
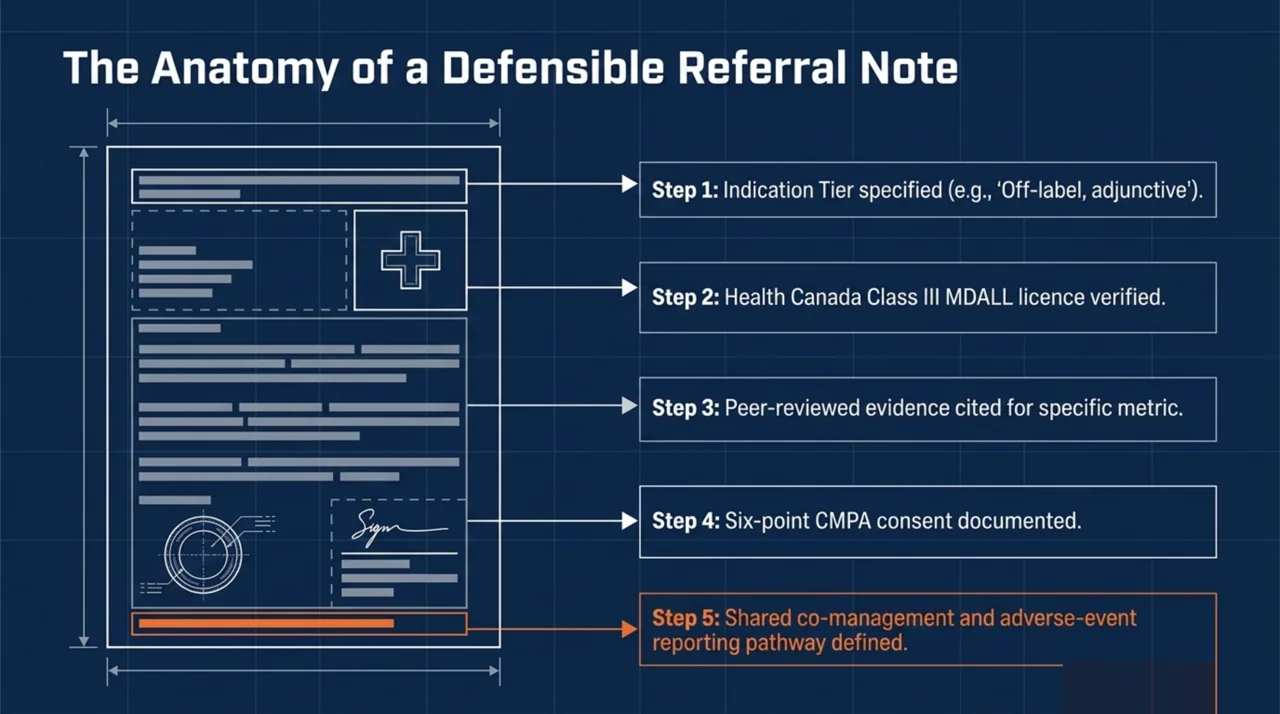
TL;DR: A defensible HBOT referral note documents five things: the indication, evidence supporting the referral, confirmation that the chamber is Health Canada-licensed, informed consent including risks and alternatives, and a co-management and follow-up plan. Canadian physicians who follow this five-step framework satisfy the documentation expectations of provincial colleges, the Canadian Medical Protective Association (CMPA), and Health Canada’s medical device incident-reporting framework.
Hyperbaric oxygen therapy (HBOT) referral documentation is the written record a Canadian physician creates when sending a patient for treatment in a Class III Health Canada-licensed hyperbaric chamber. The note explains why the patient needs HBOT, what evidence supports the referral, how the patient was screened, and how risks were disclosed. Done well, it protects the patient, the referring physician, and the treating facility. Done poorly, it leaves all three exposed when a complication occurs or when a regulator asks for justification.
This guide walks through the five-step documentation framework Canadian physicians should follow for every HBOT referral, whether the indication is recognised (such as carbon monoxide poisoning or compromised flaps) or off-label (such as central retinal artery occlusion or refractory ulcerative colitis). Canada Hyperbarics maintains a national directory of hospitals and regulated facilities to support practitioners who need to identify a referral pathway for any of these indications.
Why does HBOT referral documentation matter under Canadian law?
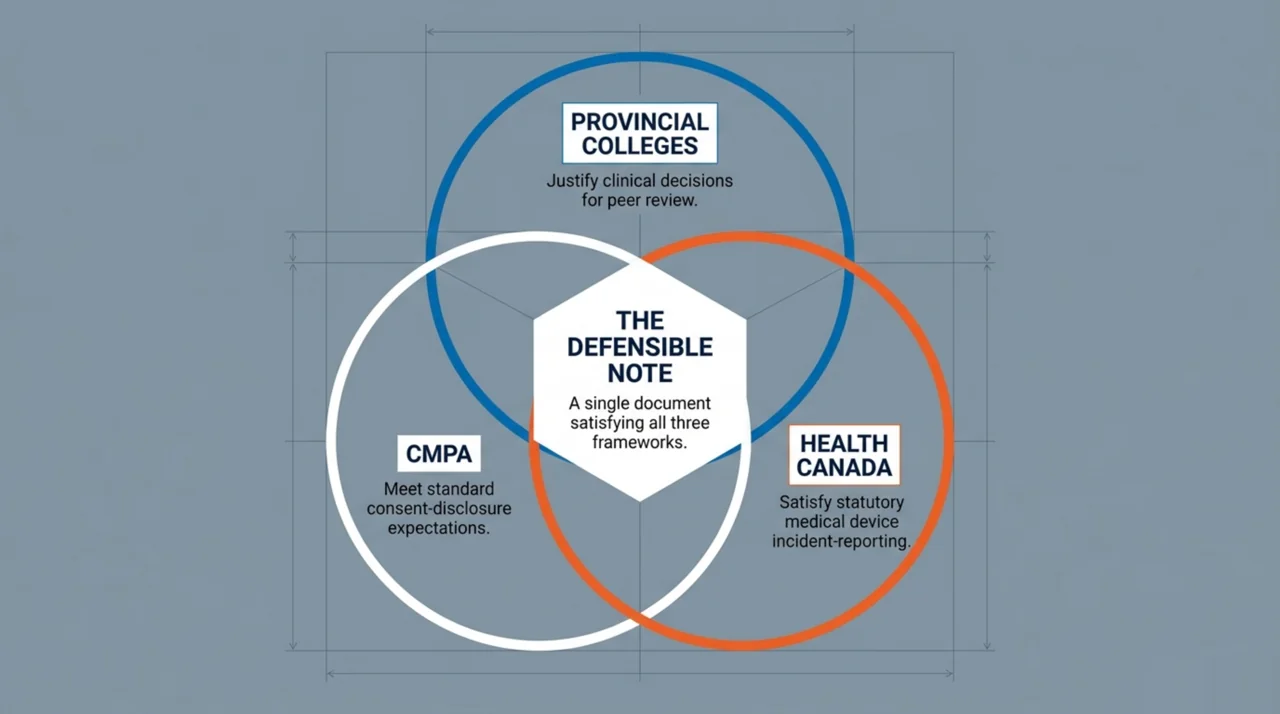
Three Canadian frameworks shape the documentation expectations for an HBOT referral. First, every provincial College of Physicians and Surgeons requires that medical records justify clinical decisions in a way a peer reviewer could follow. Second, the CMPA’s Consent: A Guide for Canadian Physicians sets out the consent-disclosure standard most provincial courts apply when patients later allege they were inadequately informed. Third, Health Canada’s Incident Reporting for Medical Devices Guidance creates a statutory reporting obligation for hospitals when serious incidents involving a licensed medical device, including a hyperbaric chamber, occur during treatment.
A referral note that ties the indication to current evidence, names the Health Canada licence number of the chamber, and records a clear consent discussion satisfies all three frameworks at once. The single biggest documentation gap Canadian physicians fall into is treating HBOT as a generic referral rather than as a referral to a regulated medical device with specific recognised indications. That gap is what the steps below close.
Step 1: Identify the indication and match it to the evidence base
The first line of the referral note states the clinical indication in language that aligns with Health Canada and the Undersea and Hyperbaric Medical Society (UHMS). For approved indications such as carbon monoxide poisoning, decompression sickness, compromised flaps and grafts, necrotising soft-tissue infection, and chronic refractory osteomyelitis, name the indication using the UHMS term. For investigational or off-label indications, name the condition and add a phrase such as “for adjunctive use, off-label, supported by current evidence.”
Real-world Canadian and international practice patterns inform what reasonable referral looks like. A 2026 multicentre prospective observational study of 327 patients across 10 Italian hyperbaric centres (Ippolito et al., PubMed | Our Assessment) reported that the three most common indications were sudden hearing loss (35.8%), carbon monoxide poisoning (19.9%), and soft-tissue infection (12.2%), with no serious adverse events recorded across the cohort. A Canadian referrer who is referring for any of those three indications can reasonably point to this distribution as part of the standard-of-practice rationale.
Tier the indication by evidence strength
| Indication tier | What the note should record |
|---|---|
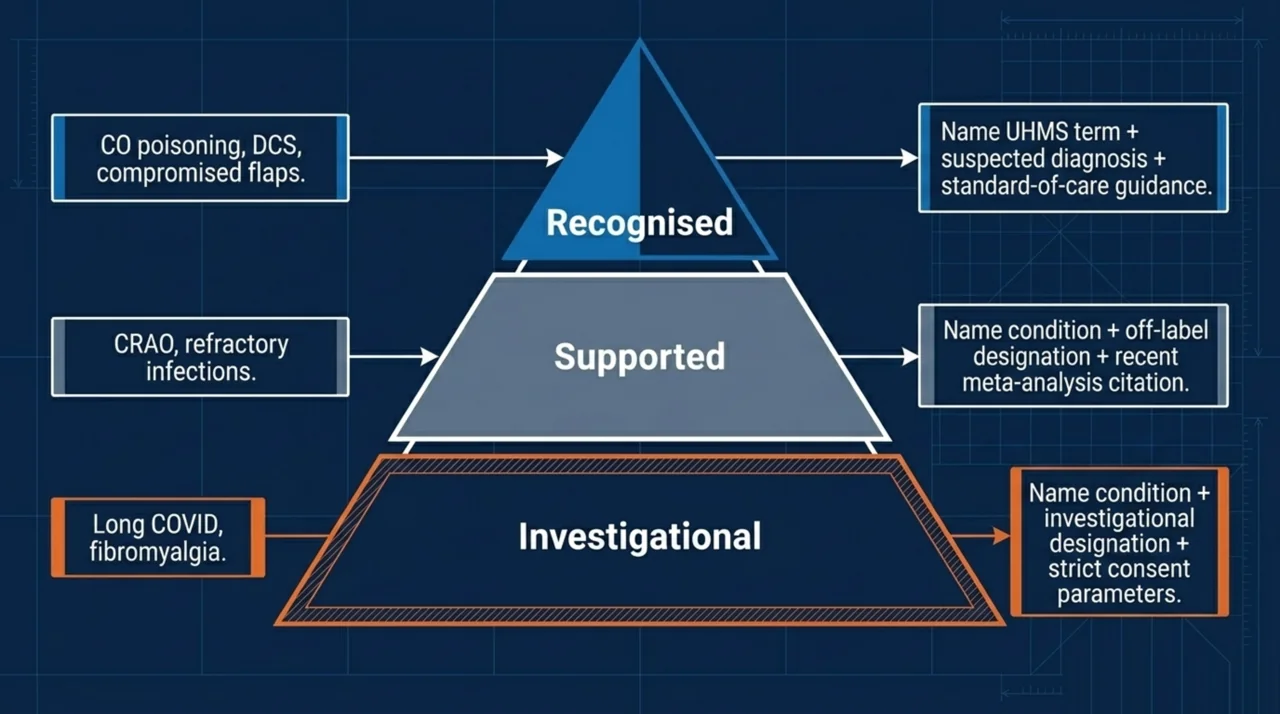
| UHMS-recognised, recognised (e.g., CO poisoning, DCS, flaps/grafts) | The UHMS indication name, the suspected diagnosis, and a brief reference to standard-of-care guidance. |
| Off-label but supported by recent systematic reviews (e.g., CRAO, refractory infections) | The condition, the off-label designation, and a citation to a recent meta-analysis or pooled review. |
| Investigational (e.g., long COVID, psychiatric indications, fibromyalgia) | The condition, the investigational designation, the limits of current evidence, and a stronger consent paragraph. |
Step 2: Verify the chamber is Health Canada-licensed
Hyperbaric chambers sold or used in Canadian medical practice are Class III medical devices and must hold an active Health Canada device licence. Before sending the referral, confirm the receiving facility’s chamber is listed on the Health Canada Medical Devices Active Licence Listing (MDALL) and record the licence number in the chart, or note that the facility provided it on request. This single line of documentation distinguishes a referral to a regulated medical device from a referral to an unregulated wellness device.
Soft-sided or “mild” portable chambers marketed for home use are not authorised for medical indications and should not appear in a referral note. Canada Hyperbarics maintains a national directory of hospitals and regulated facilities operating Health Canada-licensed chambers, organised by province, to make this verification fast.
Step 3: Cite the evidence supporting the referral
Defensible referral notes name at least one published source supporting the indication. For approved indications, a recent systematic review is sufficient; for off-label indications, citing recent evidence is part of meeting the consent disclosure standard, because the conversation with the patient should reflect what the literature actually shows.
For flap and graft referrals, a 2026 systematic review of comparative studies (Carter et al., PubMed | Our Assessment) analysed 25 reports from 24 studies including 13 RCTs and 2,246 patients. A pooled meta-analysis of four RCTs at 2 to 2.5 ATA found a large favourable effect on flap and graft survival within four weeks of HBOT, and the authors issued a strong recommendation for HBOT to heal flaps or grafts in soft-tissue injury and trauma wounds. For a Canadian plastic-surgery or reconstructive referral, this is the citation to put in the note.
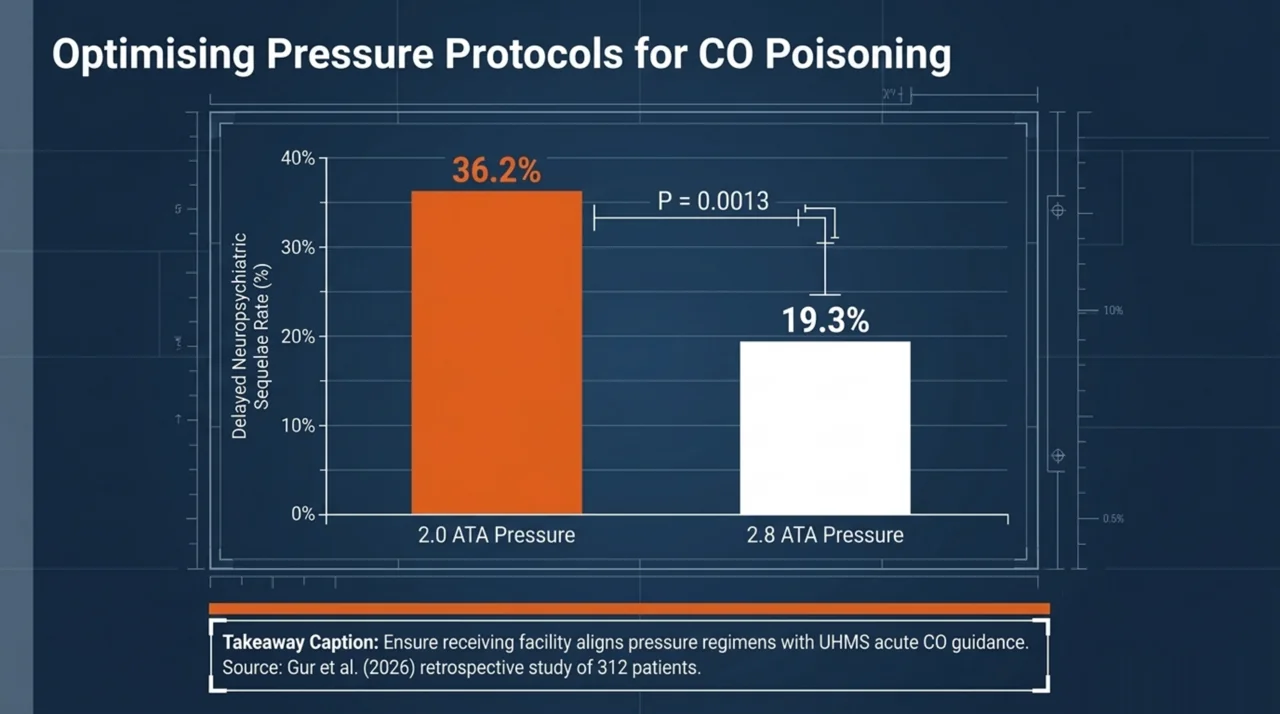
For carbon monoxide poisoning, dose selection is part of the referral conversation. A 2026 retrospective study of 312 patients across four HBOT regimens (Gur et al., PubMed | Our Assessment) reported that patients treated at lower pressures (2.0 ATA) were associated with a higher delayed neuropsychiatric sequelae rate (36.2%) than those treated at higher pressures (2.8 ATA, 19.3%), with the difference reaching statistical significance (P = 0.0013). The note should specify that the receiving facility uses an evidence-aligned pressure regimen for acute CO poisoning, consistent with current UHMS guidance.
For central retinal artery occlusion (CRAO), referral timing is the central documentation point. A 2026 systematic review and meta-analysis of 12 studies (ALBalawi et al., PubMed | Our Assessment) reported a pooled odds ratio of 0.47 (95% CI 0.26 to 0.87, P = 0.02) favouring HBOT, with greater visual improvement consistently reported when HBOT was initiated within 12 hours of symptom onset. Heterogeneity was substantial. The referral note should record the time-of-symptom-onset clock and flag the case as time-critical for the receiving facility.
For complex infections, a 2026 mechanism review (Zhang et al., PubMed | Our Assessment) summarised the case for adjunctive HBOT in diabetic foot wounds, necrotising soft-tissue infections, COVID-19, and mucormycosis, while noting that further randomised trials are needed to standardise protocols. For these referrals, the documented framing is adjunctive use alongside standard antimicrobial and surgical care, not as a replacement for it.
For investigational indications, the evidence-citation requirement is stricter, not weaker. A 2026 Phase I/II feasibility and safety trial in infective endocarditis (Pries-Heje et al., PubMed | Our Assessment) enrolled 13 selected patients with left-sided endocarditis caused by Gram-positive cocci. Of the 10 who completed the protocol, no serious adverse events or suspected unexpected serious adverse reactions were recorded. A referral note for an investigational indication should explicitly cite this kind of feasibility evidence rather than gesturing at HBOT’s general safety record.
For a broader synthesis across indications, the Canada Hyperbarics research database indexes published studies on hyperbaric medicine relevant to Canadian referrers, and the conditions index summarises the current evidence for each indication.
Step 4: Document informed consent in the standard CMPA format
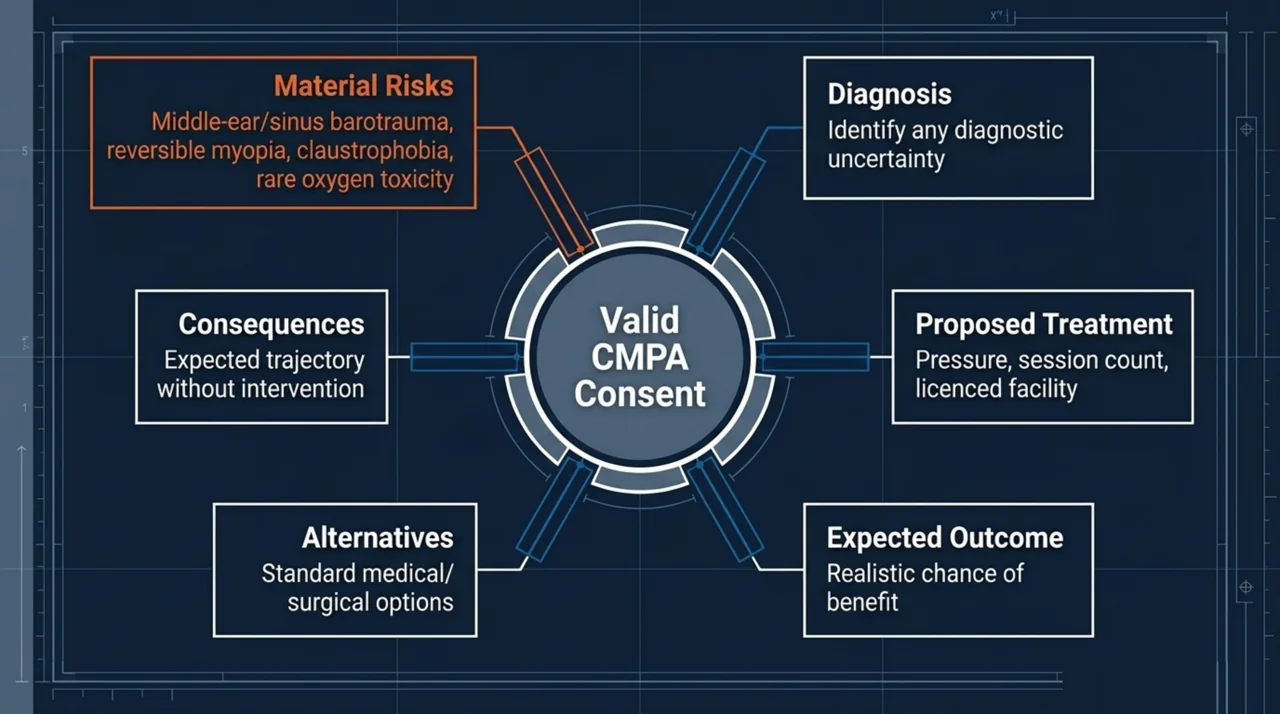
The CMPA consent standard expects the physician to disclose, and the chart to reflect: the diagnosis (with any uncertainty), the proposed treatment, the chances of success, the material and special risks, the alternative treatments and their risks, and the consequences of not treating. For HBOT, this means the referral note records each of those six elements in plain language, not just a generic “consent obtained” line.
- Diagnosis: name the working diagnosis and any diagnostic uncertainty.
- Proposed treatment: HBOT at a specified pressure and session count, delivered in a Health Canada-licensed chamber at a named facility.
- Expected outcome: the realistic chance of benefit, framed against the published evidence for the indication.
- Material risks: middle-ear barotrauma (the most common adverse event, generally minor and manageable), sinus barotrauma, reversible myopia with prolonged courses, claustrophobia in monoplace chambers, and the rare risk of pulmonary or central nervous system oxygen toxicity.
- Alternatives: standard medical or surgical management without HBOT, or a delayed referral pending response to first-line therapy.
- Consequences of not treating with HBOT: the expected course of the underlying condition without the adjunctive therapy.
For investigational or off-label indications, the consent paragraph should expressly use the word “investigational” or “off-label” and record that the patient understood the indication is not on the recognised list. This single sentence is the most important medical-legal protection in the entire note.
Step 5: Plan and document follow-up and adverse event communication
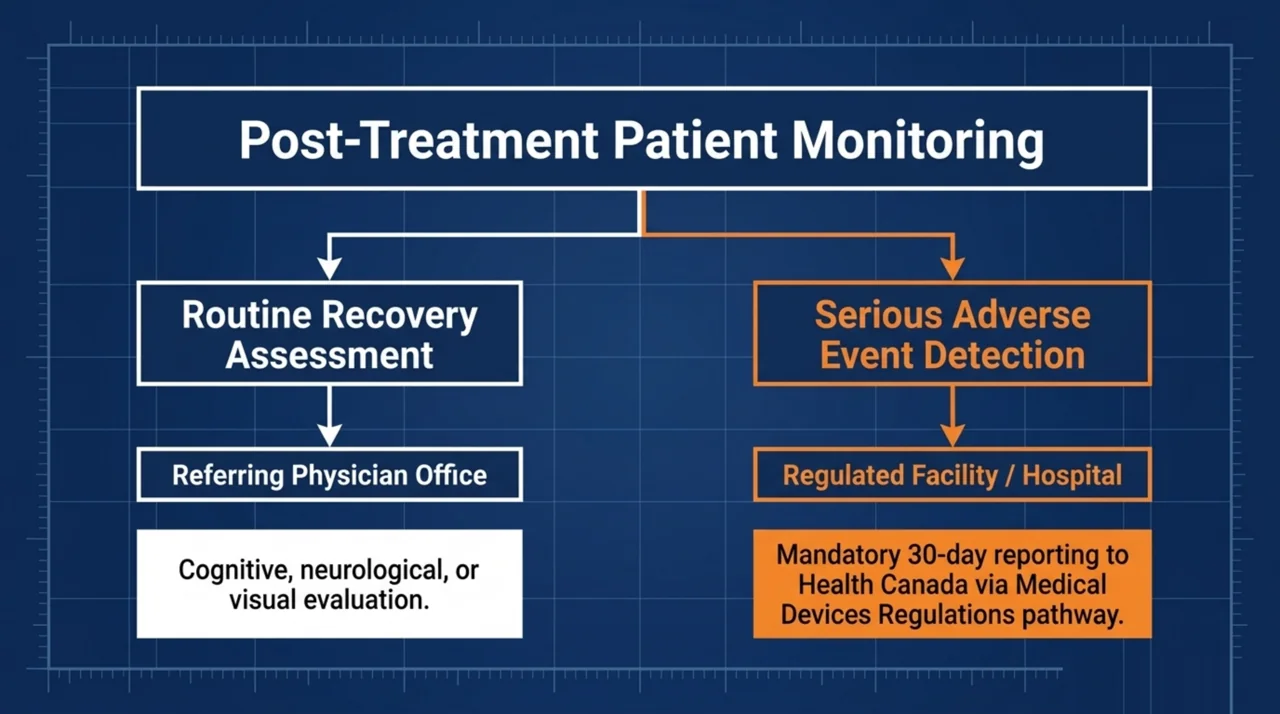
The final step ties the referring physician back into the treatment loop. The note should specify who is following the patient during the HBOT course (typically a shared model with the treating hyperbaric physician), what symptoms would prompt the patient to call the referring office versus the facility, and the expected timing of a treatment-completion summary. For acute indications such as CO poisoning, DCS, and CRAO, the follow-up plan also names the recovery-window assessments (cognitive, neurological, or visual) the referrer will perform after the course.
The note should also reference the adverse event reporting pathway. Under the Medical Devices Regulations, Canadian hospitals are required to report serious medical device incidents to Health Canada within 30 days, using the Health Canada medical device problem reporting pathway for health care providers. Outside the hospital setting, voluntary reporting is encouraged. The referral note does not need to reproduce the reporting form, but it should state that the patient was informed serious adverse events will be reported through this pathway.
Frequently asked questions
Do I need to document Health Canada licensure on every referral?
For first-time referrals to a facility, yes, record the chamber’s MDALL listing or the licence number. For repeat referrals to a facility you regularly use, a chart note recording that the facility was previously verified is sufficient, but a periodic re-check at least annually is good practice.
How specific does the consent risk disclosure need to be?
Specific enough that the patient could repeat the major risks back in their own words. The CMPA standard is what a reasonable patient in similar circumstances would want to know, not a comprehensive list of every theoretical risk. For investigational indications, the bar is higher, and the note should record both the uncertainty about benefit and the absence of Health Canada recognition.
Who is responsible for adverse event reporting, the referring physician or the facility?
The hospital or facility operating the chamber holds the mandatory reporting obligation under the Medical Devices Regulations. The referring physician’s role is to communicate any post-treatment adverse symptoms back to the facility promptly and to document that the patient was informed of the reporting pathway. A practitioner-side voluntary report is also welcomed by Health Canada.
Can I refer for an off-label indication and still be medically defensible?
Yes, off-label referral is a normal part of Canadian practice, provided the documentation explicitly identifies the indication as off-label, cites recent evidence supporting the referral, records an enhanced informed consent discussion, and confirms the patient has tried or considered standard-of-care first-line options. Off-label is a documentation problem, not a prohibition.
How many sessions should I specify in the referral?
Specify a session range rather than a fixed number. The treating hyperbaric physician will set the final protocol based on response, but a referral that frames an expected range (for example, “20 to 40 sessions, pending response”) is more useful than one that names a single number. Real-world Italian data report a median of 16 sessions per patient across all indications.
What if the patient asks whether HBOT is covered by their provincial health plan?
Coverage varies by province and indication. In Ontario, OHIP covers HBOT for specified indications when delivered in a designated hospital programme. Quebec’s RAMQ, British Columbia’s MSP, and Alberta Health Care all cover hospital-based HBOT for emergency indications such as DCS and CO poisoning. Off-label indications are routinely out-of-pocket. Direct the patient to the Canada Hyperbarics coverage guide for province-specific details rather than estimating in the referral note.
Does telehealth referral satisfy the consent documentation standard?
Yes, provided the consent discussion happened by direct two-way communication, the chart records the substance of the discussion in the same six-element format above, and the patient was given an opportunity to ask questions. The CMPA’s general guidance on virtual care consent applies.
Putting it together
A defensible Canada Hyperbarics-aligned HBOT referral note runs about half a page and contains: the indication and its tier (approved, off-label, or investigational), the chamber’s Health Canada licence status, at least one supporting citation, a six-element consent paragraph, and a follow-up plan that names who follows the patient and how adverse events will flow back to both the facility and the referrer. Practitioners who build this template once and reuse it for every referral satisfy the provincial college, CMPA, and Health Canada frameworks in a single note.
To identify a Health Canada-licensed receiving facility for a referral, search the Canada Hyperbarics directory of hospitals and regulated facilities. For evidence summaries by condition, the conditions index and the research database are updated as new Canadian and international literature is indexed.
This content is for informational purposes only and does not constitute medical advice, legal advice, or regulatory advice. Canadian physicians should consult their provincial college, the CMPA, and Health Canada directly for current binding guidance, and should verify Health Canada device licence status through MDALL at the time of each referral.