
TL;DR: A 2026 prospective observational study in J Clin Med (n=90 patients with Fontaine stage IV peripheral arterial disease and chronic ulceration) found that 20 sessions of hyperbaric oxygen therapy at 2.0 to 2.5 ATA significantly reduced platelet reactivity across all three measured pathways (ASPI, ADP, TRAP) independent of antiplatelet therapy, and reduced pain intensity. Ulcer size did not change over the 4-week treatment window. For Canadian referring physicians, HBOT is an adjunct to optimised revascularisation and antiplatelet therapy in selected advanced PAOD patients, not a replacement for either. Canada Hyperbarics maintains a directory of accredited hospitals and regulated facilities offering HBOT across the country.
Hyperbaric oxygen therapy (HBOT) is a medical treatment that delivers 100 percent oxygen at greater than atmospheric pressure inside a sealed chamber. Peripheral arterial disease (PAD), also called peripheral arterial occlusive disease (PAOD), is a chronic atherosclerotic condition characterised by impaired tissue perfusion, chronic ischaemia, and increased platelet reactivity in the lower extremities. Advanced PAOD often progresses to Fontaine stage IV: rest pain accompanied by chronic ulceration or tissue loss. For Canadian referring physicians managing patients in whom revascularisation has been exhausted or is technically infeasible, hyperbaric oxygen therapy (HBOT) is an adjunctive option supported by an expanding evidence base. A 2026 study published in Journal of Clinical Medicine adds a new mechanistic finding: HBOT was associated with measurably lower platelet aggregation in advanced PAOD, independent of antiplatelet therapy. This article summarises that trial, situates it among the broader 2026 wound-healing literature, and outlines how to refer.
What did the 2026 Knezevic study actually find?
The trial (Knezevic et al., 2026, J Clin Med (PubMed)) enrolled 90 patients with Fontaine stage IV PAOD and chronic ulceration, assigned to an HBOT group (n=60) or a waiting-list control group (n=30). Mean age was 66.8 years in the study group and 63.0 years in controls. Diabetes mellitus was present in 55.0 percent and 63.3 percent of the two groups respectively, reflecting the typical comorbidity profile of advanced PAOD. Prior revascularisation included open surgery in roughly one-third of each group and endovascular treatment in another third, with the remaining 26.7 to 30.0 percent having no further revascularisation option.
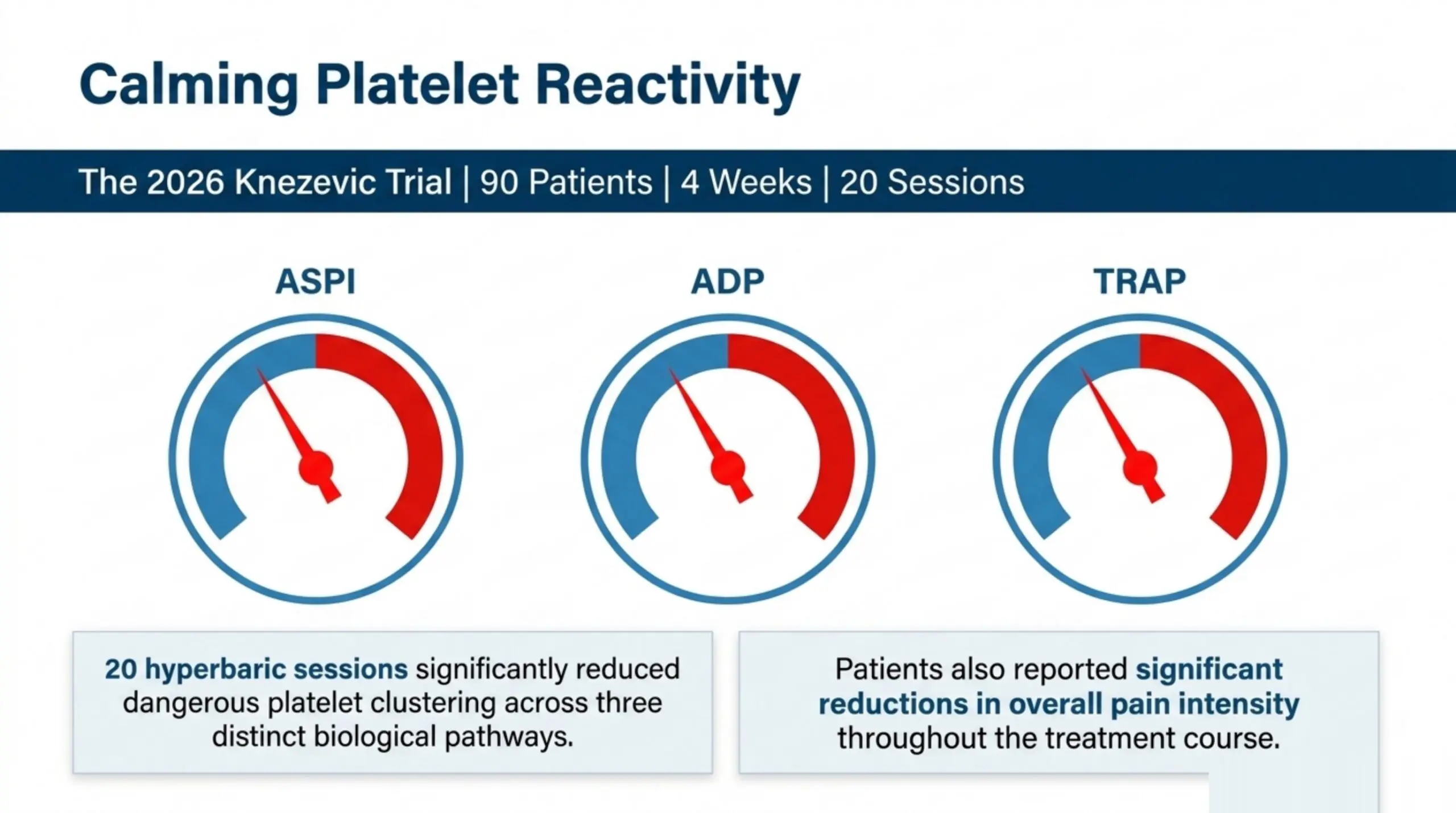
HBOT was delivered over 4 weeks (20 sessions at 2.0 to 2.5 ATA). Platelet aggregation was measured by impedance aggregometry using three agonists: arachidonic acid (ASPI), adenosine diphosphate (ADP), and thrombin-receptor-activating peptide (TRAP). Generalised estimating equation models adjusted for antiplatelet therapy, diabetes mellitus, smoking, and C-reactive protein.
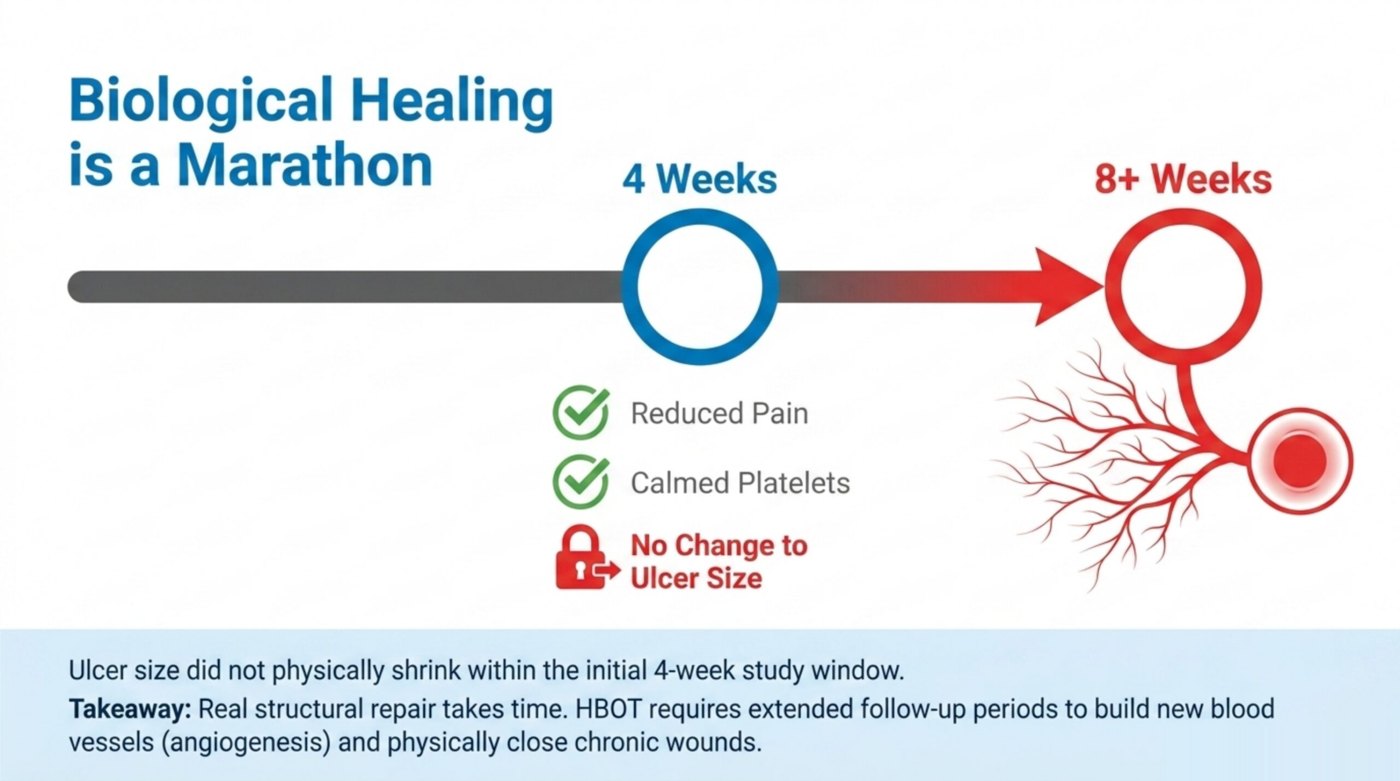
The authors reported significant group × time interactions across all three platelet activation pathways, indicating that HBOT was associated with reduced platelet reactivity independent of background antiplatelet regimens. Patients also reported reduced pain intensity over the treatment course. Notably, ulcer size did not change significantly within the 4-week study window. The investigators frame this as consistent with the timeline of HBOT-mediated angiogenesis and tissue remodelling, which typically extend beyond 4 weeks and require longer follow-up to capture wound-closure endpoints.
How does this fit with the broader 2026 evidence base?
The Knezevic findings sit alongside several relevant 2026 publications indexed in our research database. A 2026 systematic review and network meta-analysis published in Journal of Clinical Medicine (PubMed) pooled 27 randomised controlled trials and 1,673 participants with chronic wounds. In pairwise pooling, gas therapies (including HBOT) significantly increased complete wound healing versus standard care (random-effects risk ratio 2.17, 95 percent confidence interval 1.61 to 2.94), with substantial heterogeneity (I² 75.7 percent). The authors prespecified subgroup analyses suggested effect modification by intervention type and wound aetiology, and the SUCRA ranking in the network analysis was influenced by network structure and between-study factors.
A 2026 structured narrative review in Cureus (PubMed) synthesised clinical evidence on HBOT in surgical wound healing and tissue salvage. The authors reported that clinical evidence supports HBOT use in chronic ischaemic wounds, such as diabetic foot ulcers, venous leg ulcers, burn injuries, and radiation-induced tissue damage, demonstrating improved wound closure rates and reduced infection risk. Mechanistically, HBOT was described as acting through enhanced plasma-dissolved oxygen delivery, angiogenesis stimulation, fibroblast proliferation, collagen synthesis, and immunomodulation.
A 2026 review in Undersea and Hyperbaric Medicine (PubMed) reaffirmed the historical and mechanistic rationale linking hyperbaric oxygen to wound healing, tracing the role of tissue oxygenation in wound repair back to Dr. T.K. Hunt’s foundational 1964 work for the National Science Foundation. The review reiterates that wound healing is dependent on tissue oxygenation, the central biological premise that underpins HBOT use in ischaemic conditions including PAOD-related ulceration.
A 2026 computational modelling study in PLoS One developed both partial-differential-equation and agent-based simulations of ischaemic dermal wound closure under oxygen therapy. The authors reported that standard hyperbaric oxygen therapy and continuous topical oxygen therapy effectively achieved complete wound closure within expected time when ischaemia levels were not too high, but the effect attenuated as the simulated ischaemia parameter increased. This provides a quantitative framework for interpreting why some ischaemic wounds respond rapidly to HBOT while others, with more severe macrovascular compromise, require revascularisation first.
Taken together, the 2026 network meta-analysis is the most important contextual signal: across 27 RCTs and 1,673 patients, gas-based therapies including HBOT roughly doubled the rate of complete chronic-wound healing versus standard care. The authors note substantial heterogeneity and limited evidence certainty under GRADE, however, and the network was sensitive to study-level factors. For the PAOD subset specifically, the direct RCT evidence remains modest, and the Knezevic mechanistic finding addresses a gap by demonstrating a measurable platelet-pathway effect.
Which PAOD patients are candidates for HBOT?
The Undersea and Hyperbaric Medical Society (UHMS) lists chronic, refractory osteomyelitis and selected problem wounds among its recognised indications, with diabetic lower-extremity wounds (Wagner grade III or higher, having failed standard wound care) qualifying under specific criteria. PAOD itself is not a standalone UHMS indication. In practice, PAOD patients access HBOT through the wound-healing pathway, when they meet these criteria:
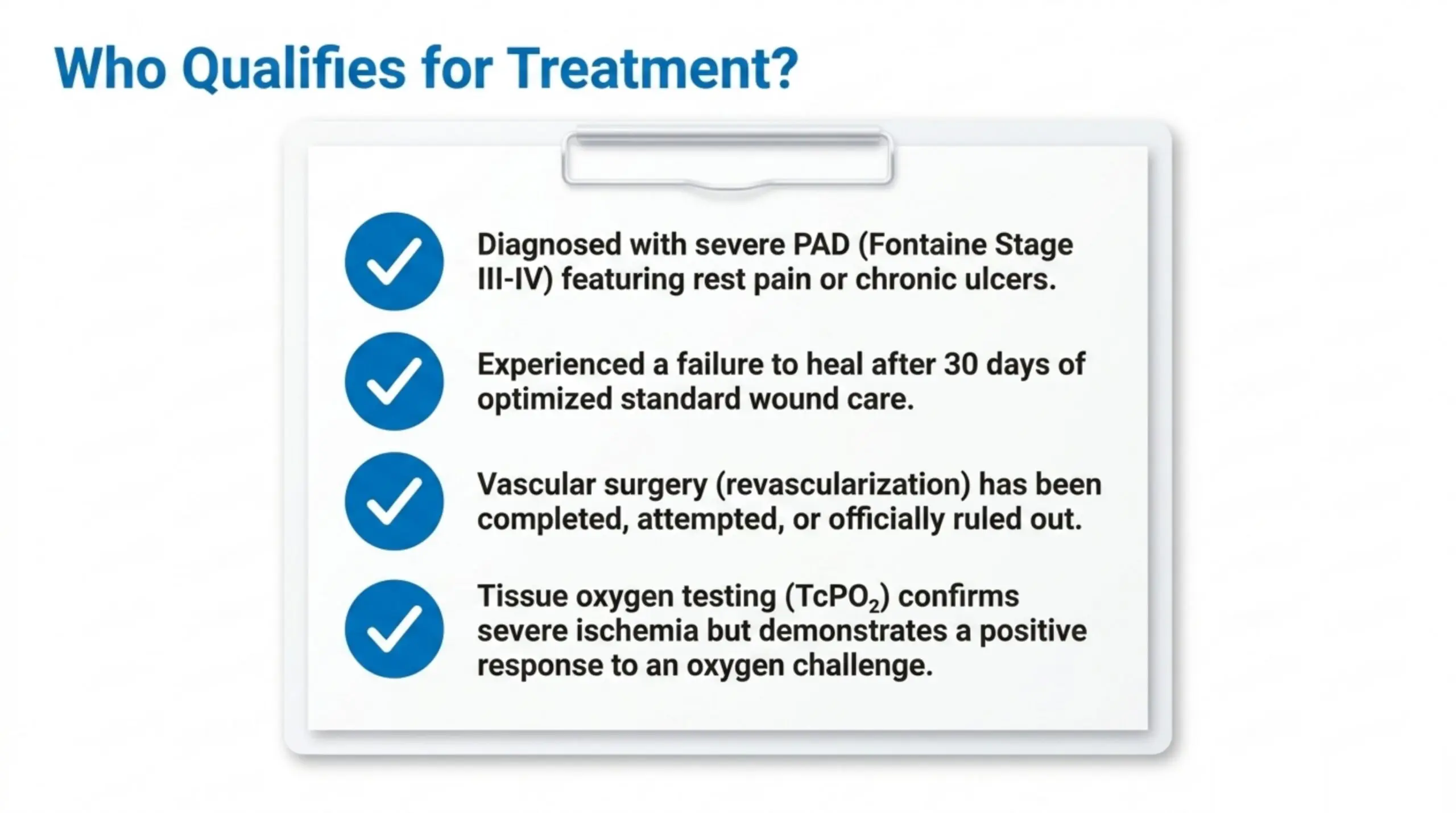
- Confirmed Fontaine III-IV disease with rest pain or chronic ischaemic ulceration that has failed 30 days of optimised standard care.
- Revascularisation status documented: either completed (with persistent ischaemic wound), planned but pending, or not feasible based on vascular surgery assessment.
- Transcutaneous oximetry (TcPO₂) values consistent with ischaemia but with adequate response to oxygen challenge (typical thresholds: baseline TcPO₂ less than 40 mmHg with rise greater than 100 mmHg under hyperbaric oxygen).
- No absolute contraindications: untreated pneumothorax, certain chemotherapeutic agents, severe COPD with bullae, and uncontrolled seizure disorder. Review the full contraindication list before referral.
- Patient able to tolerate 4 to 8 weeks of daily or near-daily sessions, each typically 90 to 120 minutes including compression and decompression.
The Knezevic protocol of 20 sessions at 2.0 to 2.5 ATA over 4 weeks is consistent with standard problem-wound protocols. Patients with concurrent diabetes mellitus may benefit from longer treatment courses, given the slower healing trajectory in that population.
What about antiplatelet therapy and bleeding risk?
One of the most clinically useful aspects of the Knezevic finding is that the platelet-reactivity reduction was statistically independent of antiplatelet therapy. Patients on aspirin, clopidogrel, or dual antiplatelet therapy still showed measurable reductions in ASPI, ADP, and TRAP aggregation after HBOT. The authors framed this as evidence that HBOT acts through a distinct mechanistic pathway, with the analysis specifically adjusting for antiplatelet therapy, diabetes mellitus, smoking, and C-reactive protein in generalised estimating equation models.
From a referral standpoint, this means there is no need to suspend or reduce antiplatelet therapy in patients beginning HBOT. The study did not report increased bleeding events in the HBOT group, although this was an observational design and not powered for that endpoint. Standard practice is to maintain background antiplatelet and statin therapy throughout the HBOT course and review bleeding risk in the usual way before any concurrent invasive procedures.
How do I refer a Canadian patient for HBOT?
The referral pathway depends on the province and on whether the patient qualifies under the local provincial health plan. In Ontario, OHIP covers HBOT for recognised indications (including specified diabetic wound criteria) when delivered at designated hospital programmes. Coverage in other provinces varies by indication and facility. Canada Hyperbarics maintains an updated coverage guide by province. The provincial health plan names referring physicians should use in patient documentation are:
| Province or territory | Provincial health plan name |
|---|---|
| Ontario | OHIP |
| British Columbia | MSP |
| Alberta | AHCIP |
| Quebec | RAMQ |
| Manitoba | Manitoba Health |
| Saskatchewan | Saskatchewan Health |
| Nova Scotia | MSI |
| New Brunswick | Medicare NB |
| Prince Edward Island | PEI Health |
| Newfoundland and Labrador | MCP |
| Northwest Territories, Yukon, Nunavut | Territory-specific plan |
A practical referral sequence for advanced PAOD with chronic ulceration:
- Confirm vascular surgery assessment is complete and revascularisation status is documented in the chart.
- Order TcPO₂ measurement at the wound margin with room-air baseline and oxygen-challenge values.
- Document failure of 30 days of optimised standard wound care (debridement, off-loading, infection management, glycemic control).
- Send a referral letter to the nearest HBOT programme. Include the imaging, vascular assessment, TcPO₂ values, wound photographs, current medications, and relevant past medical history. The facility directory lists current HBOT programmes including hospital-based and accredited private centres.
- Continue co-management during treatment, including weekly wound assessment, medication review, and management of any HBOT-related side effects (most commonly middle-ear barotrauma and transient myopia).
For up-to-date Canadian guidance, consult Health Canada for medical device and approved-indication updates, and the Canadian Undersea and Hyperbaric Medical Association (CUHMA) for accreditation and clinical-practice resources.
What are the limitations of the current evidence?
The Knezevic study is a prospective observational design, not a randomised controlled trial. The control group was a waiting-list cohort rather than a sham-treated group, and platelet-function measurements are a surrogate endpoint rather than a hard clinical outcome (limb salvage, amputation-free survival, mortality). The 4-week timeframe is shorter than the typical HBOT wound-healing trajectory, which is why ulcer-size change was not detected within the study window. Longer follow-up trials, ideally randomised with blinded assessment and validated patient-reported outcomes, are needed to confirm whether the platelet-reactivity finding translates into improved wound-healing and limb-salvage rates.
The 2026 gas-therapies network meta-analysis noted substantial between-study heterogeneity (I² 75.7%) and reported low-to-moderate evidence certainty under GRADE. SUCRA ranking in the network was influenced by the specific structure of available trials, and the authors recommended further well-designed RCTs for the chronic-wound population overall, including the PAOD subset.
Frequently asked questions from referring physicians
Is HBOT a first-line treatment for PAOD?
No. Standard care for PAOD remains risk-factor management (smoking cessation, statins, antiplatelet therapy, glycemic control), supervised exercise where appropriate, and revascularisation (endovascular or surgical) for symptomatic disease. HBOT is an adjunct considered in selected advanced cases, particularly Fontaine III-IV disease with chronic ischaemic ulceration after revascularisation has been optimised or deemed infeasible.
Does HBOT replace revascularisation?
No. Revascularisation remains the priority intervention for restoring macrovascular perfusion. HBOT is considered after revascularisation has been completed, attempted, or formally ruled out by a vascular surgeon. The Knezevic cohort reflected this pattern: roughly 70 percent of patients had undergone prior revascularisation before HBOT.
Should antiplatelet therapy be paused during HBOT?
No. The 2026 Knezevic data indicate that the HBOT effect on platelet reactivity is statistically independent of background antiplatelet therapy. Maintain aspirin, clopidogrel, or dual antiplatelet therapy as clinically indicated, and manage bleeding risk for any concurrent procedures using standard criteria.
What is the typical session schedule?
For chronic ischaemic wounds the standard protocol is 20 to 40 sessions at 2.0 to 2.5 ATA, 90 to 120 minutes per session, daily or near-daily. The Knezevic protocol was 20 sessions over 4 weeks. Some programmes extend to 30 or 40 sessions when wound healing has begun but is incomplete at the 20-session reassessment.
What is the most common side effect to warn patients about?
Middle-ear barotrauma is the most common HBOT side effect. It is managed with equalisation training, decongestants if appropriate, and occasional myringotomy in refractory cases. Transient myopia is the second most common, typically resolves within weeks of treatment completion, and is more frequent in longer treatment courses. Less common but more serious events (oxygen toxicity seizure, pulmonary toxicity, claustrophobia requiring termination) are reviewed during the pre-treatment workup.
How is HBOT funded for Canadian PAOD patients?
Coverage varies by province and indication. OHIP, MSP, AHCIP, RAMQ, Manitoba Health, MSI, Saskatchewan Health, Medicare NB, PEI Health, and MCP all cover HBOT for certain recognised indications at designated hospital programmes. Off-label or out-of-criteria PAOD use is often delivered at accredited private facilities on a self-pay or private-insurance basis. Confirm coverage before referral. See our coverage guide and FAQ for current information.
Where can I find a current list of accredited HBOT centres in Canada?
Canada Hyperbarics maintains a directory of hospitals and regulated facilities offering HBOT, sortable by province. The directory is updated regularly and includes hospital-based programmes and accredited private centres.
Bottom line for referring physicians
The 2026 Knezevic study adds a useful mechanistic data point to the growing HBOT-for-ischaemic-wound evidence base: in advanced PAOD with chronic ulceration, 4 weeks of HBOT at 2.0 to 2.5 ATA reduced platelet reactivity across three independent aggregation pathways and reduced pain intensity, with the analysis adjusting for antiplatelet therapy. Ulcer size did not change in the 4-week window, which the authors describe as expected given the slower trajectory of HBOT-mediated angiogenesis. Combined with the 2026 network meta-analysis showing roughly doubled chronic-wound-healing rates with gas-based therapies including HBOT, the evidence supports HBOT as an adjunct in selected advanced PAOD patients who have exhausted or are not candidates for revascularisation. Referrals are most appropriate after Fontaine III-IV disease with rest pain or chronic ulceration is documented, TcPO₂ assessment confirms ischaemia with adequate oxygen response, and 30 days of optimised standard care has been delivered without satisfactory progress. Patient access is through the network of hospitals and regulated facilities indexed by Canada Hyperbarics.
This content is for informational purposes only and does not constitute medical advice. Clinicians should exercise their own judgement and consult current guidelines and the relevant provincial regulatory authority. Patients should consult a qualified healthcare professional regarding their specific circumstances.