
TL;DR: An oxygen toxicity monitoring protocol is a written, auditable procedure that lets a Canadian hyperbaric clinic identify patients at higher risk of central nervous system or pulmonary oxygen toxicity, set treatment-pressure ceilings and mandatory air breaks, recognize the earliest symptoms, and respond safely if a seizure or other toxicity event occurs. Build the protocol around four pillars: pre-treatment screening, dose limits and air-break rules, in-chamber surveillance, and a documented emergency response. Align the protocol with CSA Z275.1, NFPA 99 Chapter 14, and the Undersea and Hyperbaric Medical Society (UHMS) accreditation manual, and review it at least annually.
Hyperbaric oxygen therapy (HBOT) is a medical treatment in which a patient breathes 100% oxygen at a pressure higher than sea level inside a hard-shelled chamber. Oxygen toxicity is the cluster of adverse effects on the central nervous system, lungs, and eyes that can occur when oxygen is breathed at those elevated partial pressures for a sustained period. In a Canadian hyperbaric clinic, central nervous system (CNS) toxicity is the most acute concern because it can present as a seizure with little or no warning, while pulmonary toxicity becomes relevant over many sessions. Every clinic that operates a hyperbaric chamber under Canadian rules needs a written oxygen toxicity monitoring protocol. This guide walks Canadian clinic owners through the steps to build one, audit it, and integrate it with the accreditation and regulatory framework that already governs hyperbaric facilities in Canada.
At Canada Hyperbarics we maintain a directory of more than 30 Canadian hyperbaric facilities, including both hospital and private programmes, and the protocol described here mirrors the framework those facilities operate under. The four pillars are screening, dosing, surveillance, and emergency response, and each pillar is grounded in published evidence and Canadian regulatory text rather than vendor marketing.
What is oxygen toxicity in a hyperbaric setting and why does it need a written protocol?
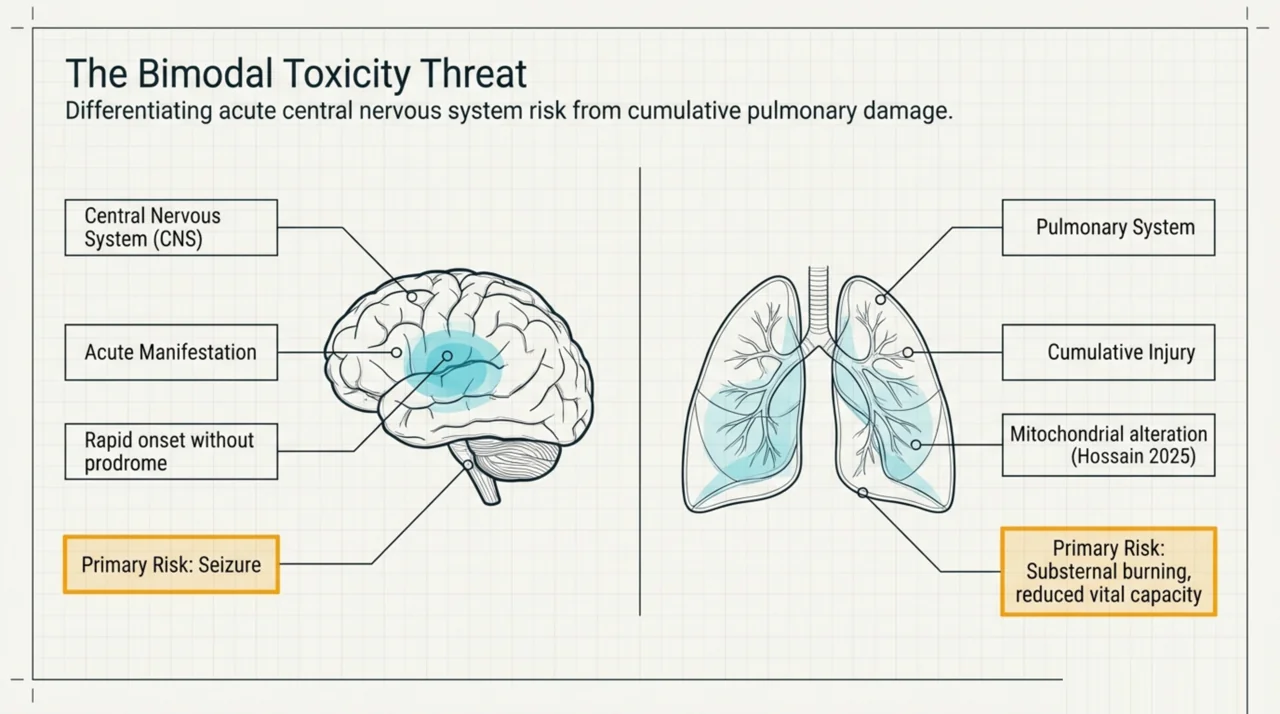
Oxygen toxicity is the dose-related cellular injury caused by elevated partial pressures of oxygen. The two clinically relevant forms in routine HBOT are CNS oxygen toxicity, classically manifesting as a generalized tonic-clonic seizure, and pulmonary oxygen toxicity, manifesting as substernal burning, cough, and reduced vital capacity after cumulative exposure. A 2025 in vitro study by Hossain and colleagues (PubMed | Our Assessment) examined human lung cells exposed to hyperbaric-hyperoxic conditions and reported alterations in mitochondrial dynamics and bioenergetics, which provides mechanistic backing for the long-standing clinical observation that cumulative oxygen exposure matters.
A written protocol matters for three reasons. First, CNS oxygen toxicity events are rare but can present without prodromal warning, so consistent in-chamber surveillance is the only reliable mitigation. Second, Canadian accreditation and standards bodies expect documented patient screening, dosing rules, and emergency procedures rather than informal practice. Third, the protocol creates the audit trail that supports continuous improvement and incident review. The next sections cover each pillar.
How do you screen patients for oxygen toxicity risk before the first session?
Risk screening is the first pillar of the protocol. It is conducted by the prescribing physician or hyperbaric medical director, documented on a structured intake form, and reviewed before every new treatment course. The structured screen captures the patient’s seizure history, current and recent antiepileptic medications, history of bronchospastic or interstitial lung disease, pregnancy status, fever, severe acidosis, and any prior adverse event during HBOT or supplemental oxygen therapy.
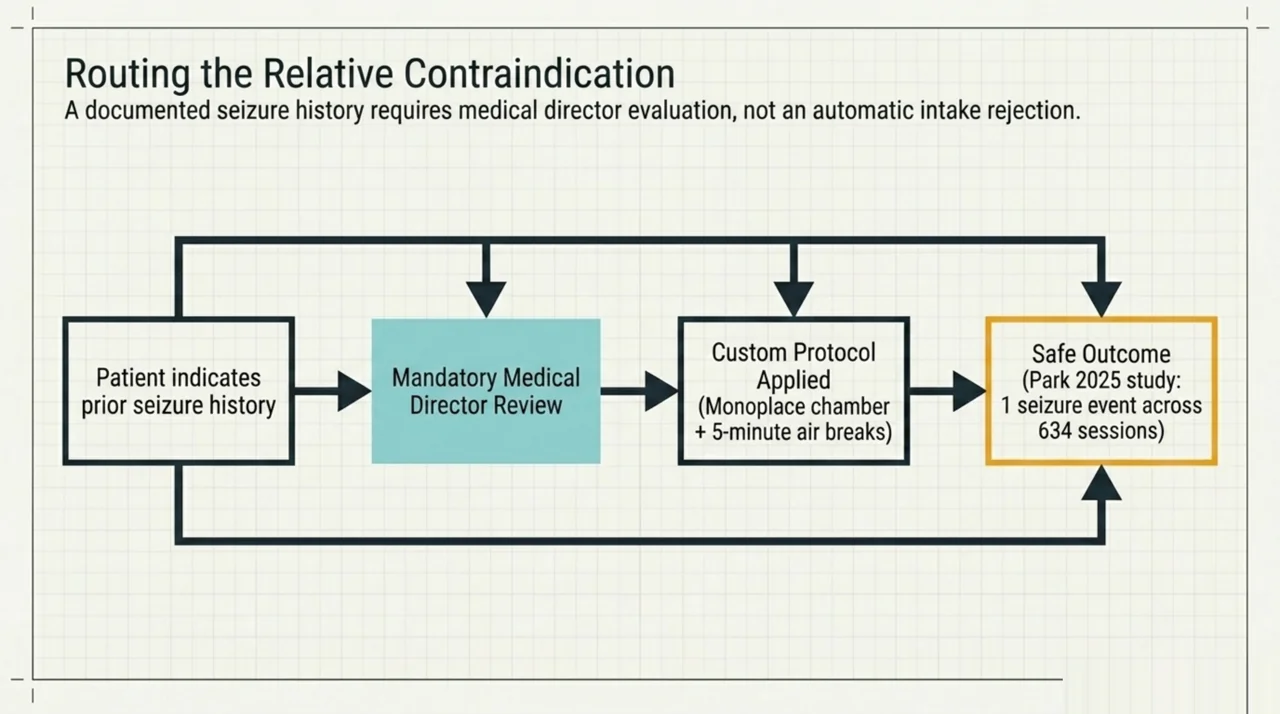
A 2025 retrospective cohort by Park and colleagues at two Toronto-area hyperbaric medicine programmes (PubMed | Our Assessment) followed 22 non-emergent patients with a history of seizures through 634 HBOT sessions delivered in monoplace chambers with five-minute air breaks. One patient experienced a single seizure during the cohort. The authors reported that, in this Canadian referral cohort, a pre-existing seizure history was associated with a low absolute event rate when air breaks and standard screening were applied, though they note the small sample and call for larger studies before changing the relative-contraindication status of a seizure history. The clinical takeaway for a clinic owner is that a documented seizure history requires medical-director review and an explicit dosing modification (typically lower treatment pressure and shorter session length with mandatory air breaks) rather than blanket refusal, and that the screening form must capture the data needed for that decision.
What dosing and air-break rules belong in the protocol?
The dosing pillar translates the screening result into a concrete prescription. The protocol should specify, for every patient, the treatment pressure in atmospheres absolute (ATA), the duration of oxygen breathing at depth, the schedule of air breaks, and the maximum number of sessions before mandatory pulmonary review. The standard Canadian default for publicly funded indications in Canada is 2.0 to 2.4 ATA for 90 minutes with a five-minute air break midway, but the prescription is always set by the hyperbaric physician for the specific indication.
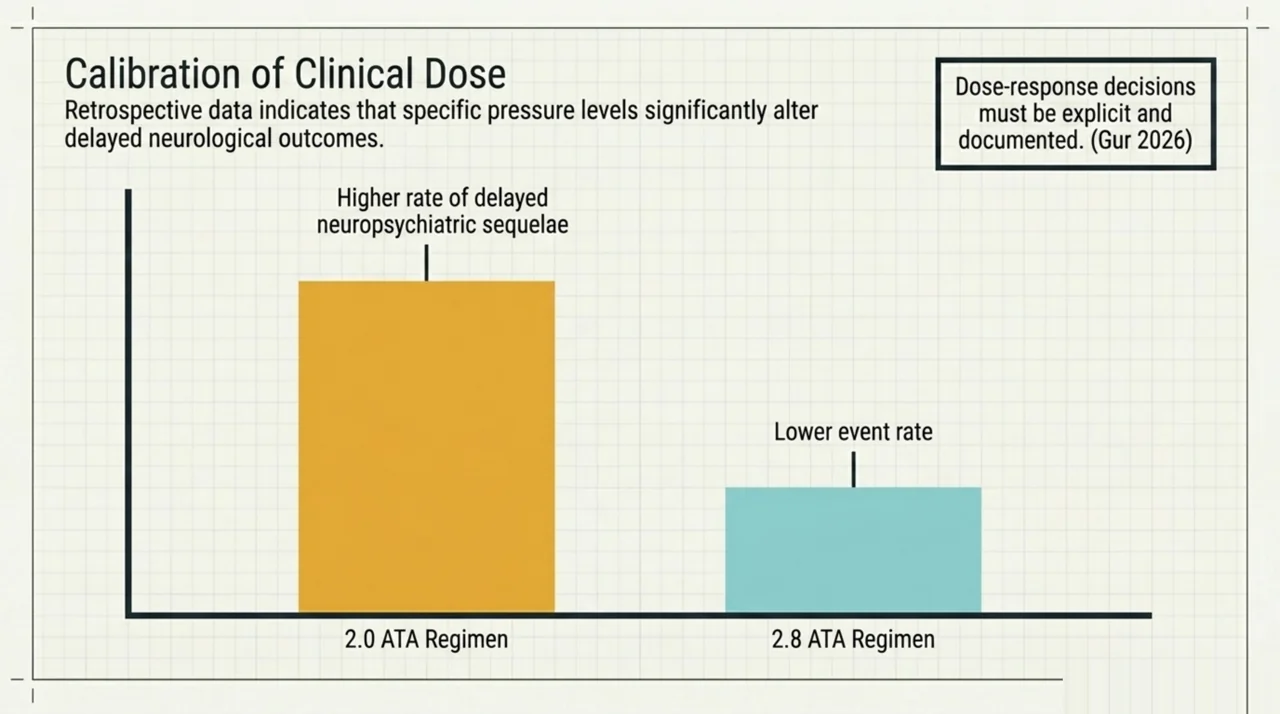
Dose matters. A 2026 retrospective review by Gur and colleagues in Clinical Toxicology (PubMed | Our Assessment) analyzed 312 carbon monoxide poisoning patients across four dosing regimens and found that lower-pressure regimens (2.0 ATA) were associated with a higher delayed-neuropsychiatric-sequelae rate than higher-pressure regimens (2.8 ATA). This is an observational study and the result applies specifically to carbon monoxide treatment, but the broader lesson is that dose-response decisions in HBOT must be explicit and documented rather than left to bedside improvisation. Document the rationale for the chosen pressure in the chart.
Build a separate dosing table for the protocol that maps each recognised indication to its standard pressure, duration, air-break schedule, and review trigger. For technical-diving and rebreather settings the framework around exposure limits has been updated: a 2025 expert-committee revision by Hoyt and colleagues in Diving and Hyperbaric Medicine (PubMed | Our Assessment) revised CNS oxygen toxicity exposure limits at an inspired PO2 of 1.3 atm. The revised guideline applies to technical diving rather than routine HBOT, but it is a useful reference for clinics that handle diving-medicine consults or commercial-diver patients, and it signals that exposure-limit science continues to evolve.
How should staff monitor patients in the chamber?
The surveillance pillar covers what the chamber operator and inside attendant (in a multiplace setting) do during the session. Every protocol should specify minimum monitoring intervals, the early warning signs of CNS oxygen toxicity, communication procedures, and the use of air breaks as both a preventive and a therapeutic tool.
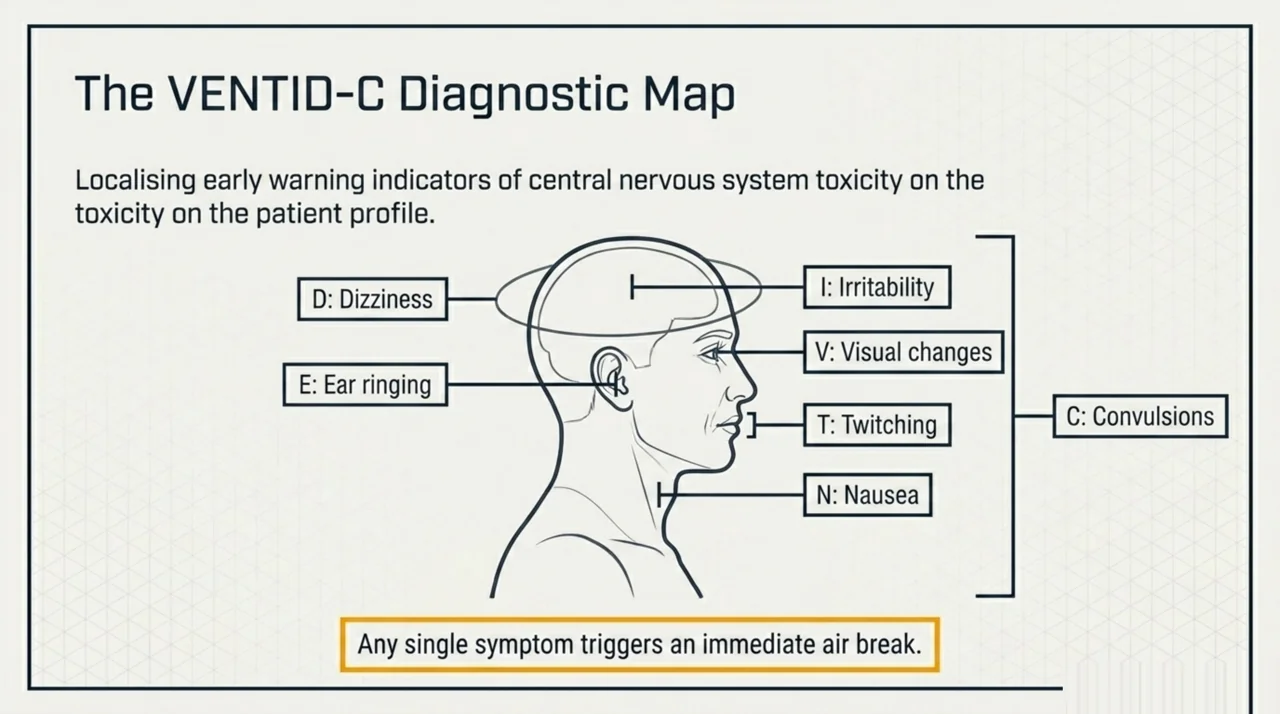
Document the following watch list as part of staff training and the chart-side reference card. The mnemonic VENTID-C (Visual changes, Ear ringing, Nausea, Twitching, Irritability, Dizziness, and Convulsions) is taught widely and should appear on the operator console card. Real-time signs to observe include facial muscle twitching (especially lips and eyelids), nausea, tinnitus, restlessness, lightheadedness, and unusual visual or auditory complaints. Any single symptom triggers an immediate air break and a re-evaluation by the medical director on call.
| Monitoring element | Frequency | Documentation |
|---|---|---|
| Verbal contact with patient | Every 5 minutes minimum | Session log |
| Vital signs (HR, SpO2 outside chamber) | Pre, mid, post-session | Treatment record |
| VENTID-C symptom check | Every 10 minutes during O2 breathing | Session log |
| Air-break compliance | Every scheduled break | Session log |
| Operator-physician communication | As needed, threshold low | Incident log if escalated |
What should the emergency response procedure look like?
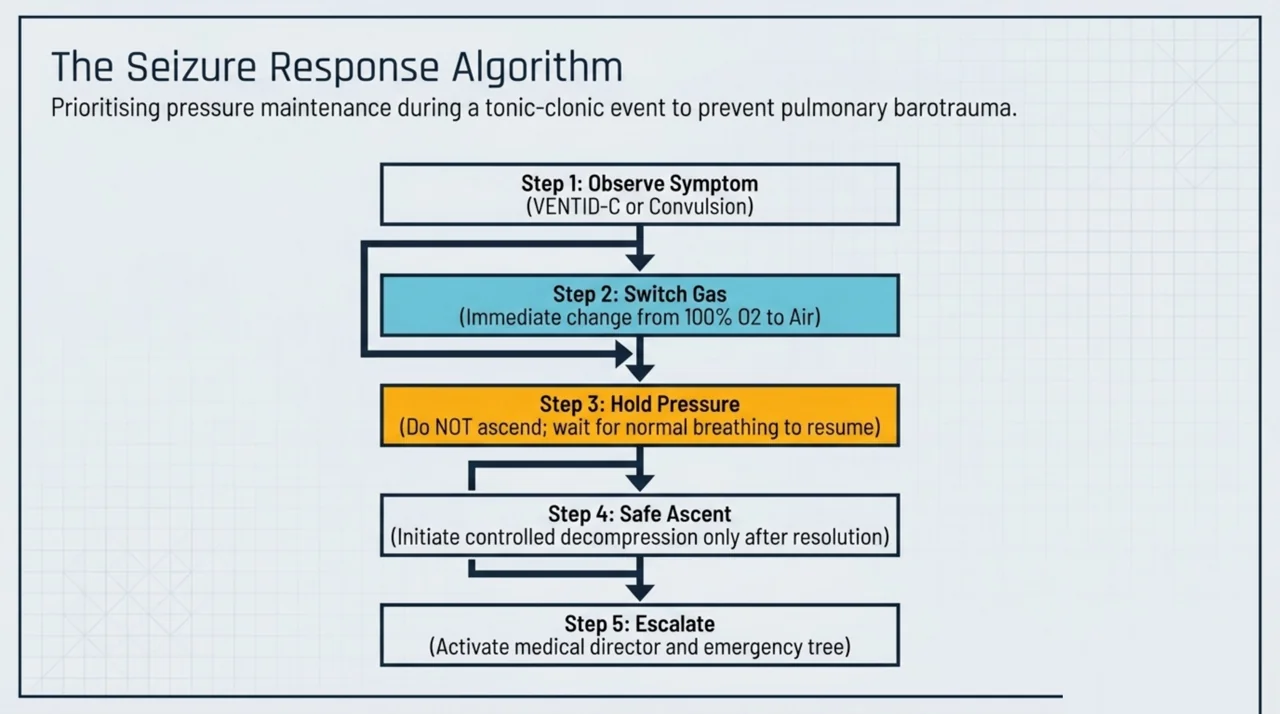
The emergency response pillar is the part of the protocol that gets practiced rather than read. It covers the response to a suspected or confirmed oxygen toxicity seizure, including the decision tree on when to descend, when to switch to air, when to escalate to emergency services, and how to document the event. Three procedural items belong in every Canadian clinic owner’s plan.
- Switch the breathing gas to air immediately if a seizure or pre-seizure symptom is observed. Continuing oxygen at depth during a convulsion increases the risk of pulmonary barotrauma during the uncontrolled breath hold that often accompanies a seizure.
- Maintain pressure until the seizure resolves and the patient is breathing normally before initiating a controlled ascent, unless a separate clinical reason requires an emergency decompression. This is the standard hyperbaric medicine guidance because ascending during a tonic-clonic episode raises the risk of pulmonary barotrauma.
- Activate the medical director and emergency services according to a written escalation tree. The tree should specify exactly who is called, in what order, and what is communicated. Drills should run at least quarterly.
After any suspected event, complete a structured incident report, schedule a debrief within 72 hours, and review whether the screening, dosing, or surveillance pillars need modification. Incident reporting requirements for Canadian clinics are summarized in our overview of Canadian hyperbaric regulation and our coverage of provincial access includes the relevant provincial reporting contacts.
How does the protocol fit Canadian regulatory and accreditation requirements?
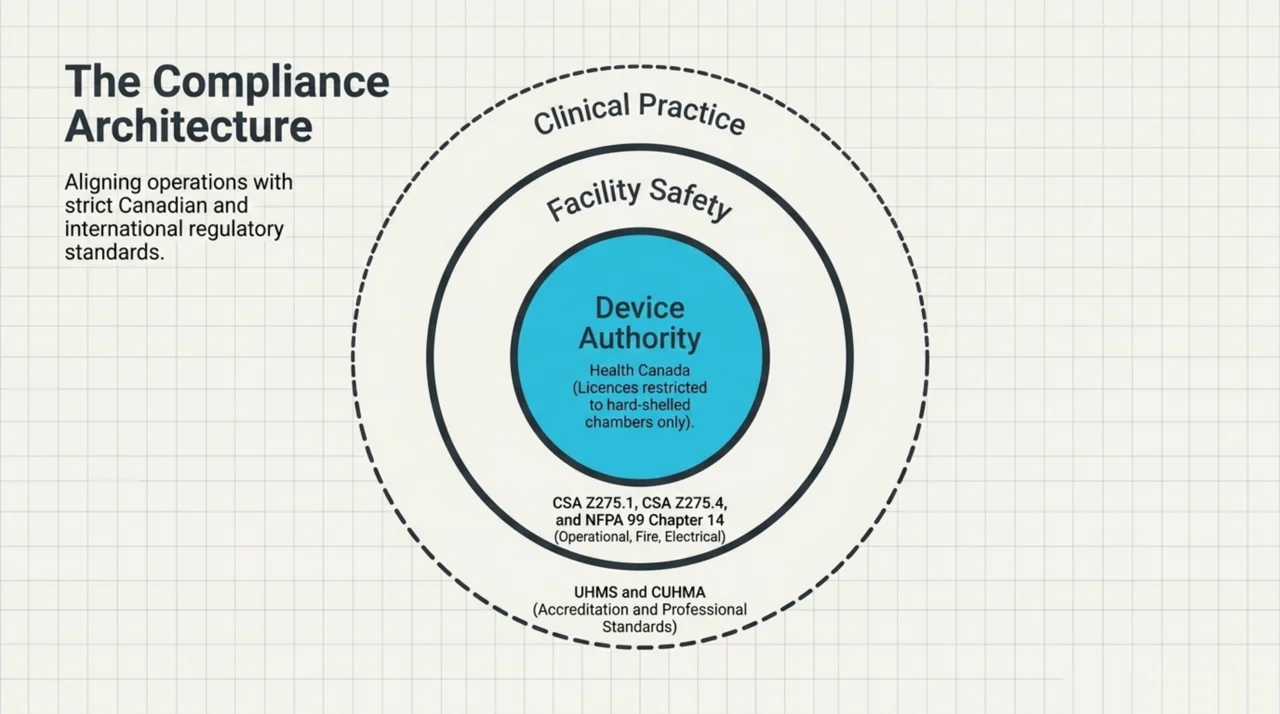
The protocol must satisfy four overlapping frameworks. Health Canada regulates the chamber itself as a medical device and has issued device licences only for hard-shelled chambers used for the Undersea and Hyperbaric Medical Society recognised indications, as described on the Government of Canada’s official hyperbaric oxygen therapy page. Operational safety standards for the chamber and the facility are set by CSA Z275.1 (Hyperbaric facilities) and CSA Z275.4 (Competency standards for diving, caisson, and hyperbaric operations). Fire and electrical safety in hyperbaric environments is governed by NFPA 99 Chapter 14. Voluntary clinical-facility accreditation is delivered by the UHMS Hyperbaric Facility Accreditation Program, and Canadian professional standards of practice are maintained by the Canadian Undersea and Hyperbaric Medical Association (CUHMA).
The protocol should cross-reference each of these documents in its preamble so that surveyors, auditors, and new staff can trace each procedural rule back to the authoritative source. CUHMA publishes guidelines on staff qualifications and the standard of care that should be cited alongside the dosing and surveillance pillars, and the UHMS manual is the most detailed practical reference for facility-level accreditation expectations.
How often should the protocol be reviewed?
Review at least annually, after any incident or near-miss, and whenever a referenced standard publishes a revision. The annual review should include a documented evidence scan (UHMS, CUHMA, CSA, NFPA, Health Canada notices), an internal audit sample of at least 20 recent treatment records, a tabletop drill of the seizure response, and a sign-off by the medical director. Keep prior versions on file. Auditors expect to see the version history.
Frequently asked questions about oxygen toxicity monitoring in HBOT
Is a seizure history an absolute contraindication to HBOT?
Most Canadian hyperbaric programmes treat seizure history as a relative, not absolute, contraindication. The Park 2025 retrospective cohort reported a low observed event rate when patients were screened, treated in monoplace chambers, and given five-minute air breaks. The medical director sets the final decision case by case.
What is the most common early sign of CNS oxygen toxicity?
There is no reliably consistent prodromal symptom. Reported early signs include facial twitching, nausea, tinnitus, irritability, and visual changes (the VENTID-C mnemonic). Any single symptom should trigger an immediate air break.
Do air breaks actually reduce risk?
Air breaks are the standard preventive measure in HBOT and are built into virtually every modern treatment table. They are designed to allow tissue PO2 to fall briefly and reduce cumulative CNS oxygen exposure. The Park 2025 Canadian cohort, in which all sessions used five-minute air breaks, observed only one seizure across 634 sessions.
How are oxygen toxicity events reported in Canada?
Adverse events involving the chamber itself follow Health Canada’s medical device problem-reporting pathway. Clinical incidents follow provincial regulatory reporting requirements and the clinic’s internal incident-management policy. UHMS-accredited facilities also report through the accreditation framework.
Does the protocol apply to soft-shelled chambers?
Health Canada has not issued medical device licences for soft-shelled chambers for HBOT delivery in recognised indications. A Canadian clinical hyperbaric programme operates a hard-shelled chamber that has been issued a Health Canada medical device licence, which is the only chamber type the regulatory and standards framework described here applies to.
How does an oxygen toxicity protocol affect insurance and accreditation?
A documented and audited protocol is one of the safety pillars surveyors look for during UHMS accreditation and during a clinic’s professional liability assessment. Most insurers expect to see written screening, dosing, surveillance, and emergency response procedures with version control and training records.
How often should staff drill the seizure response?
Most accredited programmes drill at least quarterly. A tabletop drill is acceptable for most cycles, with a full simulation at least annually.
Next steps for Canadian clinic owners
Start by mapping your current screening intake, dosing rules, in-chamber surveillance procedures, and emergency response against the four pillars above. Cross-reference each procedural rule against CSA Z275.1, NFPA 99 Chapter 14, the UHMS accreditation manual, and the relevant Health Canada device-licence conditions. Document gaps, assign owners, and set a target close-out date. To compare facility-level practice across Canada, browse our directory of hospitals and regulated facilities offering HBOT, and our overview of conditions treated with HBOT in Canada. Canada Hyperbarics maintains both directories as independent reference resources for clinic owners, referring physicians, and patients.
This content is for informational purposes only and does not constitute medical advice. It is intended as an operational reference for hyperbaric clinic owners and medical directors in Canada and does not replace site-specific clinical or regulatory consultation. Always consult a qualified hyperbaric physician and review the current edition of all referenced standards before adopting or modifying a clinical protocol.