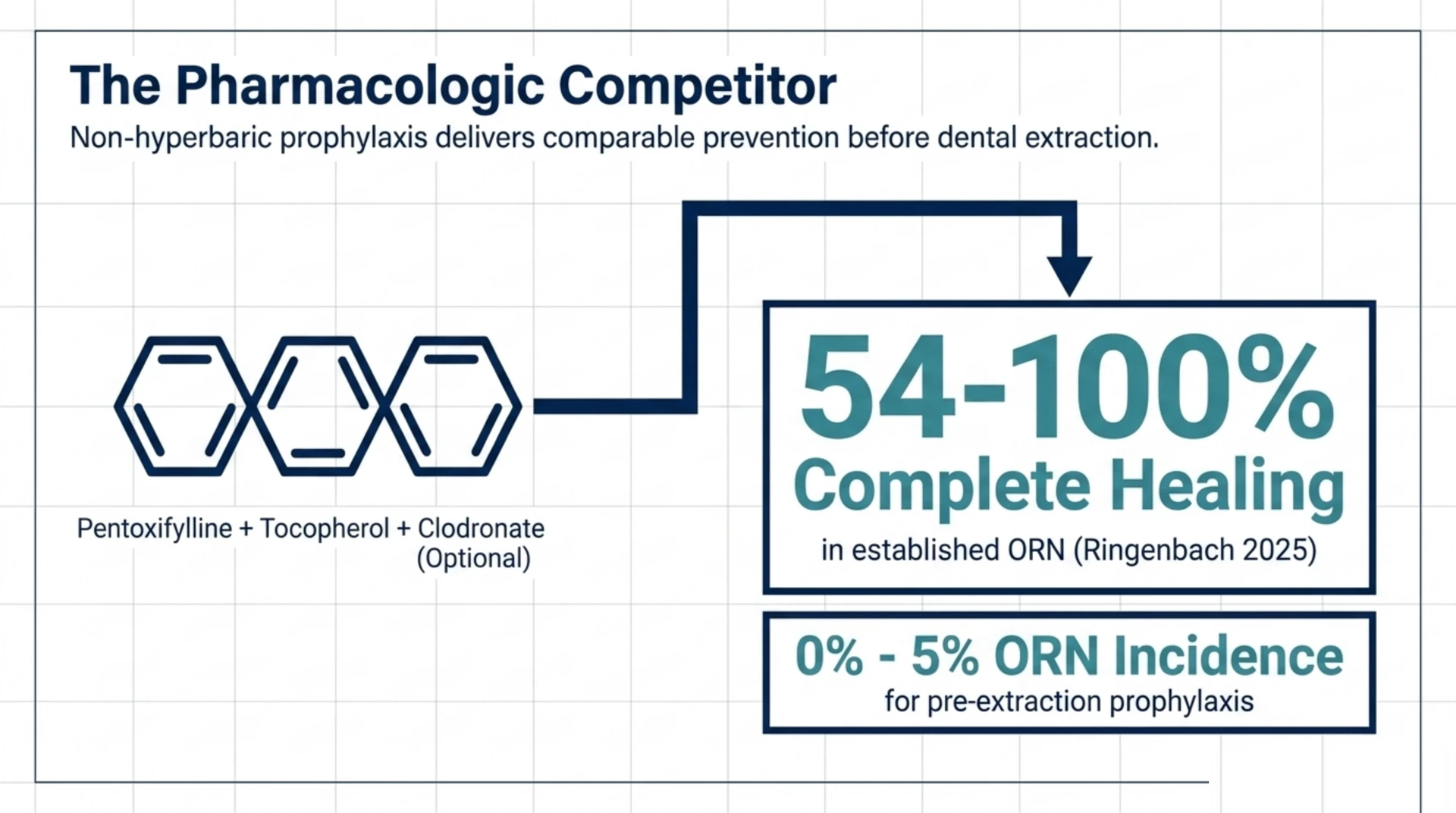
The PENTOCLO protocol, which combines pentoxifylline and tocopherol with optional clodronate, has become an important non-hyperbaric pharmacologic option. A 2025 literature review in the Ear, Nose & Throat Journal by Ringenbach and colleagues (PubMed | Our Assessment) synthesised 22 studies. PENTO or PENTOCLO was associated with complete healing in 54% to 100% of treated ORN patients across the included literature, with low adverse-effect rates. Prophylactic PENTO before dental extraction in irradiated patients was associated with ORN incidence between 0% and 5%. For referring physicians, this means HBOT is no longer the only credible prevention or treatment strategy, and a frank discussion with patients about both pathways is appropriate.
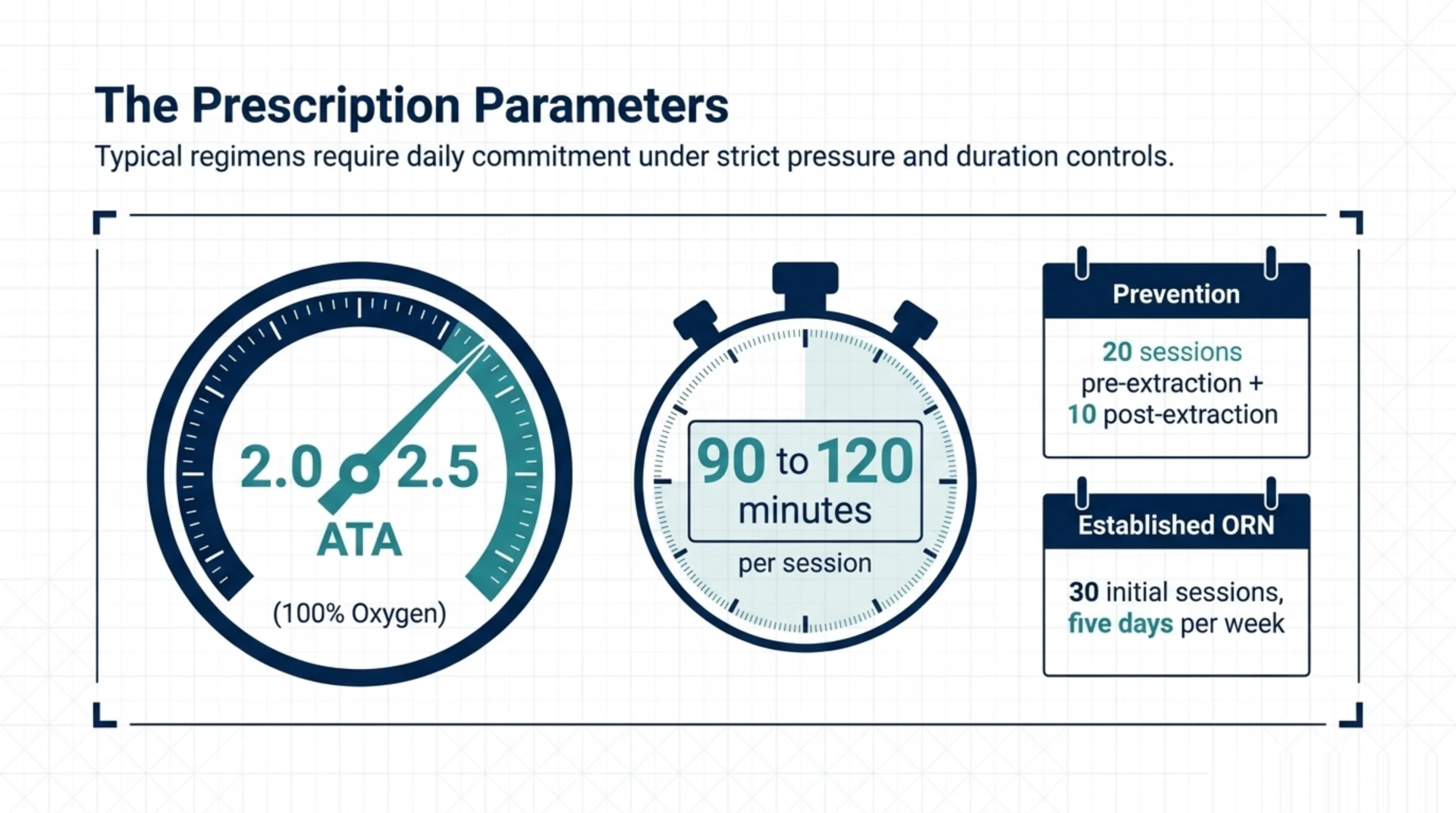
What does a typical HBOT protocol look like for ORN?
Most Canadian facilities follow protocols broadly consistent with UHMS guidance for delayed radiation injury. The typical features are summarised below.
| Parameter | Typical range |
|---|---|
| Treatment pressure | 2.0 to 2.5 atmospheres absolute |
| Session duration | 90 to 120 minutes at pressure on 100% oxygen |
| Pre-extraction prevention course | 20 sessions before the dental procedure plus 10 sessions after |
| Established ORN treatment course | 30 sessions, with reassessment and possible extension based on response |
| Frequency | Once daily, five days per week |
The exact protocol is set by the supervising hyperbaric physician at the treating facility based on the patient’s ORN stage, surgical plan, and oxygen-toxicity screening. Pressures and session counts are not interchangeable across indications, which is why the referring physician’s role is to confirm appropriateness for HBOT in principle and leave protocol specifics to the hyperbaric team.
Which patients should you consider referring?
Based on the 2025-2026 literature and UHMS guidance, the strongest candidates for HBOT referral are:
- Patients with prior head and neck radiotherapy at doses above 50 to 60 Gy who require dental extraction in the radiated field, particularly when conservative pharmacologic prophylaxis is contraindicated or has failed
- Patients with early-stage ORN (exposed bone without pathological fracture or extensive soft-tissue involvement) who have not yet undergone surgical resection
- Patients undergoing planned free-flap reconstruction of advanced ORN where the multidisciplinary team has decided perioperative HBOT may be of benefit, with the caveat that the recent retrospective comparator data are mixed (LaBanc 2025)
- Patients with concurrent radiation injuries such as soft-tissue necrosis, mucositis, or haemorrhagic cystitis where HBOT may address more than one indication in a single course
A 2025 review by Mascard and colleagues in Orthopaedics & Traumatology: Surgery & Research (PubMed | Our Assessment) describes antioxidants and HBOT as effective measures for ORN prevention in patients undergoing high-dose radiotherapy to bone, particularly when combined with general risk reduction such as correcting pre-existing osteopenia.
What are the contraindications and screening considerations?
Absolute and relative contraindications to HBOT are well-established. The referring physician’s pre-referral screening should consider:
- Untreated pneumothorax: absolute contraindication
- Active malignancy in the treatment field: requires multidisciplinary discussion. Current evidence does not support HBOT as a tumour stimulant, but co-management with the treating oncologist is essential
- Severe chronic obstructive pulmonary disease with bullous emphysema: relative contraindication; requires baseline imaging
- Uncontrolled seizure disorder: increased oxygen toxicity seizure risk
- Recent ear or sinus surgery, middle ear pathology: barotrauma risk; otolaryngology clearance may be required
- Bleomycin exposure: historic concern for pulmonary toxicity; current consensus favours individual risk-benefit assessment
- Claustrophobia or active anxiety disorders: manageable but requires advance preparation
The treating hyperbaric facility will conduct its own pre-treatment workup, including chest imaging and otolaryngology assessment where appropriate. The Canadian Undersea and Hyperbaric Medical Association maintains national resources for referring physicians seeking further detail on screening protocols.
How does the referral pathway work in Canada?
Canada has a mixed landscape of hospital-based and regulated private hyperbaric facilities. Delayed radiation injury is one of the indications covered by some provincial health plans when treatment is delivered at a hospital programme; private facilities operate on a fee-for-service basis, and coverage depends on the patient’s extended health benefits. A current directory of Canadian hyperbaric facilities is available on our facilities page, which lists hospitals and regulated facilities offering HBOT for delayed radiation injury.
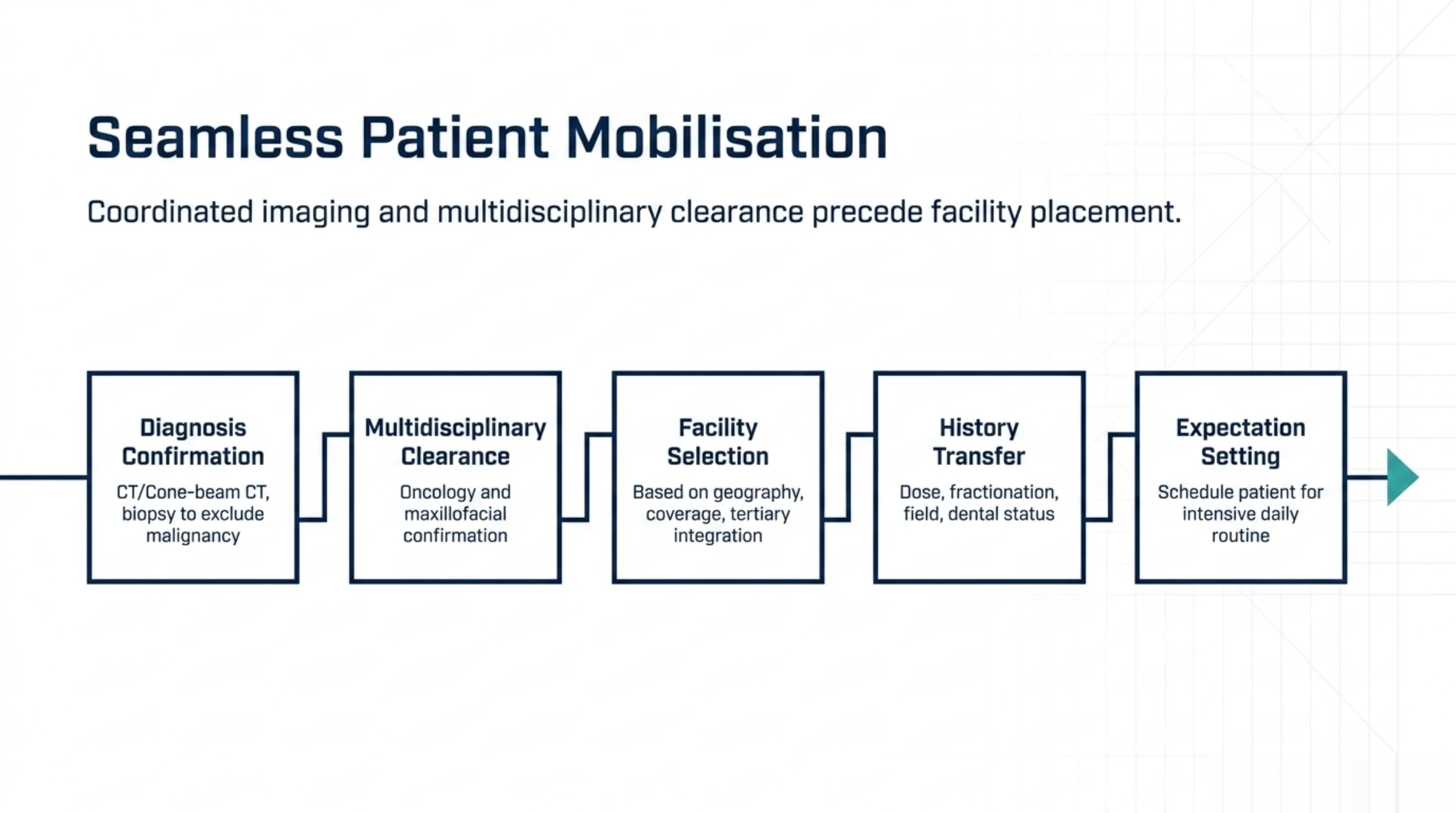
The typical referral workflow is:
- Confirm the clinical diagnosis of ORN with appropriate imaging (orthopantomogram and CT or cone-beam CT) and biopsy where malignancy must be excluded
- Coordinate with the treating oncology and maxillofacial teams to confirm there is no active recurrent disease in the radiated field
- Identify the appropriate hyperbaric facility based on geography, indication coverage, and waitlist. For complex cases involving planned surgical reconstruction, prefer a facility integrated with a tertiary head and neck programme
- Provide the hyperbaric team with the radiotherapy history, including total dose, fractionation, and field, together with current dental status and any planned procedures
- Set patient expectations about treatment duration (six to eight weeks for a 30-session course at daily sessions, five days per week)
For broader context on Canadian access pathways, see our coverage page and the delayed radiation injury condition guide.
What should you tell patients before referring?
Patient-facing counselling should be honest about both potential benefit and uncertainty. Key points to convey:
- HBOT is one of several modalities used for ORN; the treating team will combine antibiotics, pharmacologic therapy (PENTO or PENTOCLO), and surgical management as appropriate
- The evidence base for HBOT in established mandibular ORN is mixed; recent retrospective data found no significant difference in surgical outcomes with perioperative HBOT in advanced disease
- For prevention of ORN before dental extraction in irradiated patients, HBOT and PENTO are both reasonable strategies with comparable supporting evidence
- A typical course requires six to eight weeks of near-daily attendance, which has practical implications for work, travel, and caregiver support
- Common side effects include reversible myopia, middle-ear barotrauma, and rare seizures from oxygen toxicity
A 2025 retrospective survey of 80 head and neck cancer survivors in the Journal of Pharmacy and Bioallied Sciences by Saha and colleagues (PubMed | Our Assessment) reported 84.8% dental implant survival at five years, with better outcomes in patients who received less than 50 Gy and waited at least 12 months between radiotherapy and implant placement. HBOT use was tracked as a variable in this cohort, and the authors recommend careful patient selection and an integrated rehabilitation plan rather than relying on any single adjunct.
Frequently asked questions from referring physicians
Is HBOT still indicated for ORN prevention before dental extraction?
Yes, but it is no longer the only option. UHMS continues to list delayed radiation injury among recognised indications, and HBOT remains a reasonable choice for high-risk patients (radiation dose above 60 Gy, mandibular field, multiple extractions). The PENTOCLO protocol now offers a pharmacologic alternative with supporting evidence in 22 studies summarised by Ringenbach 2025. Many Canadian centres use a shared decision-making approach.
What is the strongest current evidence for HBOT in radiation injury?
The strongest signal is for haemorrhagic radiation cystitis, where Cuccia 2026 reported response rates of 67% to 100% across 42 included studies. Evidence for established mandibular ORN is more mixed: HBOT is associated with healing in some prospective cohorts but recent retrospective comparator data (LaBanc 2025, n=311) found no significant difference in surgical outcomes when added perioperatively in advanced disease.
Does HBOT increase the risk of cancer recurrence?
The Feldmeier 2026 review explicitly addresses this concern and reports literature supporting the safety of HBOT in cancer survivors. Current consensus does not regard HBOT as a tumour stimulant. That said, co-management with the treating oncologist is appropriate, and HBOT is not initiated until active recurrent disease has been excluded.
How many sessions will my patient actually need?
For prevention before dental extraction, a typical course is 20 sessions before and 10 after the procedure. For established ORN, 30 sessions is a common initial course with reassessment at completion. Median exposure in the Cuccia 2026 systematic review was 34.5 sessions at 2.45 atmospheres absolute, which is broadly consistent with Canadian practice.
What if the patient has already failed HBOT?
Failed HBOT is not uncommon in advanced ORN. A 2025 retrospective series by Vos and colleagues in Otolaryngology Head and Neck Surgery (PubMed | Our Assessment) reviewed 23 patients undergoing iliac crest bone graft and anterolateral thigh fascia lata rescue flap; 39.1% had failed prior HBOT and 78.3% had failed antibiotics. These patients can still be salvaged with appropriate microvascular reconstruction at a tertiary head and neck programme.
Is there a Canadian regulatory framework for hyperbaric chambers?
Yes. Hyperbaric chambers used for medical treatment are regulated as Class III medical devices by Health Canada under the Medical Devices Regulations. Provincial standards for chamber installation typically reference CSA Group standards such as CSA Z275.1 (hyperbaric operations and work in compressed air environments). Patients can be reassured that any facility on our directory operates within this regulatory framework.
Where can I find more information for my patient?
The Canadian Undersea and Hyperbaric Medical Association (CUHMA) is the national professional body for hyperbaric medicine in Canada and maintains patient-facing resources. For research summaries, see our research bank, which indexes thousands of HBOT studies including those cited above. Our FAQ page answers common patient questions in plain language.
The bottom line for Canadian referring physicians
Osteoradionecrosis of the jaw remains a serious late complication of head and neck radiotherapy, and HBOT continues to have a defined place in its prevention and management within a multidisciplinary framework. The 2025-2026 evidence base supports HBOT most strongly for prevention before dental procedures in high-risk patients and for haemorrhagic cystitis; for established mandibular ORN requiring surgical reconstruction, recent comparator data are mixed and decisions should be individualised within a head and neck multidisciplinary team. PENTO and PENTOCLO are credible non-hyperbaric alternatives with supporting evidence. Canada Hyperbarics maintains a directory of hospitals and regulated facilities offering HBOT across the country, and the referral pathway is straightforward when supported by complete radiotherapy and surgical documentation.
This content is for informational purposes only and does not constitute medical advice. Treatment decisions should be made in consultation with the patient’s oncology, maxillofacial, and hyperbaric medicine teams based on individual clinical circumstances.