
Hyperbaric oxygen therapy (HBOT) is being investigated as an adjunctive intervention in Parkinson’s disease, with recent meta-analyses pooling small Chinese-language and English-language randomised and quasi-experimental studies. The 2024 and 2025 evidence base remains modest in size and consistent in direction: HBOT is associated with measurable improvements in non-motor symptoms (sleep, depression, anxiety, cognition) and modest reductions in motor severity scales when added to standard pharmacological care. No phase III trial has yet established HBOT as a disease-modifying therapy, and Health Canada does not list Parkinson’s disease among the medical device licensing recognised indications for hyperbaric chambers. This 2024-2026 evidence review summarises the most recent systematic reviews, meta-analyses, and mechanistic work relevant to Canadian HBOT researchers.
TL;DR: Three 2024-2025 meta-analyses (pooled n approx. 2,700) consistently report that HBOT, when added to standard Parkinson’s treatment, was associated with improved motor severity scales (UPDRS III), sleep efficiency, depression and anxiety scores, and cognitive screening measures. The underlying trial quality is low to moderate, most studies originate in Chinese centres, and there is no current Canadian RCT. The next research priorities for Canadian investigators are sham-controlled dosing trials and longer follow-up windows.
What is the current evidence base for HBOT in Parkinson’s disease?
Parkinson’s disease (PD) is a progressive neurodegenerative disorder characterised by dopaminergic neuron loss in the substantia nigra, leading to motor symptoms (bradykinesia, rigidity, tremor, postural instability) and a wide range of non-motor symptoms (sleep disturbances, depression, cognitive decline, autonomic dysfunction). The rationale for investigating HBOT in PD draws on three lines of mechanistic reasoning: improved cerebral oxygenation in hypoxic basal ganglia regions, modulation of mitochondrial function and oxidative stress, and possible effects on neurotrophic factor expression.
Three recent meta-analyses anchor the current literature. Pan and colleagues (2025) reviewed sixteen studies totalling 1,324 patients and reported that HBOT was associated with significant improvements compared with baseline on the Hamilton Anxiety Scale, the Hamilton Depression Scale, the Montreal Cognitive Assessment, and the Mini-Mental State Examination (all p < 0.05) (PubMed | Our Assessment). Bu and colleagues (2025) pooled thirteen studies with 958 participants and reported a higher treatment efficacy rate in the HBOT-adjunct group (odds ratio 3.18, 95% CI 1.60-6.33), along with a lower UPDRS III motor score (mean difference -2.96, 95% CI -4.31 to -1.61) (PubMed | Our Assessment).
A third meta-analysis by Tan and colleagues (2024) focused specifically on sleep disorders in PD and synthesised seven RCTs with 461 participants. The pooled analysis reported that adjunctive HBOT was associated with substantially improved sleep efficiency (mean difference 15.26, 95% CI 10.89-19.63) (PubMed | Our Assessment). The same research team published a protocol in 2024 for a separate systematic review specifically on PD with cognitive dysfunction, which is expected to report once the search window closes (PubMed | Our Assessment).
What outcomes have been reported across the three pooled analyses?
| Outcome domain | Lead meta-analysis | Pooled n | Reported effect |
|---|---|---|---|
| Motor severity (UPDRS III) | Bu 2025 | 958 | Mean diff -2.96 (95% CI -4.31 to -1.61) |
| Treatment efficacy rate | Bu 2025 | 958 | OR 3.18 (95% CI 1.60-6.33) |
| Sleep efficiency | Tan 2024 | 461 | Mean diff 15.26 (95% CI 10.89-19.63) |
| Anxiety and depression scales | Pan 2025 | 1324 | Significant change vs baseline (p < 0.05) |
| Cognitive screening (MoCA, MMSE) | Pan 2025 | 1324 | Significant change vs baseline (p < 0.05) |
The directional consistency across the three meta-analyses is notable. Each reports HBOT as associated with improvement in its respective primary outcome at conventional statistical thresholds. The effect sizes are clinically modest rather than dramatic: a 2.96-point reduction on UPDRS III represents a meaningful but not transformative change in motor severity, and the absolute confidence intervals remain comfortably away from zero in each domain.
What does the underlying mechanistic literature suggest?
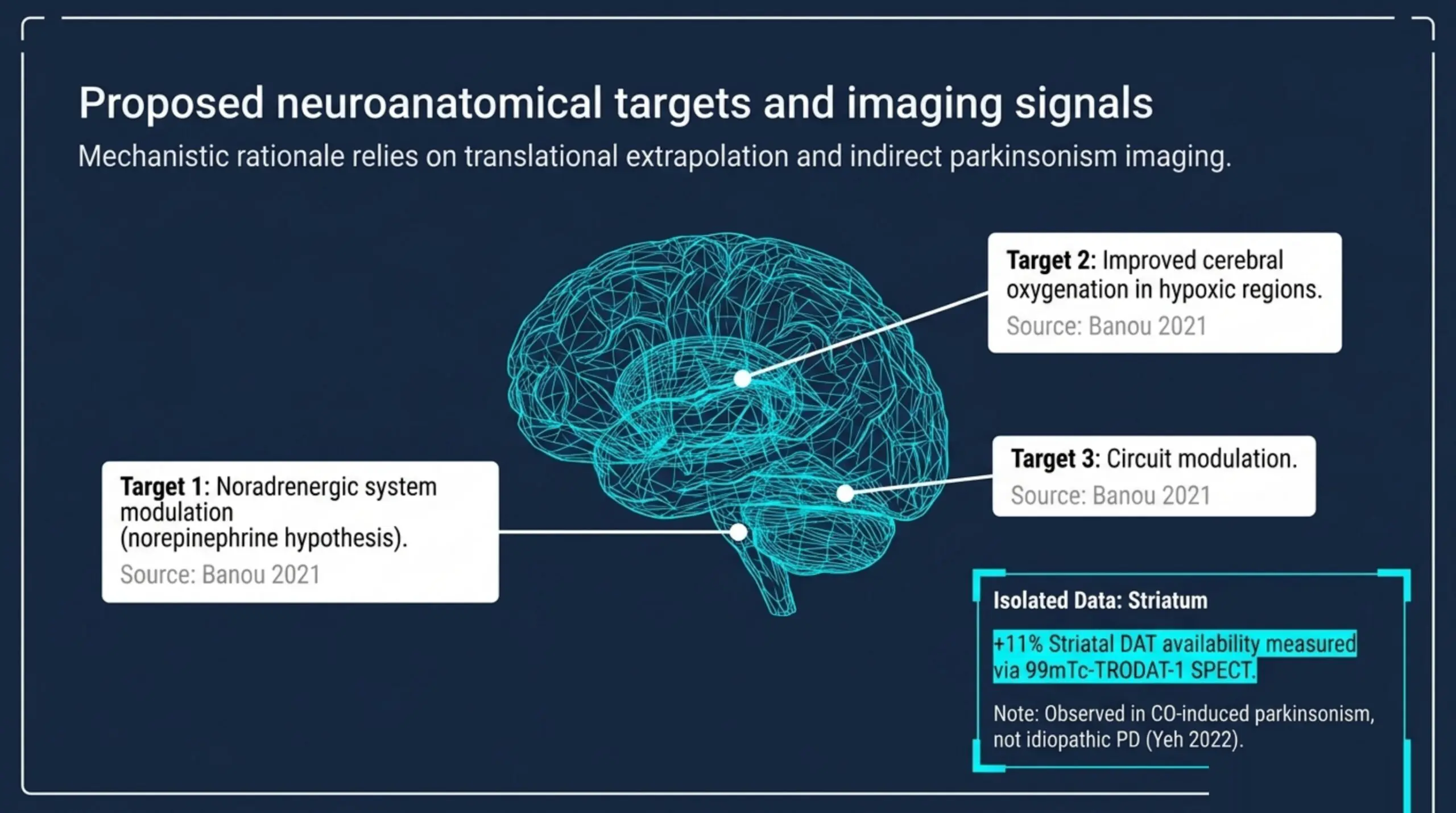
Banou (2021) reviewed mechanistic candidates for HBOT effects on Parkinson’s disease and proposed three circuits as the likely substrate: the noradrenergic system (particularly the locus coeruleus), the basal ganglia, and the cerebellum. The review presents a “norepinephrine hypothesis” in which HBOT-associated increases in norepinephrine levels may contribute to the observed motor improvements (PubMed | Our Assessment). The mechanistic case is preliminary and rests on translational extrapolation rather than direct human dopaminergic imaging.
One imaging study does exist for a related condition. Yeh and colleagues (2022) examined 21 patients with delayed neuropsychiatric syndrome (DNS) following acute carbon monoxide poisoning, a population in which CO-induced parkinsonism is well documented. The investigators used 99mTc-TRODAT-1 single-photon emission computed tomography (SPECT) to quantify dopamine transporter (DAT) availability in the striatum before and after HBOT. Striatal DAT availability increased by approximately 11% on average after HBOT in this cohort (PubMed | Our Assessment). The result is hypothesis-generating for idiopathic PD but does not directly demonstrate dopaminergic recovery in classical Parkinson’s disease.
Earlier case-level evidence pointed in the same direction. Xu and colleagues (2018) described a single PD patient with severe comorbid depression and anxiety who declined dopamine agonists and SSRIs, and was treated with 30 daily HBOT sessions. The case report documented improved scores on UPDRS I, UPDRS II, Hamilton Depression Rating Scale, and Hamilton Anxiety Rating Scale (PubMed | Our Assessment). A case report cannot establish causation, but the result is consistent with the pooled meta-analytic direction.
What are the key limitations of the current evidence?
Three structural limitations recur across the 2024-2025 meta-analyses and constrain what can be inferred for Canadian practice.
- Trial quality is uneven. The Pan 2025 and Bu 2025 reviews include both randomised controlled trials and pre-post or quasi-experimental designs. Methodological quality was assessed using the Cochrane risk-of-bias tool and was rated as low to moderate across most included studies. Blinding to sham pressure is rarely reported.
- Geographic and language concentration. The vast majority of source studies are conducted in Chinese centres and many are published in Chinese-language journals. The Pan 2025 search drew from Chinese Science and Technology Periodical Database, SinoMed, and Wanfang, in addition to PubMed and Cochrane. Generalisability to Canadian populations under Health Canada-regulated chambers is not directly established.
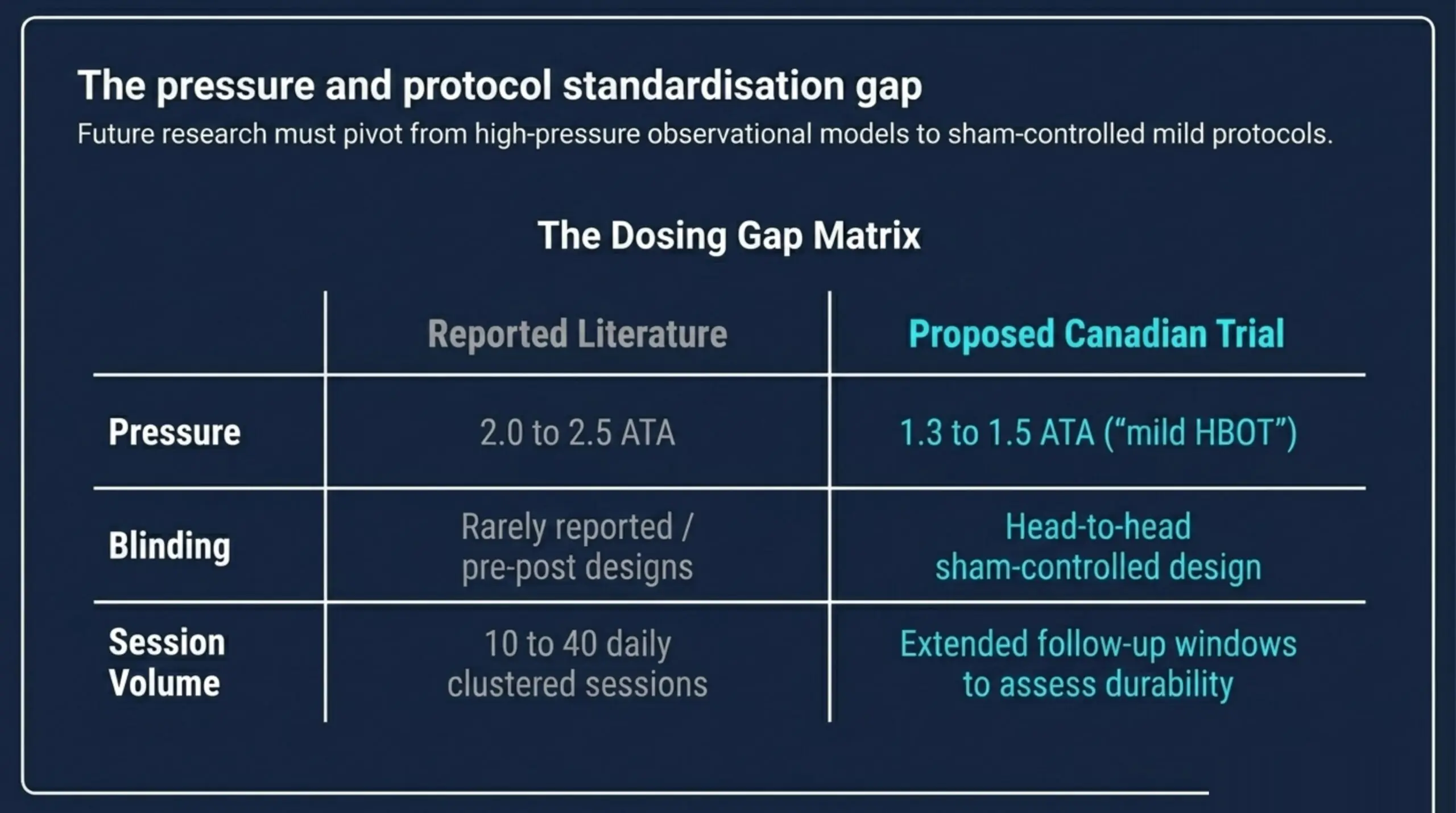
- Dose heterogeneity is high. Treatment protocols vary in pressure (typically 1.5 to 2.5 ATA), number of sessions (10 to 40 across pooled studies), and duration per session. No optimal dosing regimen has been established for PD specifically.
An additional contextual point: Parkinson’s disease is not listed among the UHMS recognised indications for hyperbaric oxygen therapy. Health Canada has issued medical device licensing for hyperbaric chambers but does not designate disease-specific approved uses in the same manner as a pharmaceutical indication. Researchers and clinicians should treat HBOT in PD as an investigational adjunct, not as a standard-of-care intervention.
How does this evidence translate to the Canadian research landscape?
Canada Hyperbarics maintains a public-facing research database indexing peer-reviewed HBOT literature, including the studies summarised here. To date, no Canadian-led randomised controlled trial of HBOT in Parkinson’s disease has been published. Three areas appear most actionable for Canadian investigators:
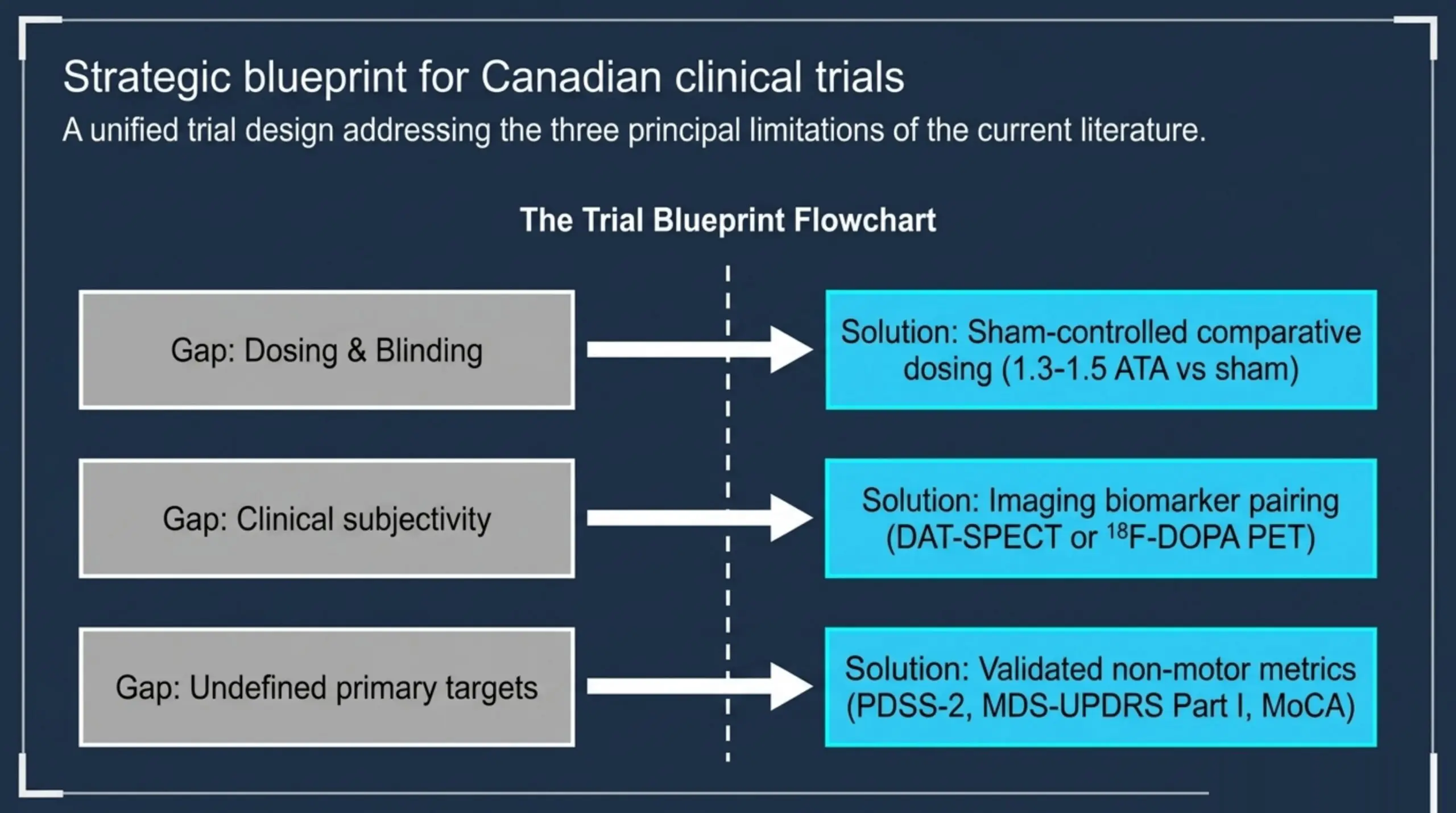
- Sham-controlled dosing comparison. The 2.0 to 2.5 ATA range used in most pooled studies is high relative to the 1.3 to 1.5 ATA “mild HBOT” range studied for some neurological indications. A head-to-head sham-controlled design comparing two pressure levels would address both the dosing gap and the blinding gap in one trial.
- Imaging biomarker pairing. Pairing UPDRS outcomes with DAT-SPECT or 18F-DOPA PET would address whether observed clinical improvements correlate with measurable nigrostriatal changes, beyond the indirect signal from the Yeh 2022 CO-induced cohort.
- Non-motor symptom focus. The strongest pooled effects to date are in sleep, mood, and cognition. A Canadian non-motor-symptom trial with validated PD-specific outcome measures (PDSS-2 for sleep, MDS-UPDRS Part I for non-motor, MoCA for cognition) would extend the existing evidence into a population reflective of Canadian access patterns.
Frequently asked questions
Is hyperbaric oxygen therapy approved for Parkinson’s disease in Canada?
No. Health Canada has not licensed any hyperbaric chamber for Parkinson’s disease as a recognised indication, and the UHMS does not list Parkinson’s disease among its 14 recognised indications. HBOT for PD is currently investigational. Patients pursuing HBOT for Parkinson’s in Canada do so through hospitals and regulated facilities on an off-label or research basis.
How large is the pooled patient population in current meta-analyses?
Across the three principal 2024-2025 meta-analyses (Pan, Bu, Tan), the pooled patient population is approximately 2,700 participants. There is substantial study overlap between Pan 2025 and Bu 2025, so the unique participant count is meaningfully smaller. No single trial in the literature exceeds approximately 200 participants.
What outcome measures are most consistently used?
The Unified Parkinson’s Disease Rating Scale (UPDRS) Parts I-III is the most widely used motor and non-motor measure. Secondary measures include the Pittsburgh Sleep Quality Index, the Epworth Sleepiness Scale, the Hamilton Depression and Anxiety Scales, the Mini-Mental State Examination, and the Montreal Cognitive Assessment. Hoehn-Yahr staging appears in approximately half of the pooled trials.
Are there imaging studies of HBOT effects on the dopaminergic system?
One published imaging study used 99mTc-TRODAT-1 SPECT to measure striatal dopamine transporter availability before and after HBOT in patients with CO-induced delayed neuropsychiatric syndrome, a parkinsonism-prone population. Striatal DAT availability rose by approximately 11% on average. No comparable imaging study has been published in idiopathic Parkinson’s disease.
What protocols are reported in the meta-analyses?
Reported protocols cluster around 2.0 to 2.5 ATA, sessions of 60 to 90 minutes, delivered daily or near-daily for 10 to 40 total sessions. Specific protocols vary by centre and are not standardised. No head-to-head dosing trial has been published.
Are there safety concerns specific to Parkinson’s disease patients?
The reviewed trials do not report PD-specific adverse events beyond the standard HBOT side-effect profile (ear barotrauma, transient myopia, oxygen toxicity at higher pressures). PD patients with orthostatic hypotension or advanced cognitive impairment may require additional screening; this is a published gap in the literature rather than a documented signal of harm.
What further research is needed?
The field would benefit from larger sham-controlled randomised trials, head-to-head dosing comparisons, imaging biomarker pairings (DAT-SPECT or 18F-DOPA PET), longer follow-up windows to assess durability of effect, and trials conducted outside Chinese centres to address generalisability. A Canadian-led trial would directly address the geographic concentration of the current evidence base.
What should Canadian researchers conclude from the 2024-2026 evidence?
The current evidence base for HBOT in Parkinson’s disease is internally consistent in direction and modest in effect size. Three pooled analyses report associations between adjunctive HBOT and improvements across motor severity scales, non-motor symptom domains, and sleep efficiency. The supporting mechanistic and imaging literature is preliminary but pointed in the same direction. None of the published evidence is sufficient to establish HBOT as a disease-modifying treatment, and Health Canada has not approved this indication.
For Canadian investigators, the gap is clearly structured: a sham-controlled, dose-comparative, biomarker-paired Canadian trial would address the three principal limitations of the current literature in a single design. For referring physicians and patients exploring HBOT in this context, the appropriate framing remains “investigational adjunct” rather than “approved therapy.” Canada Hyperbarics maintains a directory of hospitals and regulated facilities across Canada that can be consulted by patients and researchers planning future clinical work.
Medical disclaimer
This content is for informational purposes only and does not constitute medical advice. Hyperbaric oxygen therapy for Parkinson’s disease is currently investigational in Canada and is not an approved indication. Patients considering HBOT should consult their treating neurologist and a hyperbaric medicine specialist at a regulated facility.