TL;DR: Hyperbaric oxygen therapy (HBOT) is well tolerated by most patients, and the only absolute contraindication is an untreated pneumothorax. Before referring a patient, the main safety questions are oxygen toxicity and seizure risk, the state of the lungs and middle ear, and a short review of current medications. Seizure disorders, significant lung disease, recent ear or chest surgery, uncontrolled fever and a few specific drugs are relative contraindications that call for screening and a conversation with the hyperbaric unit, not an automatic refusal. This guide summarises what Canadian referring physicians should check first.
Hyperbaric oxygen therapy is one of the safest interventions in medicine when patients are screened properly, but it is not appropriate for everyone. For a referring physician, the practical task is to identify the small number of patients who need extra assessment, dose adjustment or an alternative plan before they ever reach the chamber. The two issues that matter most are the risk of an oxygen toxicity seizure and the risk of pressure-related lung or ear injury (barotrauma). A short medication review rounds out the picture.
Central nervous system oxygen toxicity (CNS-OT) is a reaction to breathing oxygen at high partial pressure that can cause a generalised seizure with little or no warning. It is the single most important safety concept behind HBOT screening, because almost every relative contraindication either raises the chance of a seizure or makes a pressure injury more likely. This article walks through how to think about each one and how the recent evidence, including Canadian data, should shape your referral.
When is hyperbaric oxygen therapy not safe?
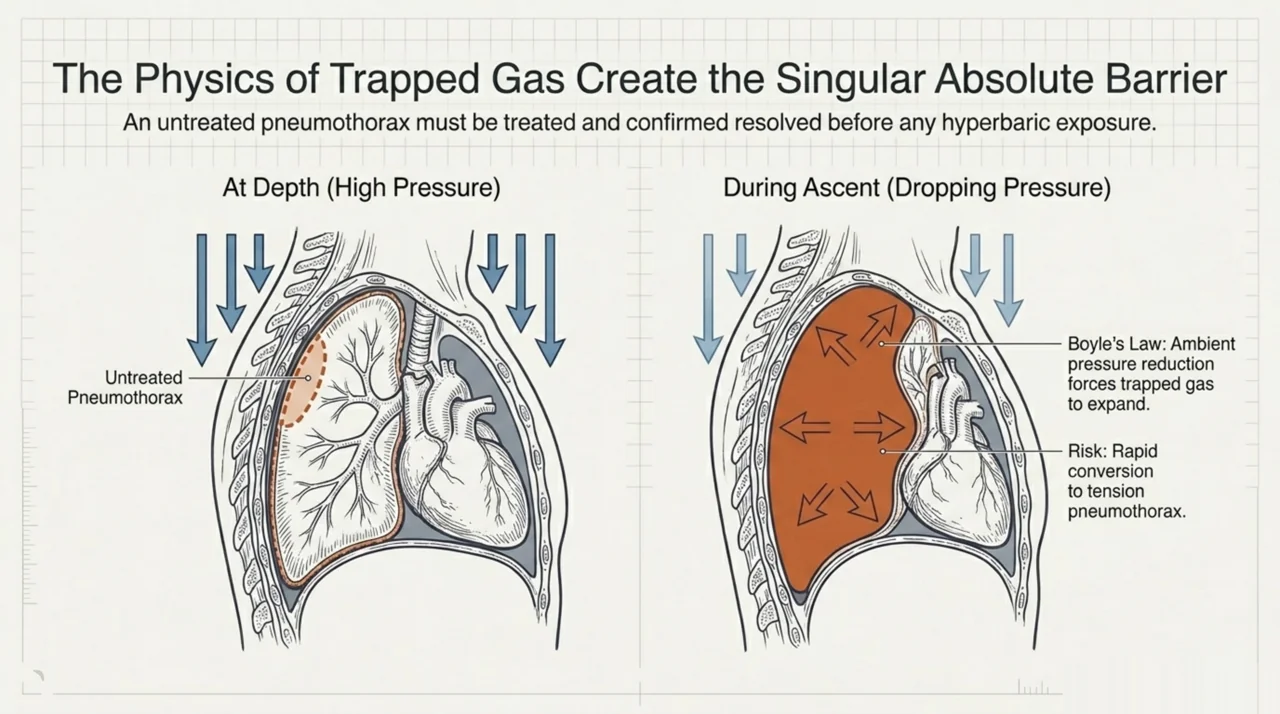
The only widely accepted absolute contraindication to HBOT is an untreated pneumothorax. Raising and then lowering ambient pressure changes the volume of any trapped gas, so an undrained pneumothorax can expand on ascent and become a tension pneumothorax. Everything else on the safety list is a relative contraindication: a reason to assess, optimise and discuss with the hyperbaric team, not a reason to withhold a potentially important treatment.
This distinction matters for referrals. A patient with epilepsy, chronic lung disease or a complex medication list is often still a good candidate once the hyperbaric physician has reviewed the case, adjusted the treatment pressure or built in extra air breaks. The Undersea and Hyperbaric Medical Society maintains the reference framework most Canadian units follow for indications and safety; you can review its current resources on the UHMS hyperbaric oxygen indications page. In Canada, the Canadian Undersea and Hyperbaric Medical Association (CUHMA) is the national professional body for the field.
What is oxygen toxicity and why does it matter for referral?
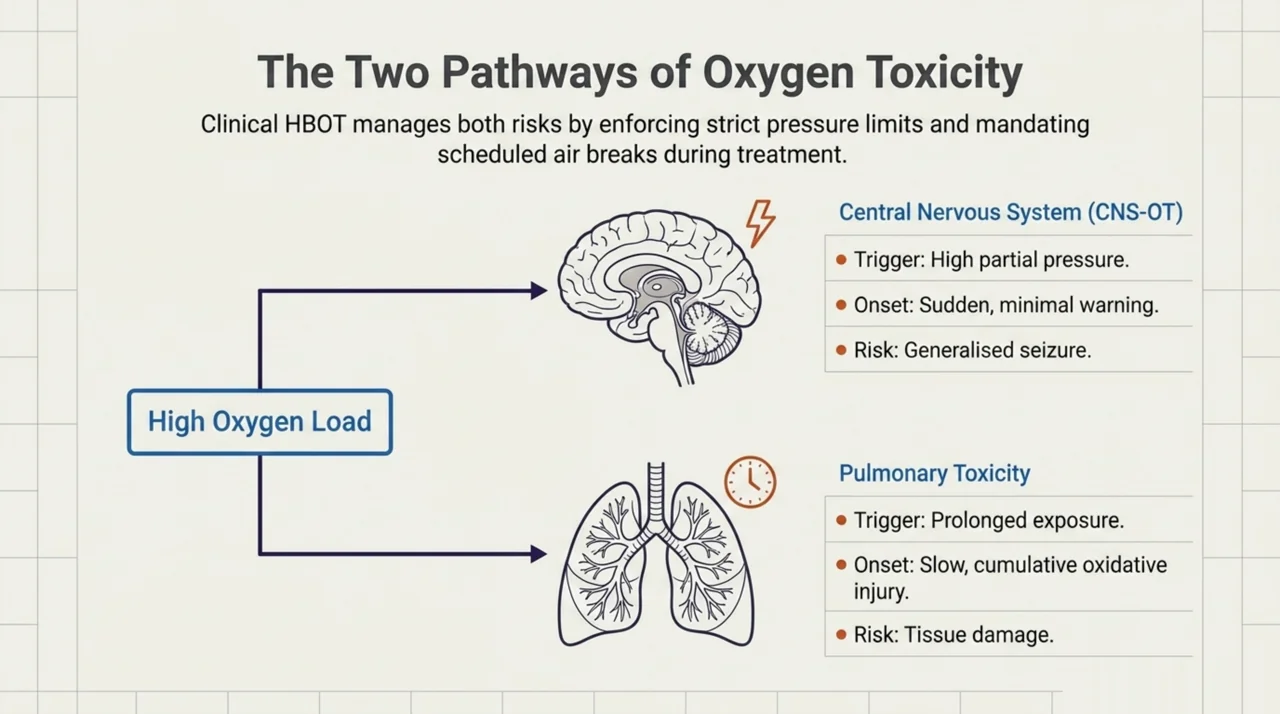
Oxygen toxicity comes in two forms. CNS oxygen toxicity affects the brain and can trigger a seizure during treatment. Pulmonary oxygen toxicity develops more slowly and reflects oxidative injury to lung tissue over prolonged exposures. Clinical HBOT manages both by keeping treatment pressures and durations within established limits and by using scheduled air breaks, during which the patient breathes ordinary air to give the body a brief recovery from the high oxygen load.
The underlying mechanism is oxidative stress at the level of the mitochondria. In a 2026 preclinical study, high-pressure oxygen exposure in animal and cell models disrupted mitochondrial function and activated pro-apoptotic signalling, and pharmacologically pre-activating mitophagy (the clearance of damaged mitochondria) prolonged the time to seizure in rats (Ding et al., 2026, PubMed | Our Assessment). The experimental exposure used in that work was far above the pressures used in patient care, so it explains the biology rather than describing a clinical protocol. Laboratory work on lung cells points the same way: a 2025 in vitro study found that hyperoxia, whether normobaric over days or hyperbaric over hours, produced mitochondrial dysfunction in human pulmonary cells, and tested whether compounds such as caffeine and a mitochondria-targeted antioxidant could blunt that effect, with differential results (Hossain et al., 2025, PubMed | Our Assessment).
For day-to-day referral the takeaway is simple. Oxygen toxicity is dose related, the hyperbaric unit controls the dose, and your job is to flag the patients in whom the seizure threshold may already be lowered. You can read more in the Canada Hyperbarics research library, which collects the studies our summaries are drawn from.
Which patients are at higher risk of an oxygen toxicity seizure?
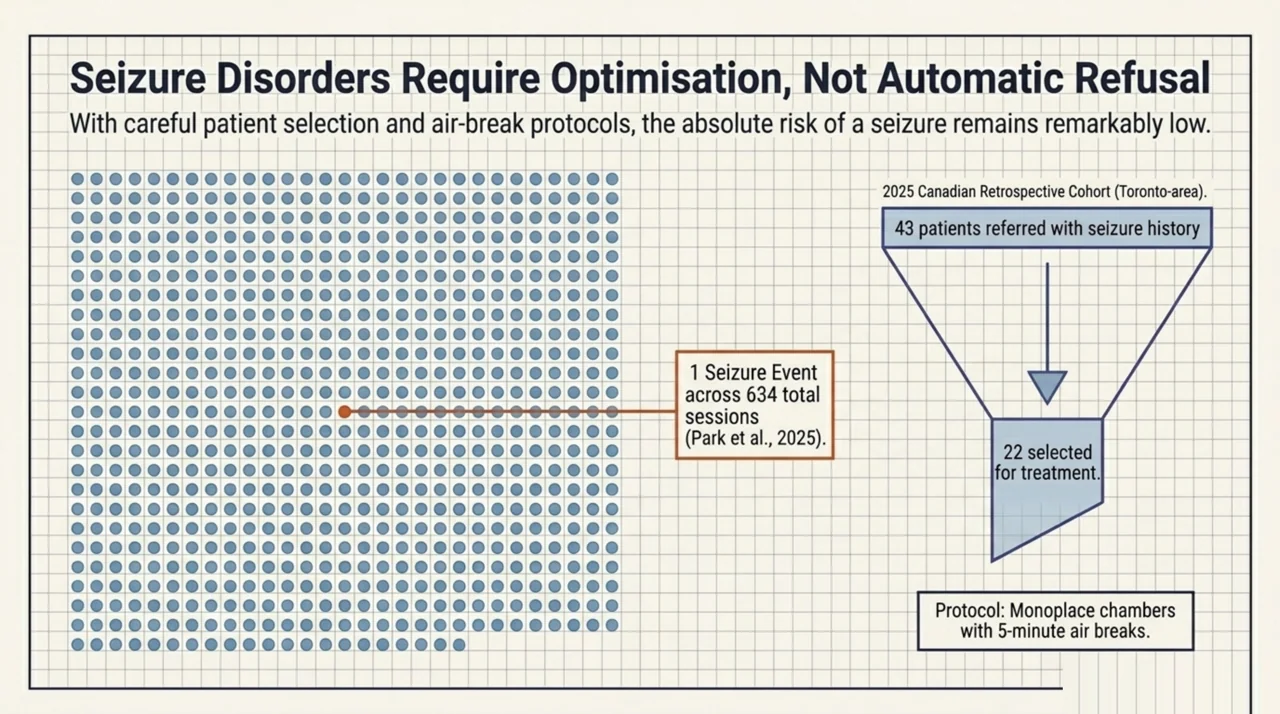
A seizure disorder is the classic relative contraindication, but the absolute risk during properly run HBOT appears low. A 2025 Canadian retrospective cohort from two Toronto-area hyperbaric units reviewed patients with a history of seizures who were referred for non-emergency HBOT. Of 43 patients referred, 21 did not proceed; the remaining 22 patients received 634 sessions in monoplace chambers with five-minute air breaks, and one patient experienced a seizure event during treatment (Park et al., 2025, PubMed | Our Assessment). Because this was an observational study with a small sample, the result is best read as reassuring rather than definitive: it was associated with a low seizure rate in carefully selected patients, and seizure disorders remain a relative contraindication that the hyperbaric physician should weigh case by case.
The broader safety framework still rests on respecting oxygen exposure limits. A 2025 expert revision of central nervous system oxygen toxicity exposure limits, written for the diving and technical-diving context where an inspired oxygen partial pressure of 1.3 atmospheres is common, reaffirmed that the principal preventive strategy is adherence to time limits tied to inspired oxygen pressure, and that CNS oxygen toxicity can present as a seizure with little or no warning (Hoyt et al., 2025, PubMed | Our Assessment). Clinical HBOT uses higher pressures than that diving scenario, which is exactly why patient-side risk factors matter. There is also no validated way to predict a seizure in real time: a 2025 systematic review of 16 studies examining electroencephalographic changes during hyperoxia found small, heterogeneous datasets and concluded the evidence is not yet sufficient to use EEG as a reliable early-warning tool (Barnes et al., 2025, PubMed | Our Assessment).
When you refer, note any factor that could lower the seizure threshold so the unit can adjust the protocol. The most relevant are:
- An established seizure disorder or a recent unprovoked seizure
- Uncontrolled high fever, which lowers the seizure threshold
- Significant carbon dioxide retention (for example, advanced COPD)
- Medications that lower the seizure threshold, and abrupt withdrawal of alcohol or benzodiazepines
- Low blood sugar at the time of treatment in patients on insulin or sulfonylureas
How should referring physicians screen the lungs and airway before HBOT?
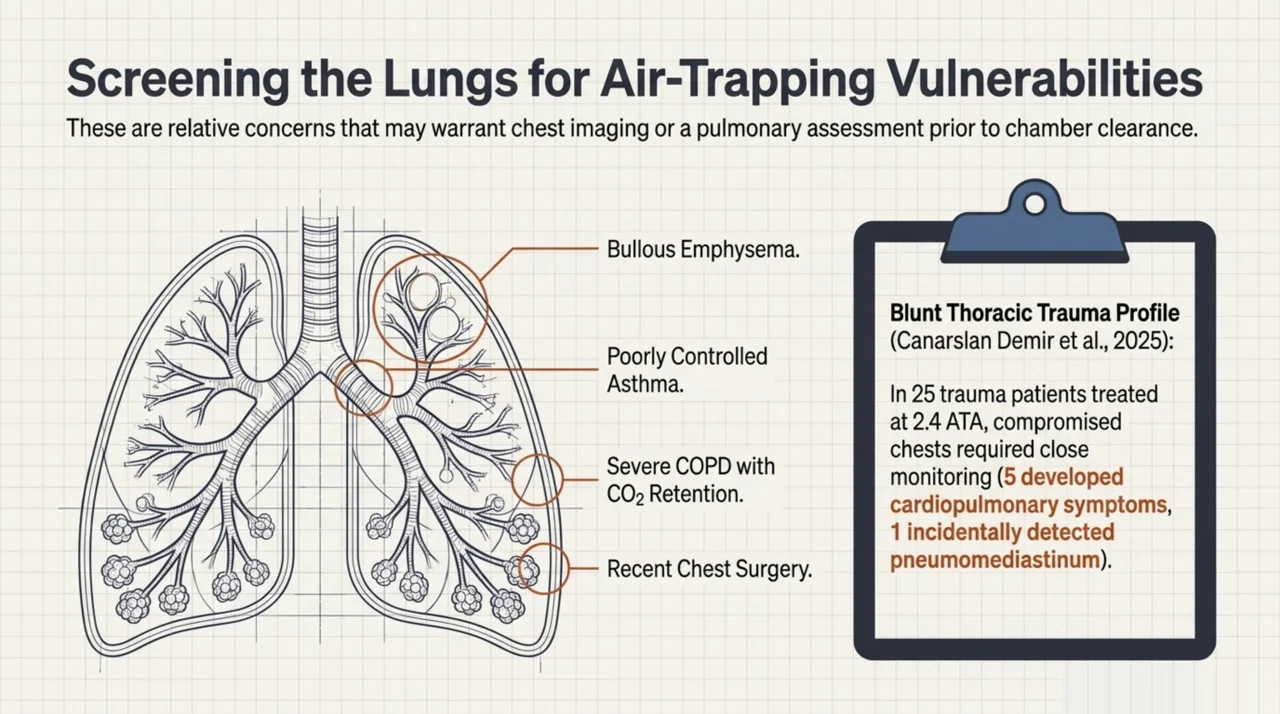
Because HBOT involves a pressure change, the lungs and middle ear are the structures most exposed to barotrauma. The lung concern is air trapping: an untreated pneumothorax is absolute, while bullous emphysema, poorly controlled asthma, recent chest surgery and severe COPD with carbon dioxide retention are relative concerns that may warrant imaging or pulmonary assessment first. A 2025 retrospective cohort of 25 patients with blunt thoracic trauma treated with HBOT at 2.4 atmospheres absolute reported that five patients (20%) developed respiratory or cardiac symptoms during treatment, one had an incidentally detected pneumomediastinum managed conservatively, and one experienced a generalised seizure attributed to CNS oxygen toxicity; three deaths during follow-up were due to severe crush injuries and were unrelated to HBOT (Canarslan Demir et al., 2025, PubMed | Our Assessment). As an observational series this does not prove cause and effect, but it is a useful reminder that patients with compromised chests need closer monitoring.
The middle ear is the more common, and more manageable, problem. Patients who cannot equalise pressure, have an active upper respiratory infection, or have had recent ear or sinus surgery are prone to middle ear barotrauma. Most of this is preventable with equalisation coaching and, where appropriate, decongestants or tympanostomy tubes arranged by the hyperbaric unit. A clear note about recent ENT surgery or congestion lets the team plan ahead.
Which medications require review before hyperbaric oxygen therapy?
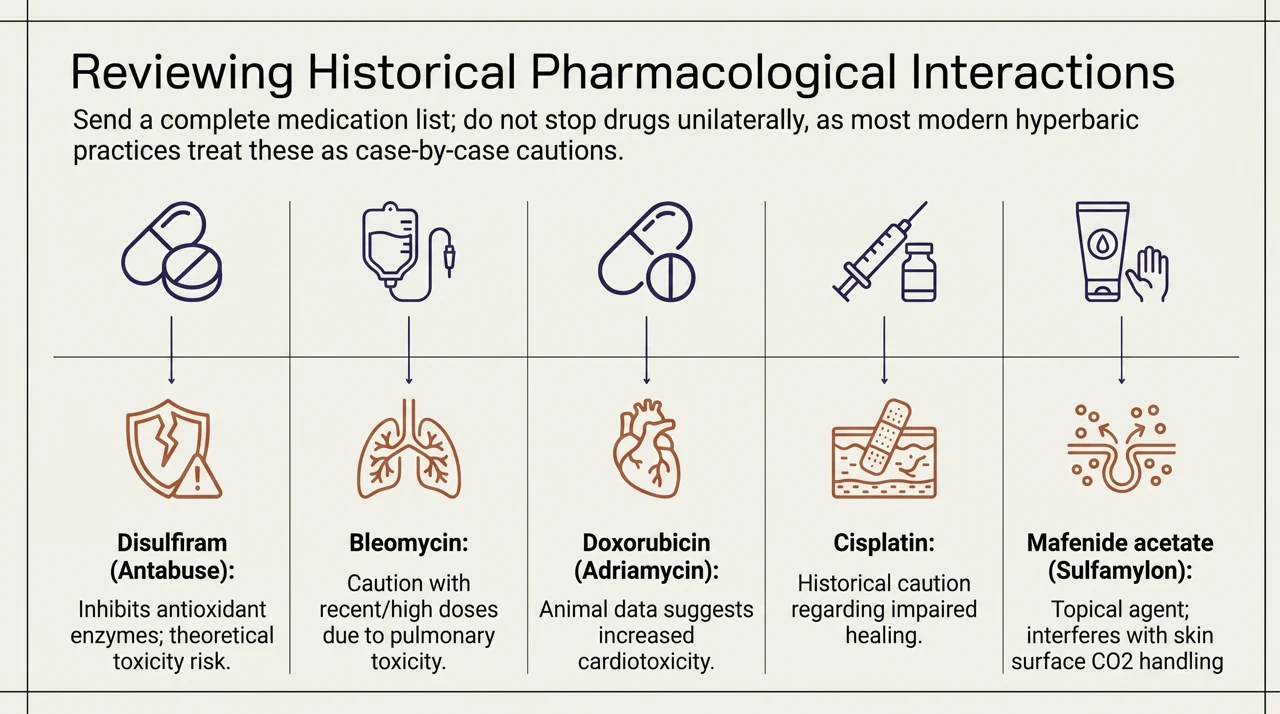
A short list of drugs has historically been flagged for interactions with hyperbaric oxygen, mostly on the basis of older animal data or pharmacological reasoning rather than modern controlled trials. Current hyperbaric practice treats almost all of them as relative cautions that prompt a case-by-case discussion, not as automatic exclusions. The agents most often raised are:
- Disulfiram (Antabuse): inhibits an antioxidant enzyme that helps protect against oxygen free radicals, so it is the drug most consistently linked to a theoretical increase in oxygen toxicity risk
- Bleomycin: long-standing concern about pulmonary toxicity with high oxygen exposure, with recent and high cumulative doses drawing the most caution
- Doxorubicin (Adriamycin): animal data suggested increased cardiotoxicity with concurrent hyperbaric oxygen
- Cisplatin: laboratory data suggested impaired healing, prompting historical caution
- Mafenide acetate (Sulfamylon): a topical burn agent that can interfere with carbon dioxide handling at the skin surface and is generally held before sessions
The practical message for referrers is to send a complete and current medication list, including recent chemotherapy and any topical burn agents, and to let the hyperbaric physician make the final call. Do not stop or change a patient’s medication on the assumption that HBOT is incompatible; in most cases it is not. The UHMS framework and Canadian hyperbaric units keep their guidance current, and the decision is best made jointly. For the regulatory backdrop, Health Canada also addresses HBOT and chamber licensing on its hyperbaric oxygen therapy information page.
What does a quick contraindication check look like?
The table below summarises the safety screen most Canadian hyperbaric units expect a referring physician to consider. It is a starting point for discussion, not a substitute for the unit’s own assessment.
| Category | Examples | Suggested action before referral |
|---|---|---|
| Absolute contraindication | Untreated pneumothorax | Treat and confirm resolution before any HBOT |
| Relative: neurological | Seizure disorder, recent unprovoked seizure, high fever | Document seizure history and current control; flag for protocol adjustment and air breaks |
| Relative: pulmonary | Bullous emphysema, severe COPD with CO2 retention, recent chest surgery, poorly controlled asthma | Consider chest imaging or pulmonary review; note in referral |
| Relative: ENT | Inability to equalise, active URTI, recent ear or sinus surgery | Note congestion or recent surgery; unit arranges equalisation support |
| Relative: medications | Disulfiram, bleomycin, doxorubicin, cisplatin, mafenide acetate | Send full medication and chemotherapy list; do not stop drugs unilaterally |
| Relative: other | Claustrophobia or severe anxiety, pregnancy, uncontrolled diabetes | Mention in referral; chamber type and timing can often accommodate |
What is the screening and referral pathway?
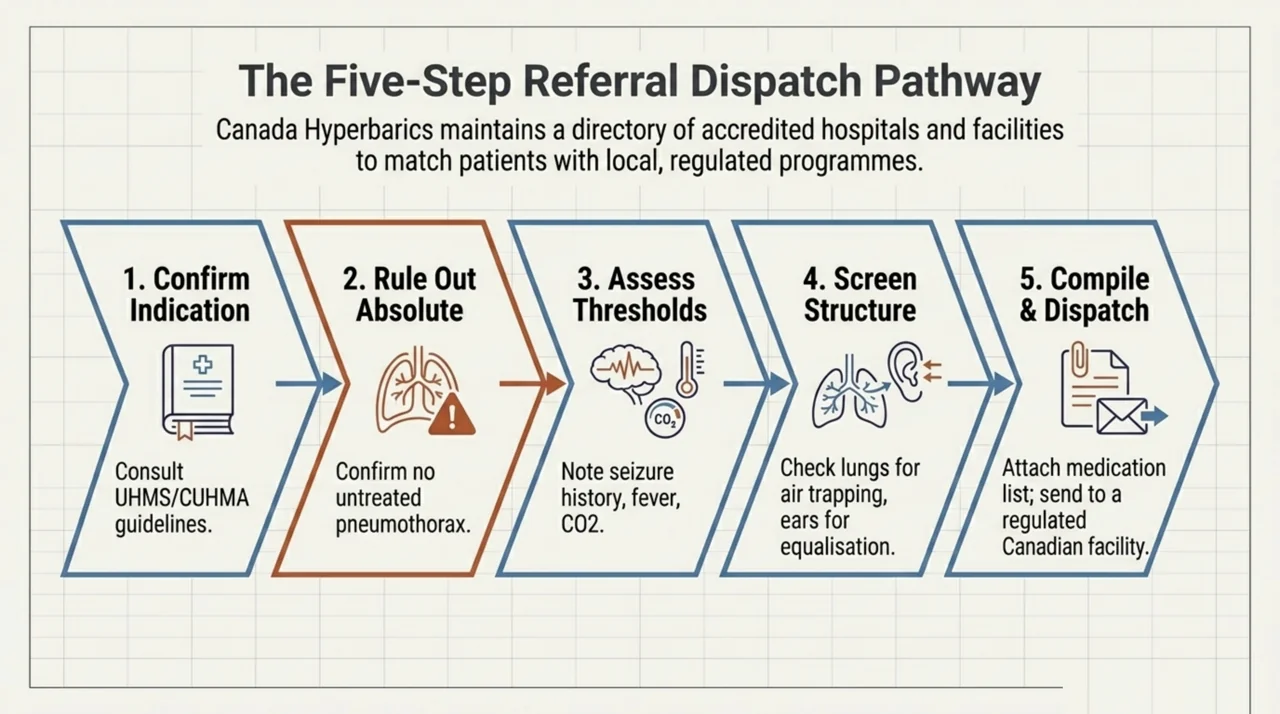
A straightforward way to prepare a safe HBOT referral in Canada is to work through these steps:
- Confirm the indication is one that hyperbaric units treat, using the conditions covered in the Canada Hyperbarics FAQ and condition pages as a guide.
- Rule out an untreated pneumothorax, the one absolute contraindication.
- Take a focused seizure history and note any factor that lowers the seizure threshold.
- Screen the lungs and middle ear for air trapping and equalisation problems.
- Compile a complete, current medication and chemotherapy list.
- Send the referral to a hospital or regulated facility with the relevant history attached, and let the hyperbaric physician finalise the protocol.
Canada Hyperbarics maintains a directory of hospitals and regulated facilities that offer hyperbaric oxygen therapy, so you can match a patient to an accredited program close to home.
Frequently asked questions
Is hyperbaric oxygen therapy safe?
For most patients, yes. Serious adverse events are uncommon when patients are screened and treatment pressures and durations stay within established limits. The main risks, oxygen toxicity seizures and barotrauma, are manageable and largely preventable through proper patient selection and the use of air breaks during sessions.
What is the only absolute contraindication to HBOT?
An untreated pneumothorax. Because pressure changes alter the volume of trapped gas, an undrained pneumothorax can expand dangerously. It must be treated and confirmed resolved before hyperbaric oxygen therapy. All other safety concerns are relative contraindications that require assessment rather than automatic refusal.
Can patients with epilepsy or a seizure disorder have HBOT?
Often, yes, with appropriate screening. A seizure disorder is a relative contraindication because oxygen toxicity can provoke a seizure, but a 2025 Canadian cohort observed only one seizure event among 22 selected patients across 634 sessions. The hyperbaric physician may adjust the treatment pressure and air-break schedule for these patients.
Which medications are a concern with hyperbaric oxygen therapy?
Disulfiram, bleomycin, doxorubicin, cisplatin and topical mafenide acetate are the agents most often flagged, mainly on older or theoretical grounds. In current practice they are relative cautions, not automatic exclusions. Send a complete medication list and let the hyperbaric unit decide; medications should not be stopped on the assumption of incompatibility.
Is HBOT safe during pregnancy?
Pregnancy is treated as a relative consideration rather than a barrier. Hyperbaric oxygen therapy is used in pregnancy for specific emergencies such as carbon monoxide poisoning, where the benefit to mother and foetus outweighs the theoretical risk. For elective indications, timing and dosing are discussed individually with the hyperbaric team.
Can patients with COPD receive hyperbaric oxygen therapy?
Many can. COPD becomes a relative contraindication when there is significant carbon dioxide retention or bullous lung disease, which raise the risk of barotrauma or oxygen toxicity. Chest imaging and a note about disease severity help the hyperbaric unit decide whether and how to proceed safely.
How do I refer a patient for HBOT in Canada?
Confirm the indication, complete the safety screen described above, attach the relevant history and medication list, and send the referral to a hospital or regulated facility offering hyperbaric oxygen therapy. You can find accredited programs through the Canada Hyperbarics directory of hospitals and regulated facilities.
Key takeaways for referring physicians
Hyperbaric oxygen therapy is safe for the large majority of patients. Screen for the one absolute contraindication (untreated pneumothorax), assess oxygen toxicity and seizure risk, check the lungs and middle ear for pressure-related vulnerability, and review the medication list rather than acting on it alone. When in doubt, refer with the relevant history and let the hyperbaric physician tailor the protocol. To find an accredited program, see the directory of hospitals and regulated facilities, and learn more about our editorial approach on the Canada Hyperbarics about page.
This content is for informational purposes only and does not constitute medical advice. It is intended to support, not replace, the clinical judgement of qualified healthcare professionals and the assessment of the treating hyperbaric facility. Always confirm patient suitability with the hyperbaric unit before referral.