
Reading time: about 11 minutes. Written for plastic, reconstructive, vascular, orthopaedic, oral and maxillofacial, and general surgeons practising in Canada.
TL;DR: Hyperbaric oxygen therapy (HBOT) is an evidence-based adjunct for selected surgical wounds, compromised flaps and grafts, and tissue-salvage cases. A 2026 systematic review of comparative studies (Carter et al., 2,246 patients) gave a strong recommendation for HBOT in skin flap and graft surgical indications for soft-tissue injury and trauma wounds. This guide gives Canadian surgeons a step-by-step referral pathway: when to refer, how to screen, how to find a regulated facility, and how to co-manage the patient through 20 to 40 sessions.
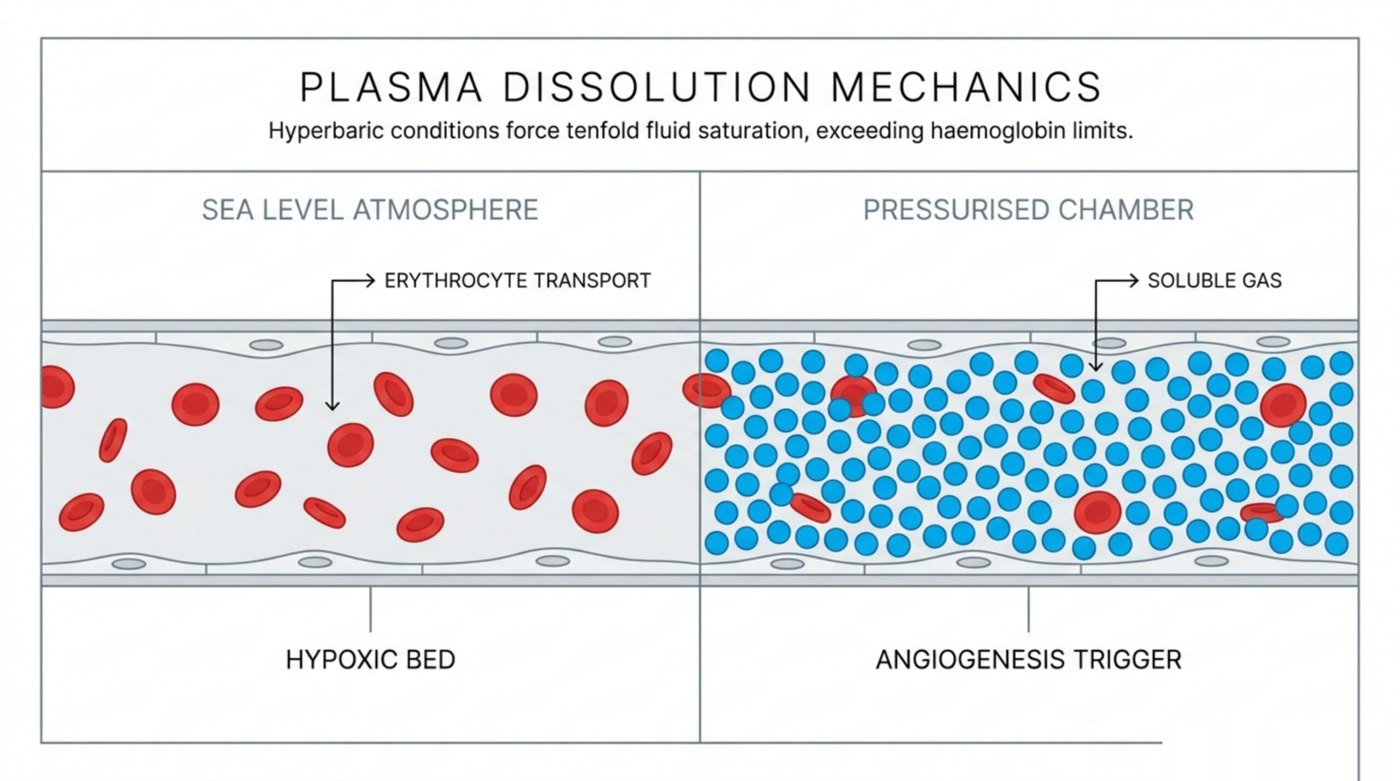
Hyperbaric oxygen therapy is a treatment in which a patient breathes 100% oxygen inside a pressurised chamber at 2.0 to 2.5 atmospheres absolute (ATA). The increased ambient pressure dissolves roughly 10 to 20 times more oxygen in plasma than breathing room air at sea level, raising tissue oxygen tension and supporting angiogenesis, fibroblast proliferation, collagen deposition, neutrophil-mediated bacterial killing, and modulation of the inflammatory response. For surgical wounds where conventional debridement, antibiotics, and reconstruction have not produced the expected healing trajectory, these mechanisms can shift the tissue-oxygen environment far enough to salvage compromised tissue.
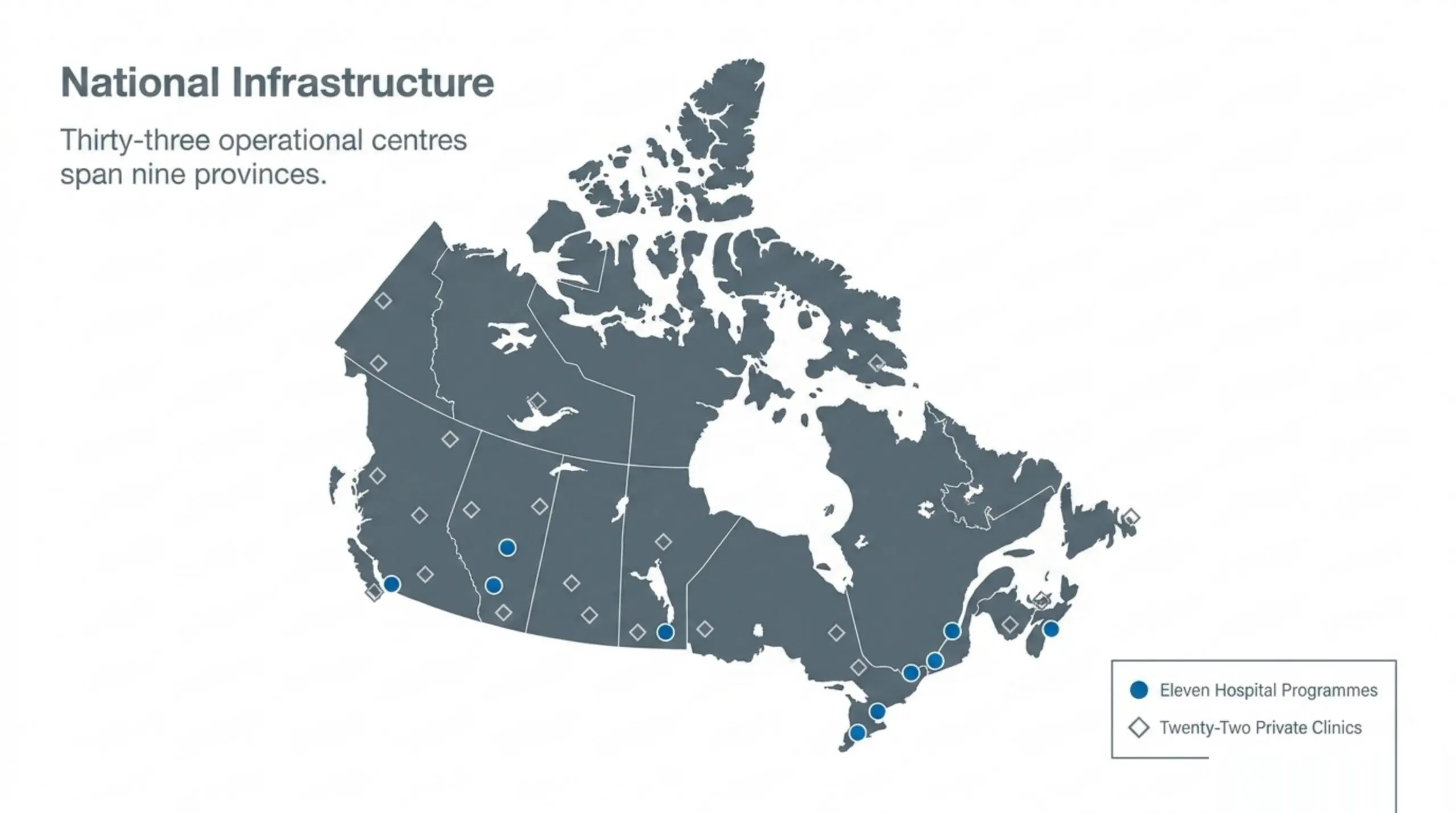
Canada Hyperbarics maintains the country’s most complete directory of hospitals and regulated facilities that deliver HBOT, currently 33 facilities across 9 provinces (11 hospital-based programmes and 22 private clinics). This guide gives referring surgeons a practical, evidence-anchored workflow for getting the right surgical-wound patient into the right facility quickly.
When should I consider HBOT for a surgical patient?
HBOT for surgical wound healing falls into two broad referral windows: prophylactic perioperative use in a known-hypoxic surgical bed, and salvage use when post-operative healing has stalled or failed. The strongest 2026 evidence supports both windows for selected indications, but the threshold for referral differs.
A 2026 structured narrative review of HBOT in surgical wound healing and tissue salvage (González Flores et al., PubMed | Our Assessment) summarised the mechanistic case and the clinical indications across diverse surgical contexts. The authors synthesised evidence for compromised grafts, ischaemic flaps, traumatic soft-tissue injuries, breast reconstruction salvage, chronic ischaemic wounds, burns, and radiation-induced tissue damage, reporting enhanced tissue viability and reduced necrosis progression across the literature.
The following table summarises the surgical scenarios most commonly referred to Canadian HBOT facilities and how urgent the referral typically is. Use it as a triage prompt, not a substitute for a hyperbaric medicine consultation.
| Surgical scenario | Typical referral window | Evidence base |
|---|---|---|
| Compromised skin graft or flap (ischaemia, partial necrosis) | Within 24 to 72 hours of recognising compromise | Strong recommendation in 2026 systematic review (Carter et al.) |
| Acute traumatic soft-tissue injury considered for flap/graft | Pre-operatively or within 24 hours of reconstruction | Strong recommendation (Carter et al.) |
| Necrotising soft-tissue infection (post-debridement adjunct) | Urgent, within 24 hours | UHMS-recognised indication; supported in adjunctive reviews |
| Refractory osteomyelitis after surgical debridement | Elective, after orthopaedic consultation | UHMS-recognised indication |
| Delayed radiation injury affecting a surgical bed | Elective; typically pre- and post-operative protocols | UHMS-recognised indication |
| Breast reconstruction with scarring defects post-mastectomy | As early as possible after recognising delayed healing | 2026 retrospective study (Najib et al.) |
| Complex rhinoplasty defects with compromised vascularity | Peri-operative, before composite-graft failure | 2026 narrative review (Toriumi) |
| Oral and maxillofacial bone regeneration after augmentation | Elective adjunct; case-by-case | 2026 systematic review (Gäde et al.) |
| Adjunct in high-energy avulsive facial injury reconstruction | Per multidisciplinary protocol | 2026 protocol update (Pepper et al.) |
Two principles deserve emphasis. First, time matters. A 2026 retrospective study of 39 women receiving HBOT for scarring defects after reconstructive breast surgery (Najib et al., PubMed | Our Assessment) found that favourable wound healing was associated with a shorter interval between surgery and HBOT initiation. Second, the indication matters more than the operation. A flap with compromised vascularity is a flap with compromised vascularity whether the surgery was breast reconstruction, rhinoplasty, ACL graft fixation, or maxillofacial trauma; the underlying tissue-oxygen rationale is the same.
What does the 2026 evidence base actually look like?
The most recent and methodologically strongest synthesis is a 2026 systematic review of comparative studies evaluating HBOT on skin flap and graft surgical indications (Carter et al., PubMed | Our Assessment). The review pooled 25 reports from 24 studies (13 RCTs and 11 non-RCTs, 2,246 patients). Meta-analysis of four RCTs evaluating flap and graft survival within 4 weeks of HBOT (2 to 2.5 ATA) produced a large overall effect (log odds ratio 1.045, 95% CI 0.44 to 1.65, P < 0.001). The authors issued 11 strong and 13 conditional recommendations, including a strong recommendation to use HBOT for flaps and grafts in soft-tissue injury and trauma wounds.
For broader chronic wound healing, a 2026 systematic review and network meta-analysis of gas therapies for chronic wounds (Zheng et al., PubMed | Our Assessment) included 27 RCTs with 1,673 participants. Pairwise pooling found that gas therapies were associated with significantly higher complete-healing rates versus standard care (random-effects RR 2.17, 95% CI 1.61 to 2.94), with substantial heterogeneity (I² = 75.7%). The network meta-analysis was more nuanced; the authors noted that SUCRA ranking placed standard care highest, a finding they attributed to network structure and between-study heterogeneity rather than a true reversal of effect. Surgeons should read the full paper before applying NMA point estimates to individual cases.
Sub-specialty evidence has also matured rapidly through 2026:
- Plastic surgery: A 2026 narrative review of HBOT in secondary rhinoplasty (Toriumi, PubMed | Our Assessment) described its role in complex rhinoplasty defects involving compromised vascularity, the use of flaps or composite grafts, and cases with prior infection.
- Oral and maxillofacial surgery: A 2026 systematic review of hypoxia and tissue regeneration in oral and maxillofacial surgery (Gäde et al., PubMed | Our Assessment) concluded that hyperbaric oxygen treatment consistently improved bone healing across the included studies.
- Sports medicine: A 2026 matched cohort study of HBOT after ACL reconstruction with hamstring autografts (Leite et al., PubMed | Our Assessment) reported significantly lower graft signal-to-noise quotient on 4-month MRI in the HBOT group versus matched controls (median difference 83.9, P = 0.031), suggesting improved early graft maturation. This is a Level 3 cohort study, so the finding is an association rather than a randomised causal claim.
- Reconstructive trauma: A 2026 management-protocol update for ballistic and high-energy avulsive facial injuries (Pepper et al., PubMed | Our Assessment) lists HBOT among the adjuncts that further optimise recovery in the four-phase resuscitation, reconstitution, reconstruction, and rehabilitation protocol.
- Adjunct in infected surgical wounds: A 2026 review of the adjunctive role of HBOT in microbial infection-related conditions (Zhang et al., PubMed | Our Assessment) supports adjunctive use in complex infections including diabetic foot wounds and necrotising soft-tissue infections, particularly in hypoxic wounds where conventional therapies show limited efficacy.
An authoritative 2026 summary in Undersea and Hyperbaric Medicine (Huang et al., PubMed | Our Assessment) places the modern wound-healing case in its historical context: Dr TK Hunt’s National Science Foundation-commissioned work in 1964 established that wound healing is dependent on tissue oxygenation, the foundational rationale for every contemporary surgical-wound HBOT protocol.
How do I screen a patient before referral?
The hyperbaric facility will perform its own pre-treatment workup, but a competent surgical referral expedites the consultation and avoids wasted clinic visits. Run the following checklist before sending the patient.
- Confirm the indication. Use the table above and the UHMS Hyperbaric Oxygen Therapy Indications reference. For off-label use, document the rationale and the failure of first-line therapy in the chart.
- Document the surgical bed. Operative notes, the date of the index procedure, any prior radiation, vascular imaging, and a current wound photograph save the hyperbaric physician 20 minutes of catch-up.
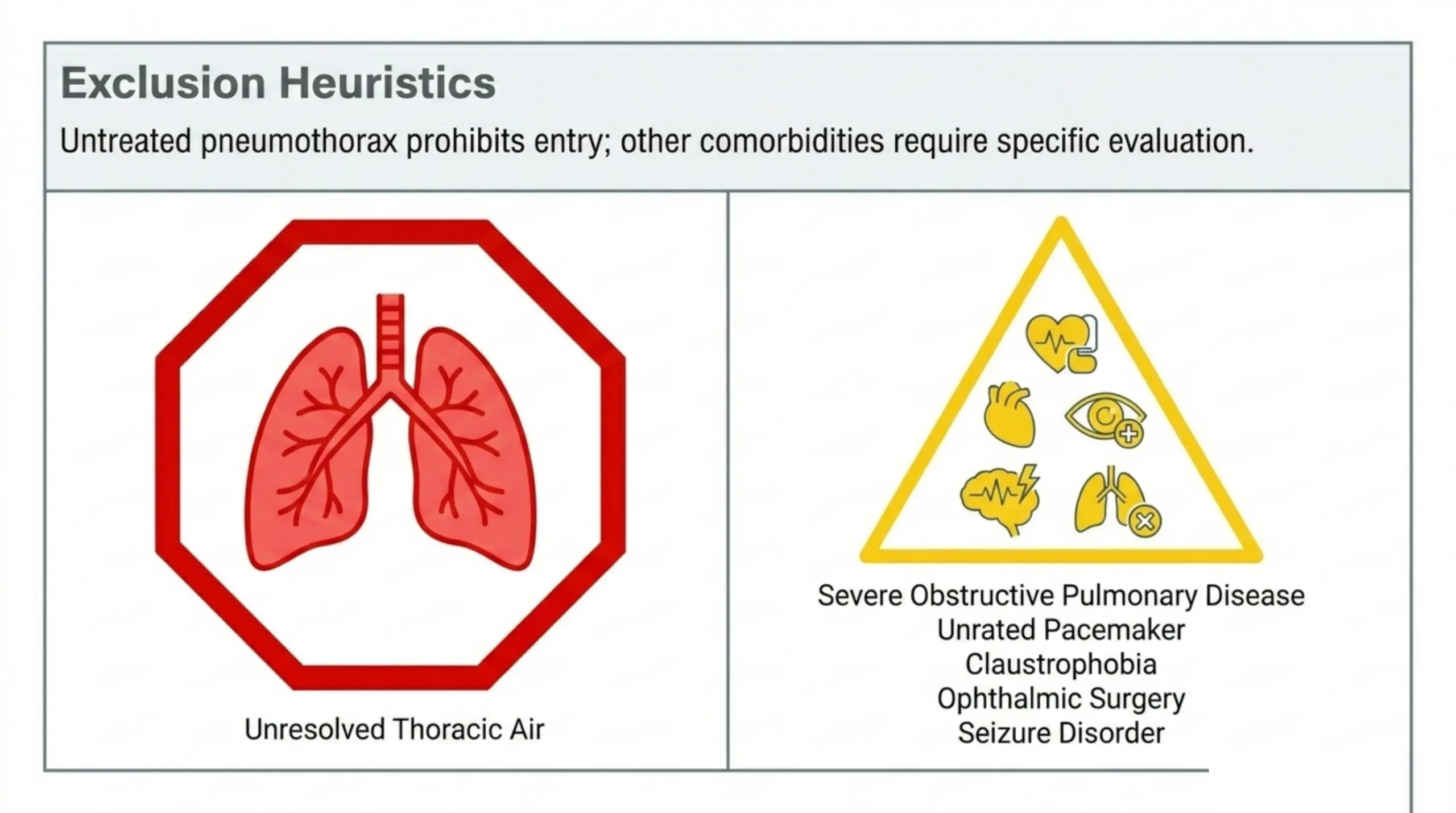
- Screen for absolute contraindications. Untreated pneumothorax is the only absolute contraindication. Confirm with a recent chest X-ray if the patient has been on positive-pressure ventilation, has chest trauma, or has had recent thoracic surgery.
- Screen for relative contraindications. Severe COPD with CO₂ retention, untreated middle-ear pathology, claustrophobia, recent ophthalmic surgery, pacemakers not rated for hyperbaric pressure, and uncontrolled seizure disorder all need to be flagged. None are automatic disqualifiers, but each changes the protocol.
- Review medications for HBOT-specific interactions. Bleomycin (any prior exposure) and concurrent disulfiram, doxorubicin, or cisplatin require discussion with the hyperbaric physician before treatment begins. Provide a complete medication list, including chemotherapy history.
- Document otoscopy and patency. A baseline otoscopic exam and a tympanogram (where available) lower the rate of middle-ear barotrauma. Patients with eustachian-tube dysfunction may need tympanostomy tubes before starting therapy.
- Check glycaemic control in diabetic patients. HBOT can lower blood glucose. Patients on insulin or sulphonylureas need a baseline glucose and a glucometer on hand for each session.
- Capture baseline imaging or measurements. For wounds, a digital image with a ruler. For grafts and flaps, the operative drawing. For osteomyelitis, the most recent MRI or bone scan. These let the hyperbaric team measure response objectively over the course of treatment.
What is the step-by-step referral process in Canada?
Canada has no single national referral pathway; access is organised at the facility level. The following workflow applies across provinces.
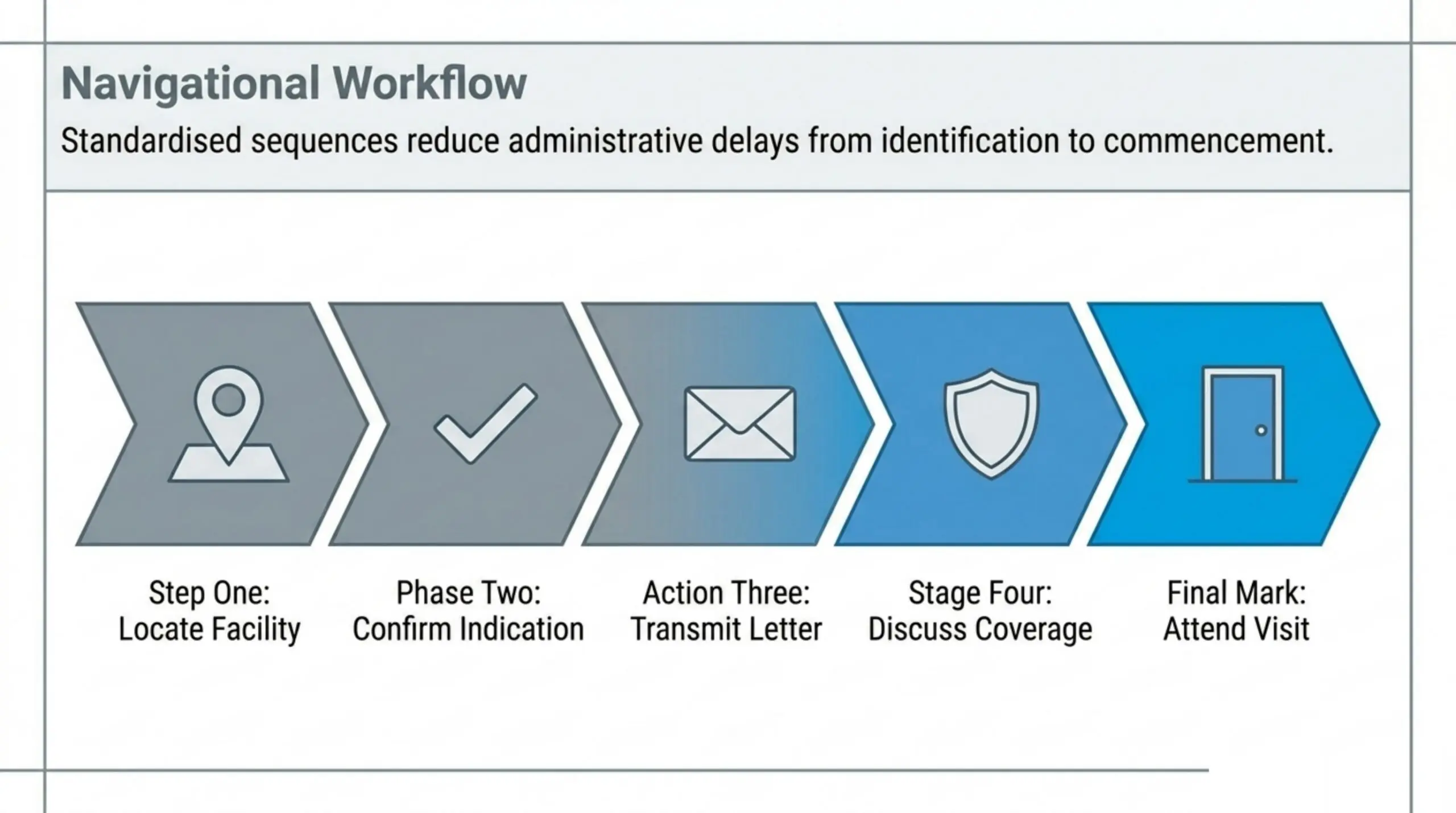
- Identify the closest regulated facility. Start with the Canada Hyperbarics directory of hospitals and regulated facilities. The directory lists every verified Canadian hyperbaric facility using Health Canada-licensed chamber equipment, with chamber type (monoplace or multiplace), patient population, and contact details.
- Confirm the facility accepts your indication. Hospital-based programmes typically treat the Health Canada and UHMS-recognised indications. Some private facilities take a broader scope. Phone or email the facility’s hyperbaric coordinator before sending the chart.
- Send a structured referral letter. Include diagnosis, ICD-10 code, surgical history, current medications, the screening items above, and your contact details. Most facilities have a referral form on their site; using it shortens the intake by a week.
- Discuss coverage with the patient. Provincial public-insurance coverage for HBOT varies. Hospital-based programmes treating a recognised indication are typically covered through the provincial health plan. Private-clinic care is generally self-pay. Direct the patient to the Canada Hyperbarics coverage guide for current province-specific details.
- Expect a hyperbaric medicine consultation. The hyperbaric physician will repeat the screening, set the treatment pressure (most surgical-wound protocols run at 2.0 to 2.4 ATA for 90 minutes), and quote a typical course length of 20 to 40 sessions delivered five days a week.
- Plan for transportation and lodging. For rural and remote patients, this is often the binding constraint. Some hospital programmes will block-schedule out-of-town patients to consolidate travel.
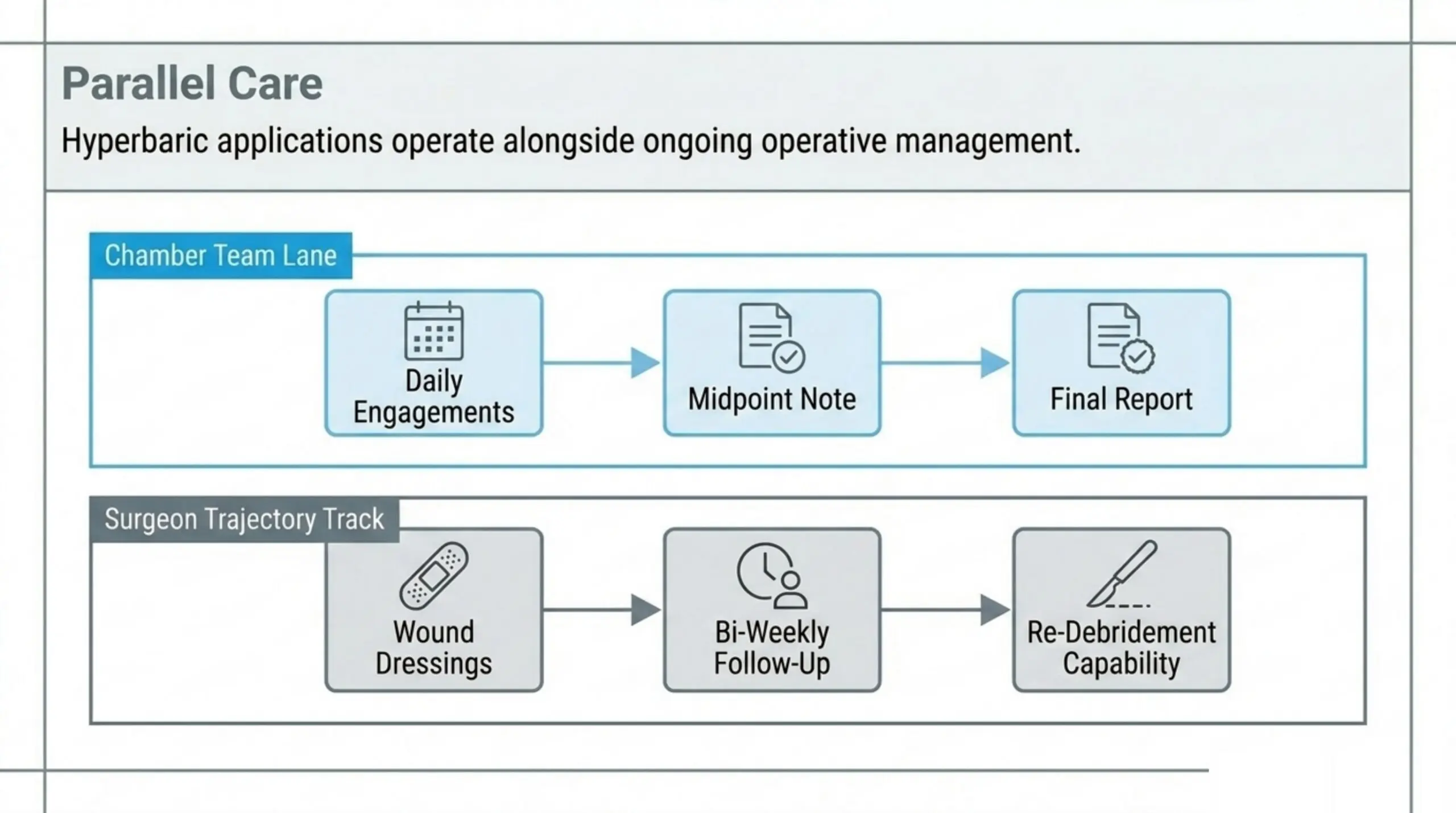
- Hand off, but stay involved. The hyperbaric team will manage day-to-day treatment, but the surgical team remains responsible for wound care, dressings, and any operative re-intervention.
How do I co-manage the patient during HBOT?
Surgical co-management during a hyperbaric course is straightforward when expectations are set early.
- Wound care continues unchanged unless the hyperbaric team identifies a problem (excessive maceration, dressing intolerance, secondary infection). Dressings come off before each chamber session and go back on after.
- Schedule clinic follow-up at the same intervals you would otherwise. Two weeks, four weeks, and at the end of the hyperbaric course is a reasonable baseline; tighten for grafts and flaps.
- Expect a written progress note from the facility at the midpoint (typically session 10 or 20) and at completion. If you have not received one, request it; this documentation matters for insurance and for the chart.
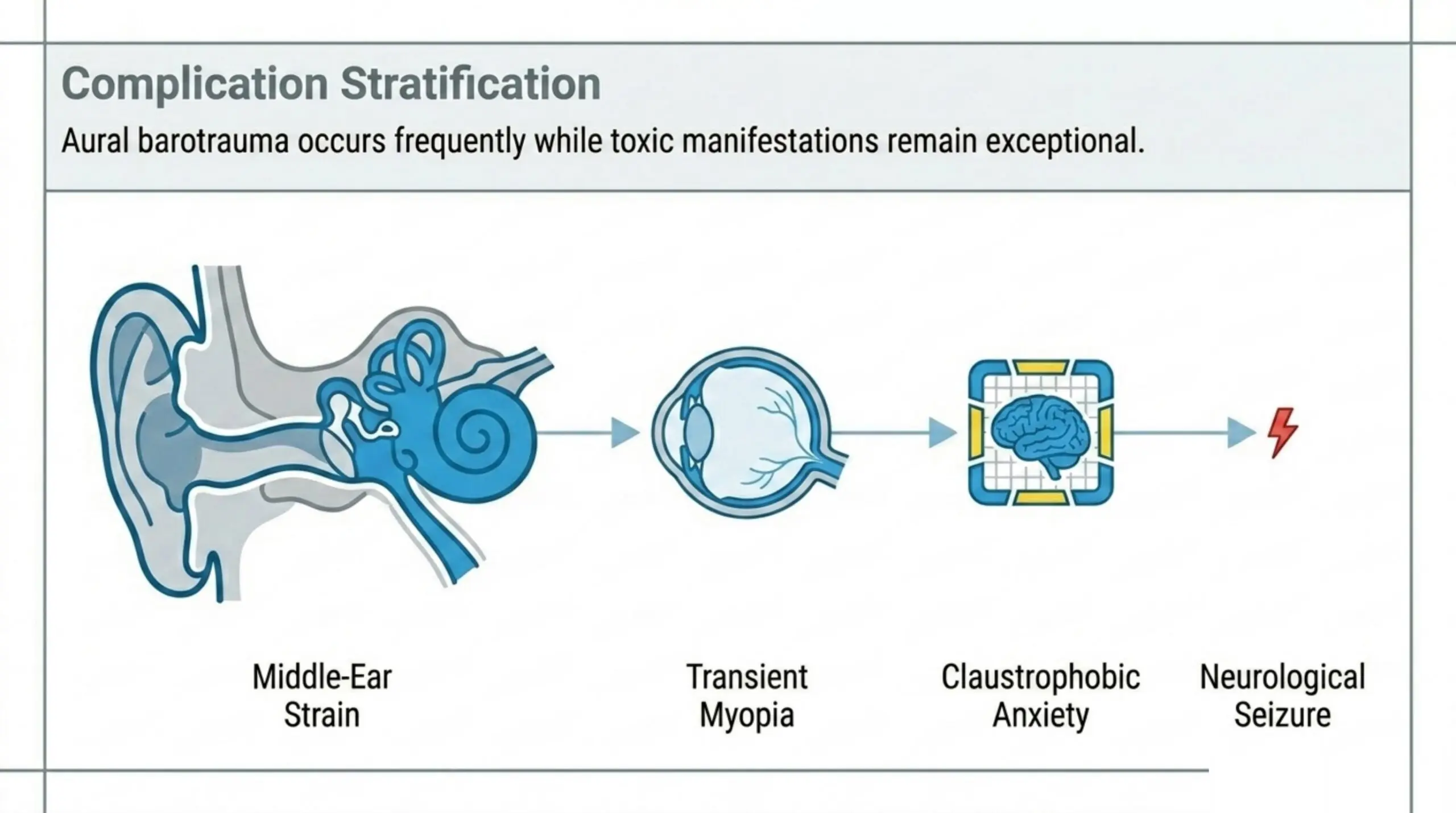
- Common side effects to recognise: middle-ear barotrauma (most common, usually mild), transient myopia (reported in roughly one in five patients on long courses; resolves within a few weeks of completion), claustrophobia and anxiety (manageable with pre-session technique or low-dose anxiolysis), and oxygen-toxicity seizure (uncommon at standard surgical pressures).
- When to interrupt treatment: any new pneumothorax, an unmanaged seizure, a new pregnancy, or a clinically significant worsening of the wound that suggests an alternative diagnosis (deeper infection, malignancy, vascular compromise needing revascularisation).
For a deeper walk-through of HBOT contraindications and side effects from the referring physician’s perspective, see our companion guides on approved conditions and the research bank.
What does HBOT cost and how do patients access it?
Hospital-based hyperbaric programmes that treat a recognised indication are typically funded through the provincial health plan; the patient pays nothing out of pocket beyond the standard parking and transport costs. Private-clinic care is usually self-pay, with per-session fees varying by region. Patients with extended-health benefits should check whether their plan reimburses HBOT for the specific indication on the referral letter; some do, most do not. For the most current province-by-province breakdown, refer patients to our coverage guide.
Frequently asked questions from referring surgeons
How urgent is a flap-compromise referral?
Within 24 to 72 hours of recognising compromise is the operational window cited in the contemporary plastic-surgery literature. Earlier initiation correlates with better outcomes in the 2026 Najib retrospective and is consistent with the strong recommendation for HBOT in flap and graft salvage from the 2026 Carter systematic review. Call the facility’s hyperbaric coordinator the same day you recognise the compromise.
Do I need a hyperbaric medicine consultant on staff to refer?
No. Any licensed Canadian physician can refer a patient. The receiving facility provides the hyperbaric medicine consultation and assumes responsibility for the HBOT-specific aspects of care.
Will HBOT delay reconstruction or re-operation if needed?
No. HBOT runs in parallel with surgical care. If you decide the patient needs re-debridement, a return to theatre, or a revision flap, the hyperbaric team will pause the course for the operative day and resume the next day. There is no washout period.
Is HBOT covered for off-label surgical indications?
Coverage tracks the Health Canada and UHMS-recognised indications, which overlap substantially. Off-label use (for example, ACL graft maturation or routine elective rhinoplasty) is generally self-pay through a private facility. The 2026 evidence base is expanding for several of these uses, but reimbursement decisions in Canada lag the evidence.
What pressure and session length should I expect for surgical-wound protocols?
Most surgical-wound protocols deliver 90 minutes of 100% oxygen at 2.0 to 2.4 ATA, five days a week, for 20 to 40 sessions. The hyperbaric physician adjusts the protocol based on the indication, the wound trajectory, and patient tolerance. The Carter 2026 systematic review of flap and graft indications used 2.0 to 2.5 ATA for its meta-analytic estimates.
Can I send a patient with a pacemaker, an implanted port, or an insulin pump?
Each device has its own pressure rating. The hyperbaric facility will check the manufacturer’s specification against its chamber pressure. Many modern pacemakers, ports, and insulin pumps are pressure-rated for standard hyperbaric protocols, but the answer is device-specific. Provide the device make and model on the referral.
How do I find the closest Canadian facility?
Use the Canada Hyperbarics facility directory. We list every Canadian hospital programme and private clinic operating Health Canada-licensed chamber equipment, with chamber type and patient population. We update the directory monthly and verify changes against Health Canada’s hyperbaric oxygen therapy page and the Canadian Undersea and Hyperbaric Medical Association (CUHMA).
Where can I read the underlying evidence?
The authoritative references for Canadian surgical-wound referrals are the UHMS Hyperbaric Oxygen Therapy Indications book, the UHMS Clinical Practice Guidelines, the Health Canada hyperbaric oxygen therapy page, and the CUHMA position statements. For Health Canada medical-device licensing of the chambers themselves, see the medical device licensing guidance.
Canada Hyperbarics maintains an indexed bank of more than 14,000 HBOT studies with structured summaries; the research bank is searchable by condition and study design.
Where do I send my next surgical-wound patient?
If you have a compromised flap or graft, a stalled surgical wound, or a tissue-salvage decision in front of you this week, start with the Canada Hyperbarics directory of hospitals and regulated facilities. Use the screening checklist above to prepare the referral letter, contact the facility’s hyperbaric coordinator, and the patient can usually be consulted within 7 to 14 days.
This content is for informational purposes only and does not constitute medical advice. Treatment decisions for any individual patient should be made in consultation with a qualified hyperbaric medicine physician and the patient’s full clinical team. Last reviewed: 2026-06-04.