
TL;DR: Hyperbaric oxygen therapy (HBOT) is a treatment that delivers 100 percent oxygen inside a pressurised chamber. The HBOT indications in Canada come from two separate but related lists. Health Canada’s framework recognises 14 conditions tied to hyperbaric chamber licensing and public coverage, while the Undersea and Hyperbaric Medical Society (UHMS) recognises 15 indications in its 15th Edition manual (2024), which added avascular necrosis. Health Canada is a device regulator, and the UHMS is a scientific society that recognises indications rather than approving them. For referring physicians, the practical decision turns on three things: whether the condition is on a recognised list, how urgent it is, and where an accredited facility can deliver treatment. This 2026 guide from Canada Hyperbarics maps those lists to real referral decisions.
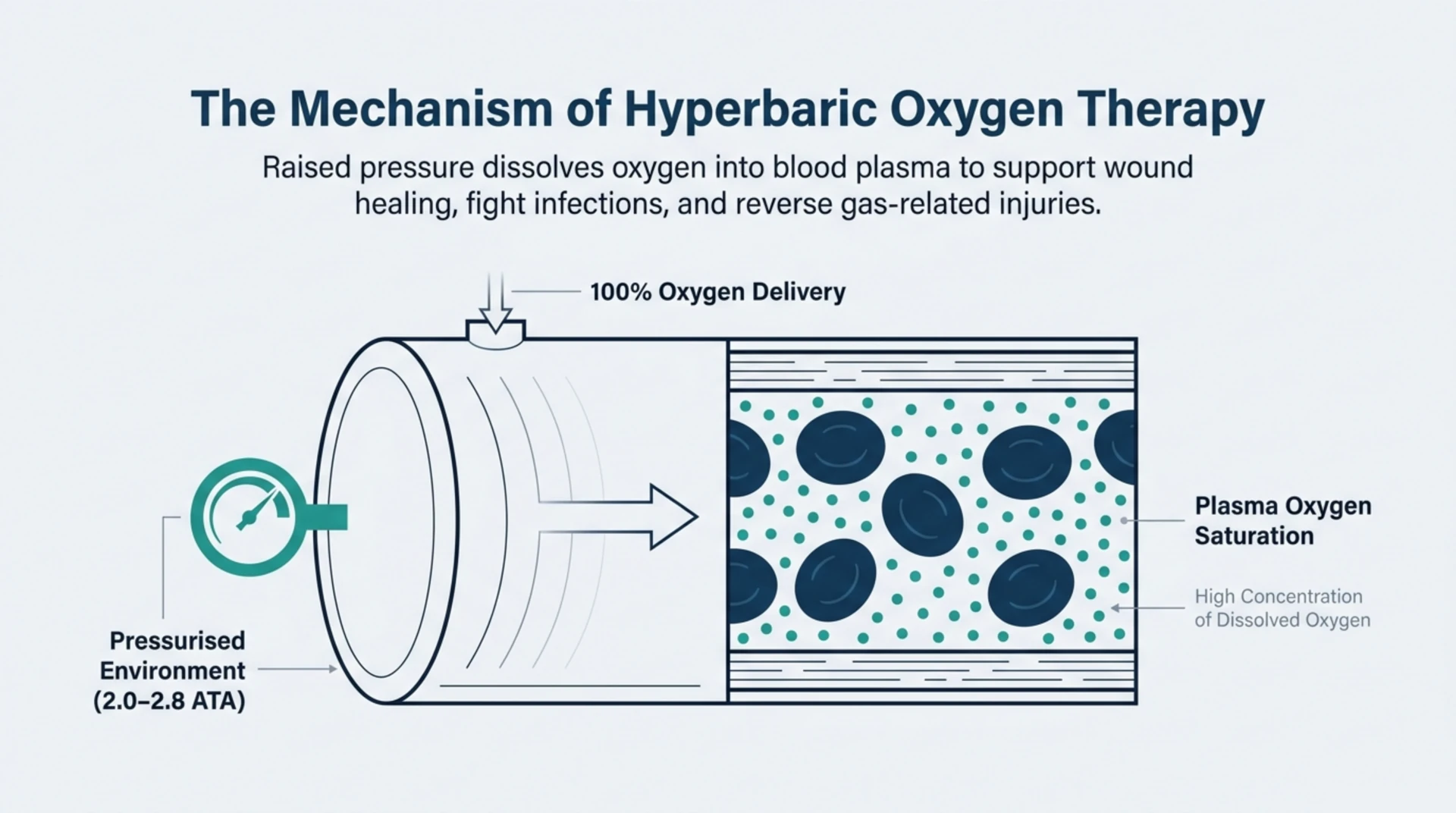
Hyperbaric oxygen therapy (HBOT) is a medical treatment in which a patient breathes 100 percent oxygen inside a pressurised chamber at pressures above sea level, usually 2.0 to 2.8 atmospheres absolute (ATA). The raised pressure dissolves far more oxygen into blood plasma, which supports wound healing, fights certain infections, and reverses gas-related injuries. For Canadian referring physicians, the first question is rarely “does HBOT work” in the abstract. It is “is this specific condition a recognised indication, and how do I refer.” Understanding the HBOT indications in Canada is the key to answering both. Reading time: about 10 minutes.
What are the recognised HBOT indications in Canada?
In the Canadian context, the reference list most physicians work from is the set of 14 conditions publicly funded in Canada for hyperbaric chamber licensing and reflected in provincial public funding, such as the 14 indications covered by OHIP in Ontario. Health Canada does not license hyperbaric clinics or run a formulary. It regulates the hyperbaric chamber itself as a medical device, and its public guidance directs clinicians to the UHMS indications while cautioning against unproven off-label use.
These 14 recognised conditions include the emergencies most physicians associate with HBOT, along with several chronic indications. The recognised list covers air or gas embolism, carbon monoxide poisoning, clostridial gas gangrene, crush injury and acute traumatic ischaemia, decompression sickness, exceptional blood loss anaemia, necrotising soft tissue infections, refractory osteomyelitis, soft tissue radiation necrosis, radiation damage affecting bone, compromised skin grafts and flaps, thermal burns, sudden sensorineural hearing loss, and non-healing wounds such as diabetic foot ulcers. You can review each of these on the Canada Hyperbarics conditions index.
How does the UHMS Indications list differ from Health Canada’s?
The Undersea and Hyperbaric Medical Society (UHMS) is a scientific and professional society, not a regulator or a government body. It publishes the Hyperbaric Medicine Indications Manual, now in its 15th Edition (2024), which recognises 15 indications. The most important recent change is that avascular necrosis was added as a recognised indication in the 15th Edition. Because the UHMS reviews the global clinical evidence, its list is broader than Canada’s 14-condition framework and is updated on its own schedule.
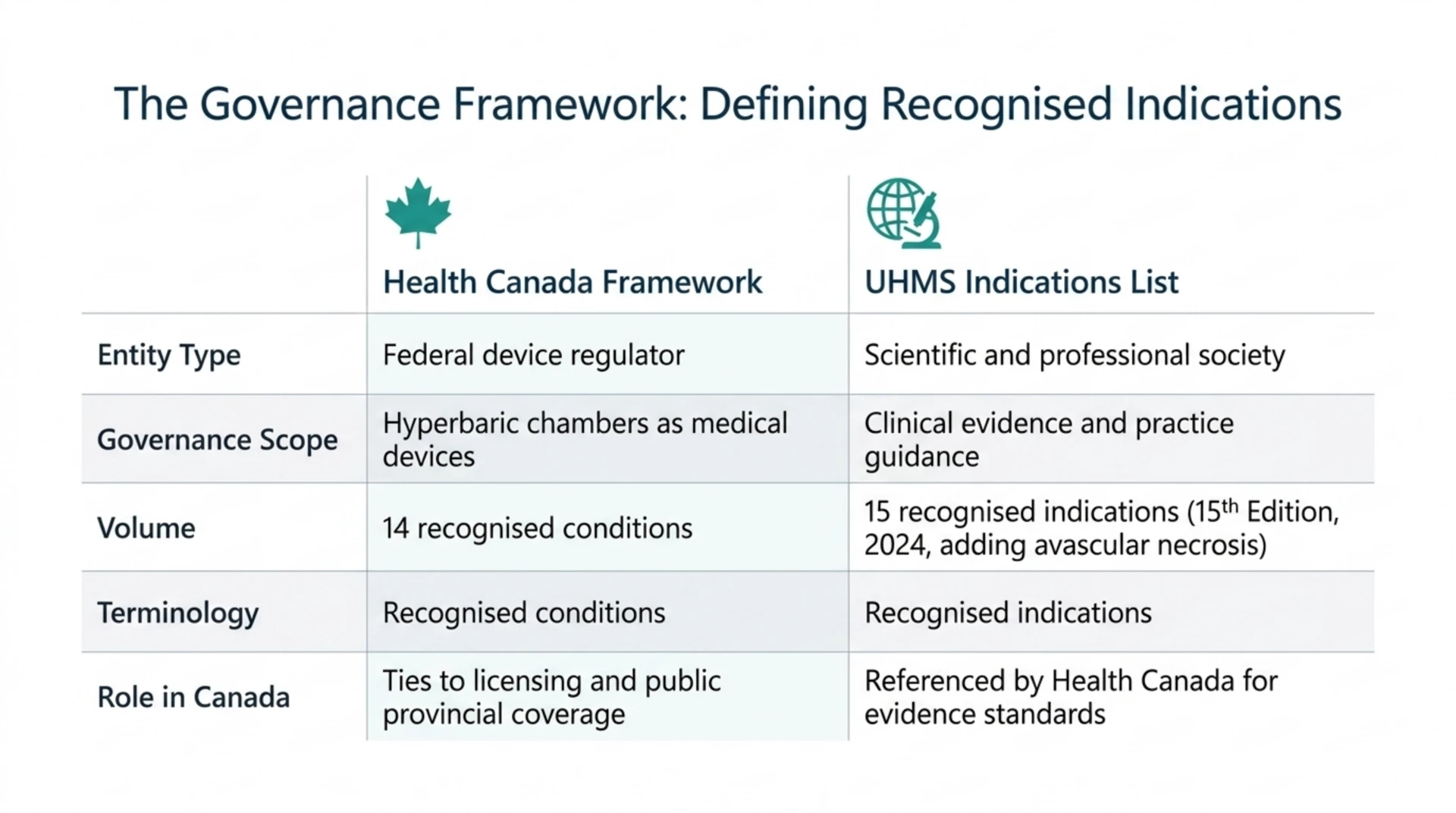
The wording here matters. The UHMS recognises indications based on evidence review. It does not “approve” them, and it does not regulate hyperbaric practice in Canada. Health Canada and the UHMS maintain two separate lists that partially overlap, so it is inaccurate to lump them together as a single “approved” list. The table below summarises the difference.
| Feature | Health Canada framework | UHMS Indications list |
|---|---|---|
| Type of body | Federal device regulator | Scientific and professional society |
| What it governs | Hyperbaric chambers as medical devices | Clinical evidence and practice guidance |
| Number of conditions | 14 recognised conditions | 15 recognised indications (15th Edition, 2024) |
| Language used | Recognised conditions | Recognised indications |
| Role in Canada | Ties to licensing and public coverage | Referenced by Health Canada for evidence |
Canadian practice standards are shaped further by the Canadian Undersea and Hyperbaric Medical Association (CUHMA), which promotes education and best practice for hyperbaric and diving medicine in Canada. Health Canada’s device-licensing framework references the UHMS indications rather than CUHMA when it evaluates applications, so a referring physician should treat the UHMS list as the evidence reference and CUHMA as the Canadian professional community.
How should the indication lists guide a referral decision?
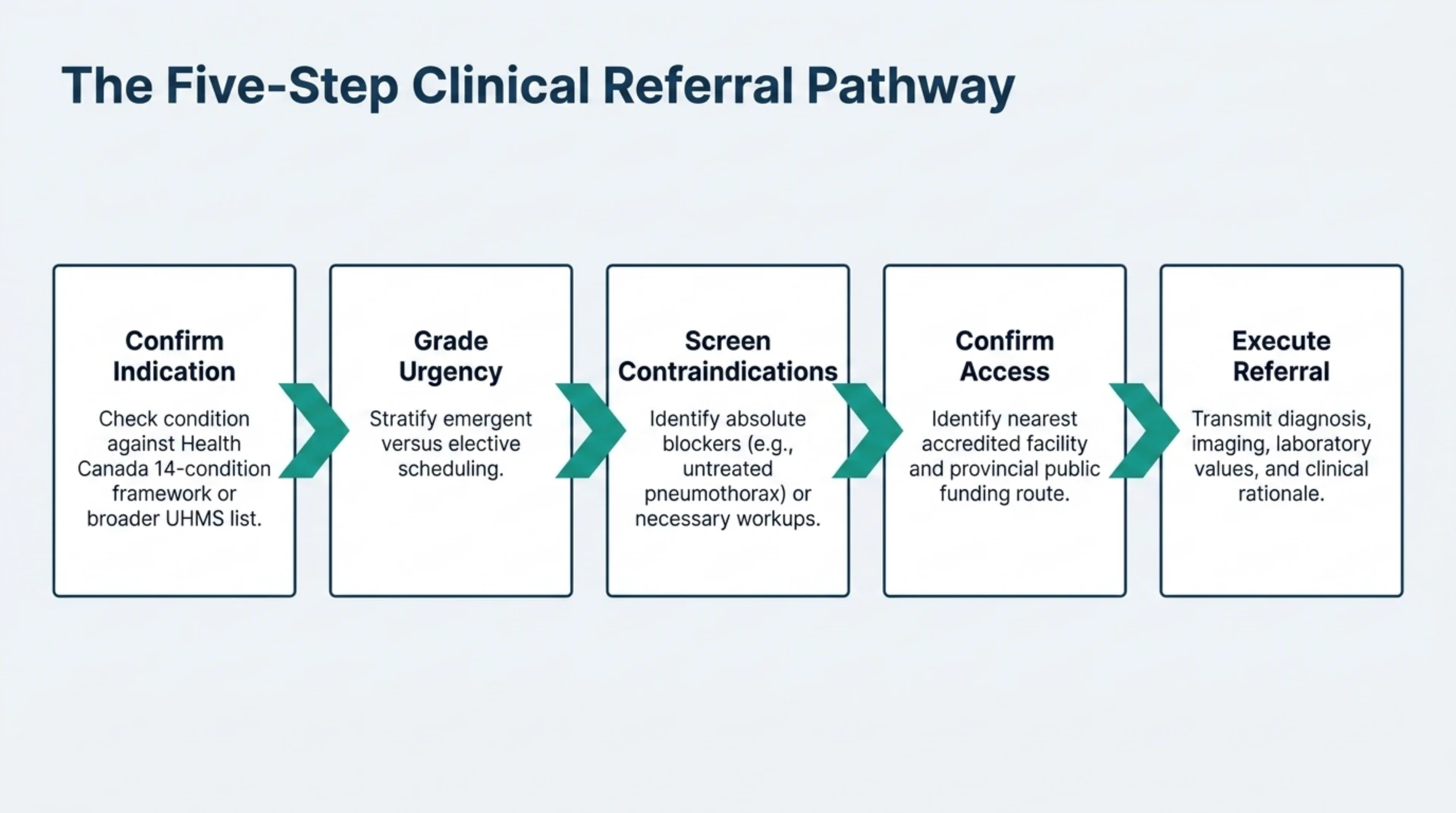
Knowing the lists is only the starting point. A clean HBOT referral follows a short, repeatable sequence. Working through these steps helps you decide not just whether to refer, but how quickly.
- Confirm the indication is recognised. Check whether the condition appears on the Health Canada 14-condition framework or the broader UHMS list. Recognised indications have the clearest evidence and the smoothest coverage pathway.
- Grade the urgency. Emergent indications such as arterial gas embolism, decompression sickness, severe carbon monoxide poisoning, clostridial gas gangrene, and central retinal artery occlusion need same-day contact with a hyperbaric facility. Chronic indications such as diabetic foot ulcers, delayed radiation injury, and refractory osteomyelitis are scheduled electively.
- Screen for contraindications. An untreated pneumothorax is an absolute contraindication, and several conditions require workup before treatment. Document these in the referral.
- Confirm the access and coverage pathway. Identify the nearest accredited facility and the correct provincial coverage route before the patient travels.
- Send a complete referral. Include the diagnosis, relevant imaging or laboratory values, and the clinical reason HBOT is being considered.
The urgency step is where the indication lists become most useful at the bedside. One 2026 retrospective cohort of 272 patients with carbon monoxide poisoning found that lower Glasgow Coma Scale scores, ischaemic ECG findings, and lactate levels were independently associated with the decision to select hyperbaric oxygen therapy over normobaric oxygen (Yüceer, PubMed | Our Assessment). In practice, the sicker the patient, the faster the escalation.
What does recent evidence show for the recognised indications?
Being on a recognised list does not mean the evidence is uniform across every indication. Referring physicians serve patients best by matching the strength of the recommendation to the strength of the underlying study design. Recent 2026 research illustrates the range.
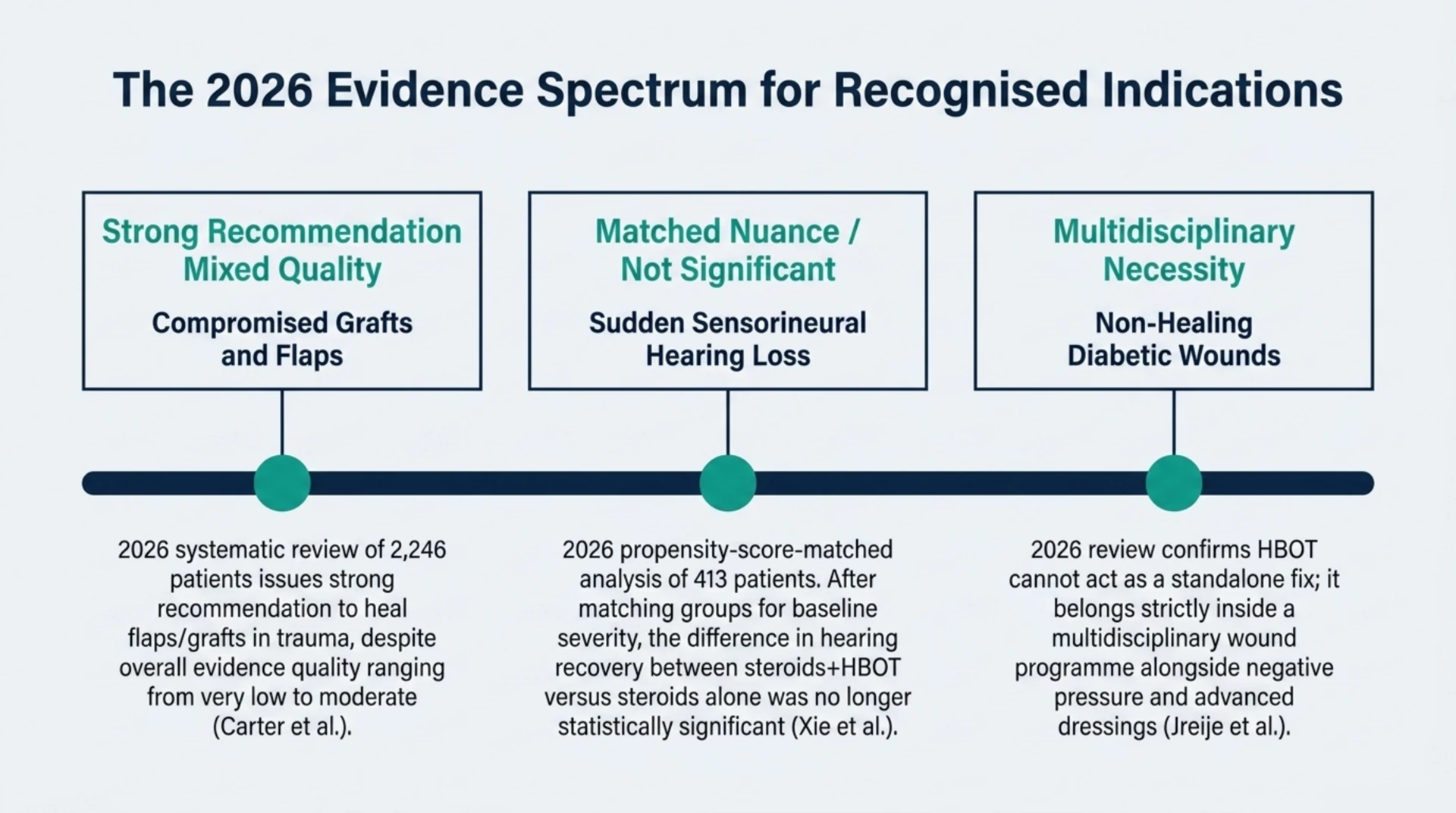
For compromised grafts and flaps, a 2026 systematic review of 24 comparative studies (including 13 randomised controlled trials and 2,246 patients) issued a strong recommendation to use HBOT to heal flaps and grafts in soft tissue injury and trauma wounds, while noting that the overall quality of evidence ranged from very low to moderate (Carter and colleagues, PubMed | Our Assessment). That combination, a strong recommendation resting on mixed-quality evidence, is common in hyperbaric medicine and worth conveying honestly to patients.
For delayed radiation injury, a 2026 review of 43 patients treated for chronic radiation cystitis reported that HBOT was associated with resolution of gross haematuria in 60 percent of patients by 20 treatments, 79 percent by 40 treatments, and 100 percent by 60 treatments, and that hospital admissions for bleeding fell from 1.2 per year before treatment to 0.3 per year afterward (Booher and colleagues, PubMed | Our Assessment). Because this was a single-arm observational study, the findings are best described as an association rather than proof of cause.
For sudden sensorineural hearing loss, the picture is more nuanced. A 2026 propensity-score-matched analysis of 413 patients compared steroids plus HBOT against steroids alone. Before matching, the two groups differed significantly in hearing recovery, but after they were balanced for baseline severity, the difference in overall hearing recovery was no longer statistically significant (Xie and colleagues, PubMed | Our Assessment). This is a reminder that a recognised indication can still carry uncertainty about the size of the benefit.
For non-healing diabetic wounds, a 2026 review of diabetic wound biology examined HBOT alongside negative pressure therapy, advanced dressings, and regenerative strategies, and concluded that no single modality fully addresses the multifactorial nature of diabetic wounds (Jreije and colleagues, PubMed | Our Assessment). The practical message is that HBOT belongs inside a multidisciplinary wound programme, not as a standalone fix.
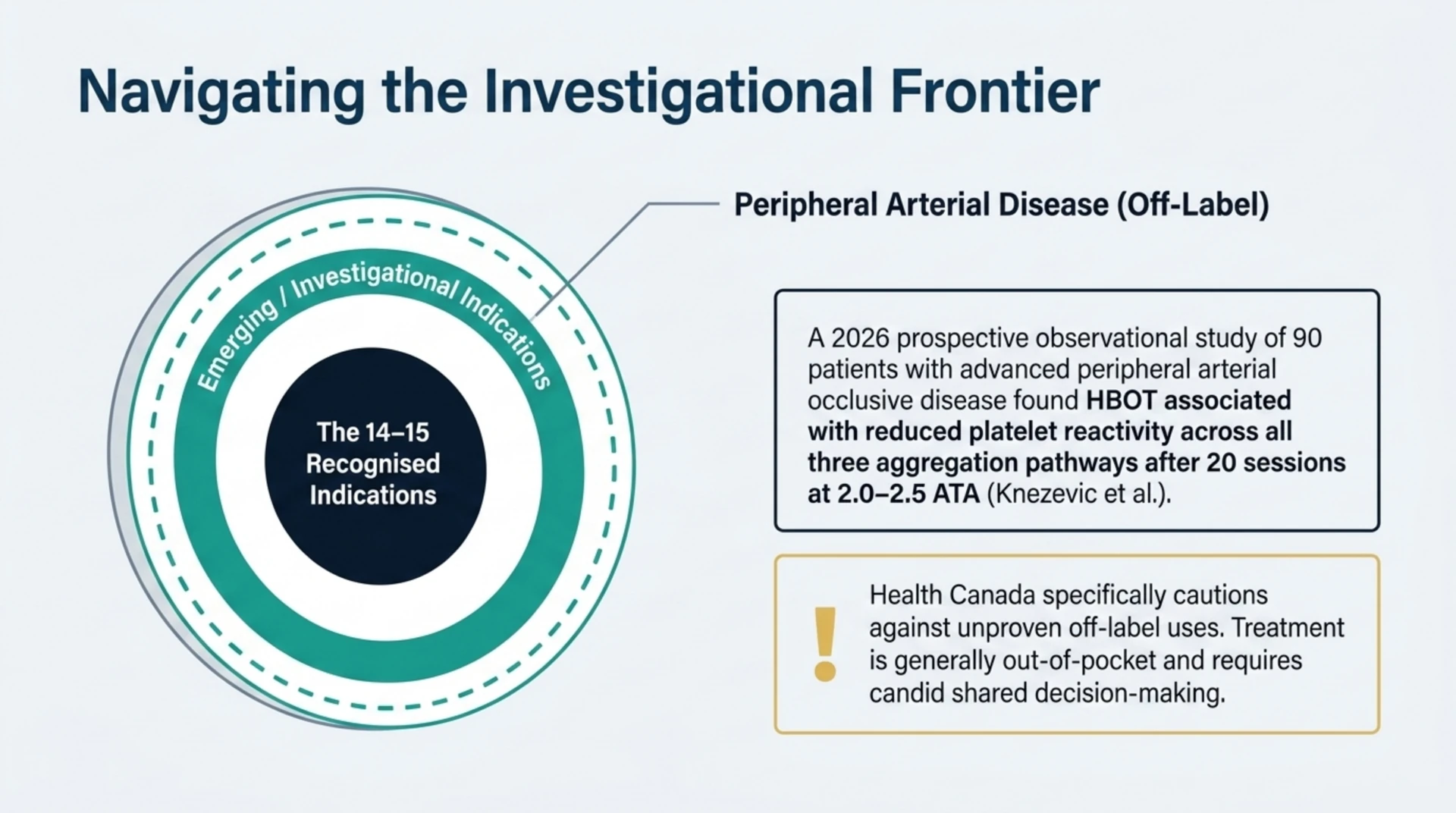
Where do emerging indications like peripheral arterial disease fit?
Beyond the recognised lists sit a large group of emerging or investigational uses. These are conditions where early research is promising but the evidence does not yet support routine coverage. Peripheral arterial disease is a good example. A 2026 prospective observational study of 90 patients with advanced peripheral arterial occlusive disease found that HBOT was associated with reduced platelet reactivity across all three tested aggregation pathways after 20 sessions at 2.0 to 2.5 ATA (Knezevic and colleagues, PubMed | Our Assessment).
The word “associated” is deliberate. This was an observational study, not a randomised controlled trial, so it can show a relationship but not prove that HBOT caused the change. When you discuss an emerging indication with a patient, it is important to be clear that treatment would be off-label, likely not publicly funded, and best pursued through a research setting or a candid shared decision. Health Canada’s guidance specifically cautions against off-label uses that have not been proven effective.
How do referring physicians access HBOT across Canada?
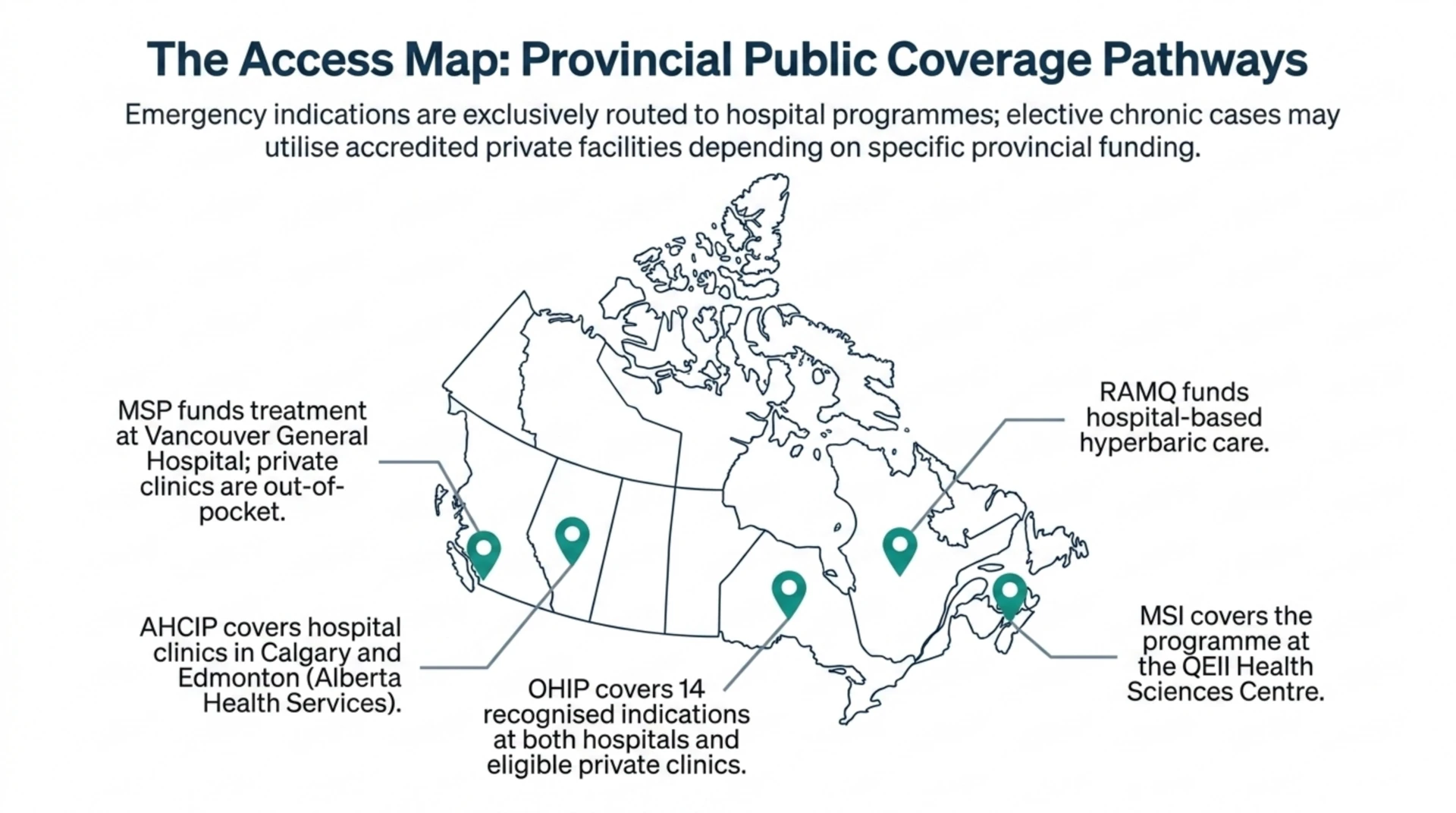
Access to hyperbaric oxygen therapy in Canada runs through a mix of hospitals and regulated facilities, and public coverage varies by province. Emergency indications are handled by hospital hyperbaric programmes, while chronic wound and radiation cases may be treated at hospital or accredited private facilities depending on the province.
In Ontario, OHIP covers the 14 recognised indications at both hospitals and eligible private clinics that bill OHIP for those indications. In British Columbia, MSP funds treatment at Vancouver General Hospital, and private-clinic care is out of pocket. In Alberta, AHCIP covers treatment at Alberta Health Services hospital clinics in Calgary and Edmonton. In Quebec, RAMQ funds hospital-based hyperbaric care, and in Nova Scotia, MSI covers the programme at the QEII Health Sciences Centre. To find the nearest option, use the Canada Hyperbarics directory of hospitals and regulated facilities and confirm the coverage route before the patient travels.
Frequently asked questions about HBOT indications in Canada
How many HBOT indications are recognised in Canada?
Health Canada’s framework recognises 14 conditions for hyperbaric chamber licensing and public coverage, and this is the list reflected in provincial funding such as OHIP’s 14 covered indications. The UHMS recognises 15 indications in its 15th Edition manual, which is broader because it added avascular necrosis in 2024.
Is HBOT “Health Canada approved” for these conditions?
Not in the way that phrase suggests. Health Canada licenses the hyperbaric chamber as a medical device rather than approving specific clinics or a formulary of indications. The recognised conditions come from the licensing and coverage framework, and Health Canada points clinicians to the UHMS indications for the underlying evidence.
What is the difference between a recognised and an emerging indication?
A recognised indication appears on the Health Canada or UHMS list, has stronger evidence, and typically has a coverage pathway. An emerging indication, such as peripheral arterial disease, is still under investigation, would usually be treated off-label, and is generally not publicly funded.
Which HBOT referrals are emergencies?
Arterial gas embolism, decompression sickness, severe carbon monoxide poisoning, clostridial gas gangrene, and central retinal artery occlusion are time-critical and need same-day contact with a hyperbaric facility. Chronic wound, radiation injury, and osteomyelitis cases are referred electively.
Does provincial insurance cover HBOT?
Coverage varies by province. Ontario’s OHIP covers the recognised indications at hospitals and eligible private clinics, while British Columbia, Alberta, Quebec, and Nova Scotia fund hospital-based programmes. Several provinces have no confirmed public coverage for private-clinic care, so confirm the pathway before referring.
Where can I read the evidence behind each indication?
The Canada Hyperbarics research library keeps a structured summary of thousands of peer-reviewed studies, each with our own assessment and a link to the primary source. You can also review the frequently asked questions or the conditions index for plain-language overviews to share with patients.
Make the referral with confidence
Understanding the HBOT indications in Canada turns a vague “maybe hyperbaric” into a clear, defensible referral. Confirm the indication is recognised, grade the urgency, screen for contraindications, and route the patient to an accredited facility. To locate the nearest option and confirm the coverage pathway, explore the Canada Hyperbarics directory of hospitals and regulated facilities.
This content is for informational purposes only and does not constitute medical advice. Treatment decisions should be made in consultation with a qualified healthcare professional. Hyperbaric oxygen therapy should be delivered at accredited facilities under appropriate medical supervision.