
TL;DR: Three 2026 systematic reviews and one large 2026 longitudinal cohort have meaningfully advanced the evidence base for hyperbaric oxygen therapy as a non-pharmacologic intervention for sleep disturbances. The signal is clearest for post-traumatic brain injury insomnia, for sleep quality in healthy aging and long COVID, and for selected sleep-breathing-disorder phenotypes. The signal is weakest for randomised head-to-head comparisons against cognitive behavioural therapy for insomnia (CBT-I). Canadian researchers are well positioned to address the most important gap: confirmatory multicentre RCTs with standardised pressure protocols and validated polysomnography endpoints.
Hyperbaric oxygen therapy (HBOT) is a medical treatment in which a patient breathes 100 percent oxygen inside a pressurised chamber, typically at 2.0 to 2.5 atmospheres absolute. The intervention has long-established Health Canada and UHMS indications for decompression sickness, carbon monoxide poisoning, selected chronic wounds, and a defined set of other conditions. Over the past 18 months, sleep medicine has emerged as a distinct area of investigation: four substantive 2026 publications now frame the evidence on HBOT for sleep disturbances, and the picture is more nuanced than the earlier mixed-condition literature suggested. This review summarises what those publications report, where the methodology is strongest, and where Canadian research groups can contribute most.
Canada Hyperbarics tracks every published HBOT study and indexes it inside a searchable Canadian research database. This article draws exclusively from the four 2026 sleep-focused studies in that database, plus two 2026 mechanism reviews that contextualise the biological rationale.
What does the 2026 evidence say about HBOT for sleep disturbances?
Sleep disturbances after brain injury, in chronic neuroinflammatory conditions, and in respiratory phenotypes such as obstructive sleep apnea share an underlying theme: dysregulated oxygenation during sleep. The 2026 evidence base for HBOT for sleep disturbances is small but converging. It is anchored by three systematic reviews and one prospectively analysed longitudinal cohort, all published within a 12-month window:
| Study | Design | Population | Sleep outcome |
|---|---|---|---|
| Loong et al. 2026 (Brain Impair) | Systematic review and meta-analysis, 12 RCTs | Adults with post-TBI sleep disturbances | PSQI, ISI, ESS |
| Wang et al. 2026 (J Head Trauma Rehabil) | Network meta-analysis, 22 RCTs, n=1299 | TBI-related sleep disorders | PSQI, ISI, ESS |
| Doenyas-Barak et al. 2026 (Front Neurol) | Retrospective longitudinal cohort, n=395 | Healthy aging, long COVID, PTSD | PSQI total and components |
| Duong-Quy et al. 2026 (Pulm Ther) | Systematic review | Sleep breathing disorders (OSA, CSA, altitude-related) | Physiological and clinical endpoints |
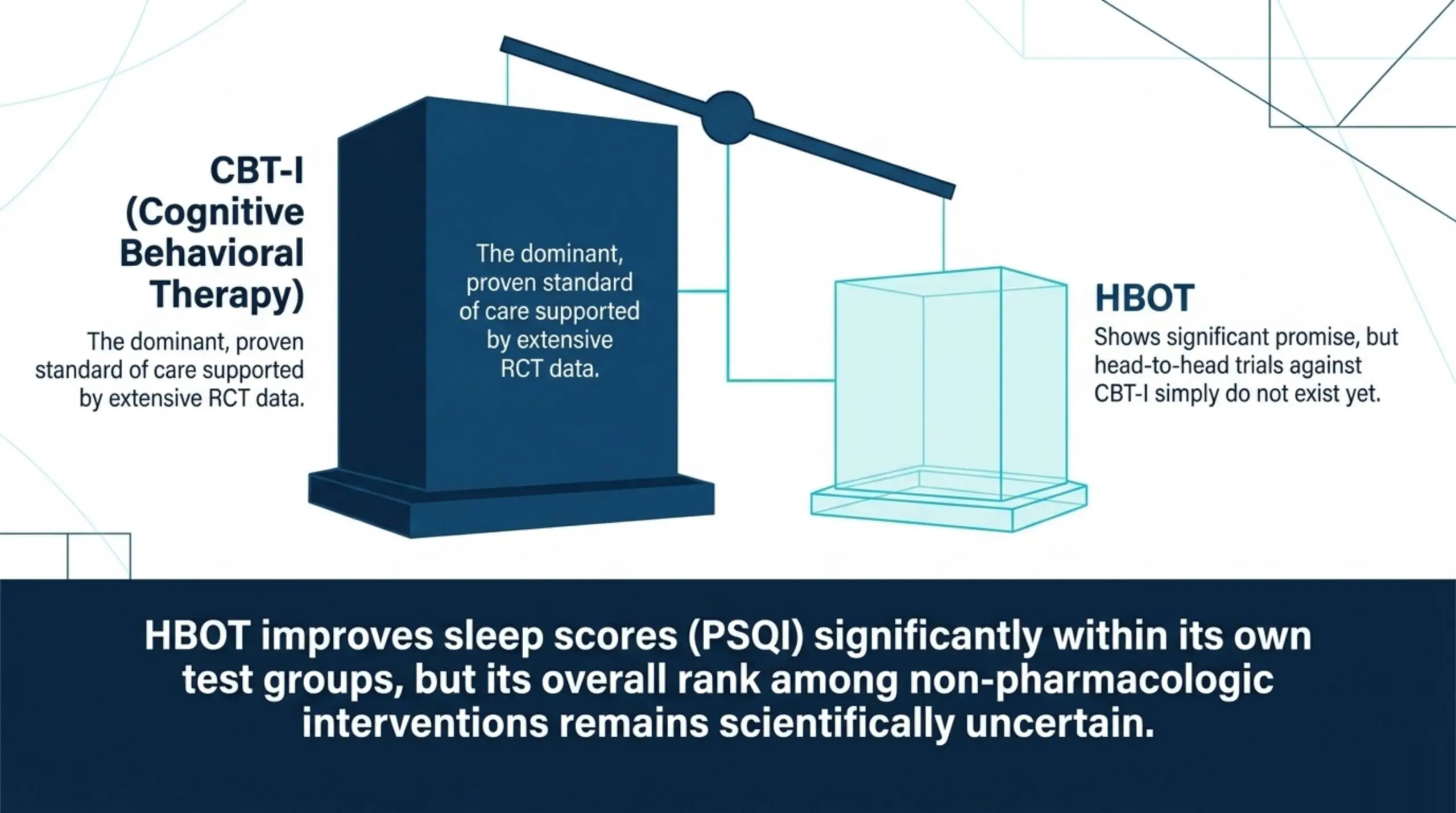
The headline finding across the four publications is that HBOT was consistently associated with statistically significant within-subject improvements in sleep quality, but its rank among non-pharmacologic interventions remains uncertain because head-to-head RCT data are scarce. CBT and CBT-I dominate the comparator landscape in both Loong et al. and Wang et al., reflecting CBT’s much larger evidence base rather than a demonstrated superiority over HBOT in matched trials.
How does HBOT plausibly modulate sleep physiology?
The mechanistic case for HBOT in sleep disturbances rests on its broader physiological effects. Bhargava et al. 2026 (Curr Med Chem) (PubMed) describe HBOT as a dose-dependent intervention that increases dissolved oxygen delivery to hypoxic tissues, provides neuroprotection following central nervous system trauma, and operates under protocols established by the Undersea and Hyperbaric Medical Society (UHMS) and the European Underwater and Baromedical Society. Wang X 2026 (Med Gas Res) (PubMed) notes positive effects in craniocerebral trauma, cerebrovascular disease, intracranial infections, and intracranial tumours.
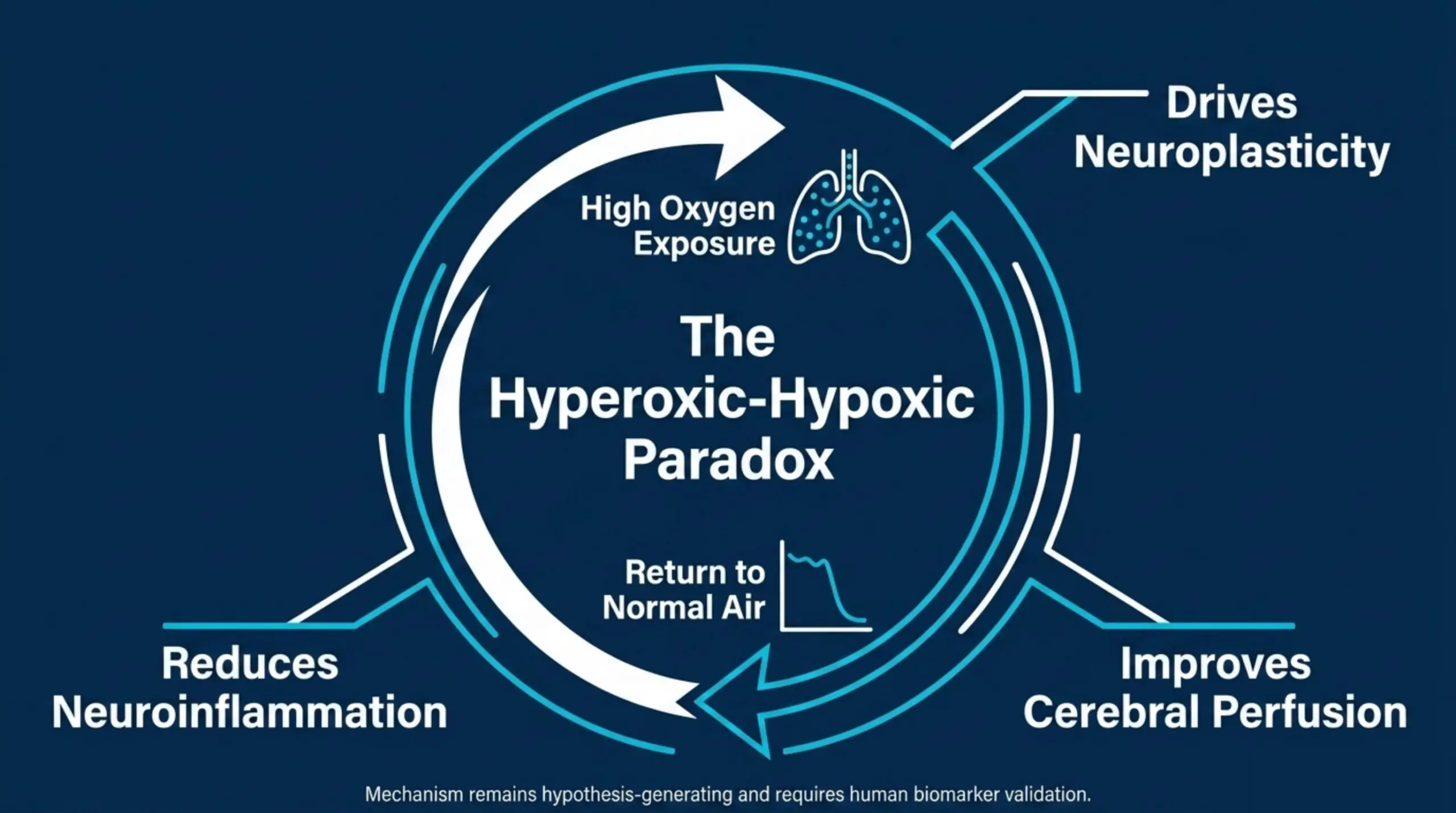
Doenyas-Barak et al. extend this rationale specifically to sleep. They describe the hyperoxic-hypoxic paradox, in which cyclical exposure to elevated then ambient oxygen tension drives neuroplasticity, improves cerebral perfusion, supports mitochondrial function, and reduces neuroinflammation. Duong-Quy et al. add a respiratory-specific layer, arguing that HBOT may modulate sleep physiology by reducing inflammation and oxidative stress, reversing tissue hypoxia, improving pulmonary function, modulating arousal threshold and loop gain, and influencing brain regions involved in sleep regulation. None of these mechanisms have been validated by sleep-specific biomarker studies in humans, and the authors of both publications are explicit that their mechanistic frameworks remain hypothesis-generating rather than confirmed.
What did the 2026 network meta-analysis of post-TBI sleep treatments find?
Wang et al. 2026 (J Head Trauma Rehabil) (PubMed) conducted a network meta-analysis of pharmacological and non-pharmacological interventions for traumatic brain injury related sleep disorders. The search captured 22 RCTs and 1299 patients. The analysis found that non-pharmacological treatments, including cognitive behavioural therapy, acupuncture, transcranial direct current stimulation, branched-chain amino acids, and HBOT, all produced statistically significant improvements in sleep outcomes compared with control. HBOT was one of five non-pharmacologic interventions that produced significant improvement in the Pittsburgh Sleep Quality Index, supported by a single included RCT. Pharmacotherapy did not demonstrate superior efficacy in the network. CBT was the most consistently effective intervention across PSQI, ISI, and ESS outcomes, supported by four RCTs.
For researchers, two methodological points matter. First, the network is sparse: most interventions, including HBOT, are anchored to one or two trials, which limits the precision of pairwise comparisons. Second, the heterogeneity in intervention protocols across the included trials is high. Wang et al. conclude that non-pharmacological treatments should be considered preferentially over pharmacotherapy, but the relative ranking among non-pharmacological options should not be over-interpreted from this single network.
How does HBOT compare to CBT for sleep after traumatic brain injury?
Loong et al. 2026 (Brain Impair) (PubMed) evaluated four named non-pharmacologic therapies for post-TBI sleep disturbances: cognitive behavioural therapy (including CBT-I), HBOT, blue-wavelength light therapy, and repetitive transcranial magnetic stimulation. The review explicitly attended to both statistical significance and minimally clinically important differences. The search was registered with PROSPERO and updated in March 2026. Twelve RCTs met inclusion criteria across the four interventions.
The strongest signal in the Loong review was for CBT, with significant improvements on the PSQI (mean difference -3.44), ISI at 6 to 8 weeks (-2.23) and 12 to 16 weeks (-0.91), and the Epworth Sleepiness Scale (-1.45). The authors graded their findings against published MCIDs and reported that only the change in PSQI reached the MCID threshold. HBOT, blue-wavelength light therapy, and rTMS were evaluated separately under the same GRADE framework. The Loong review does not report a head-to-head pairwise comparison of HBOT against CBT, because no included RCT randomised participants between those two interventions. This is the central methodological limitation researchers should note: in the current literature, the comparative efficacy claim of HBOT vs CBT for post-TBI insomnia cannot be answered.
How effective is HBOT for sleep quality across aging, long COVID, and PTSD?
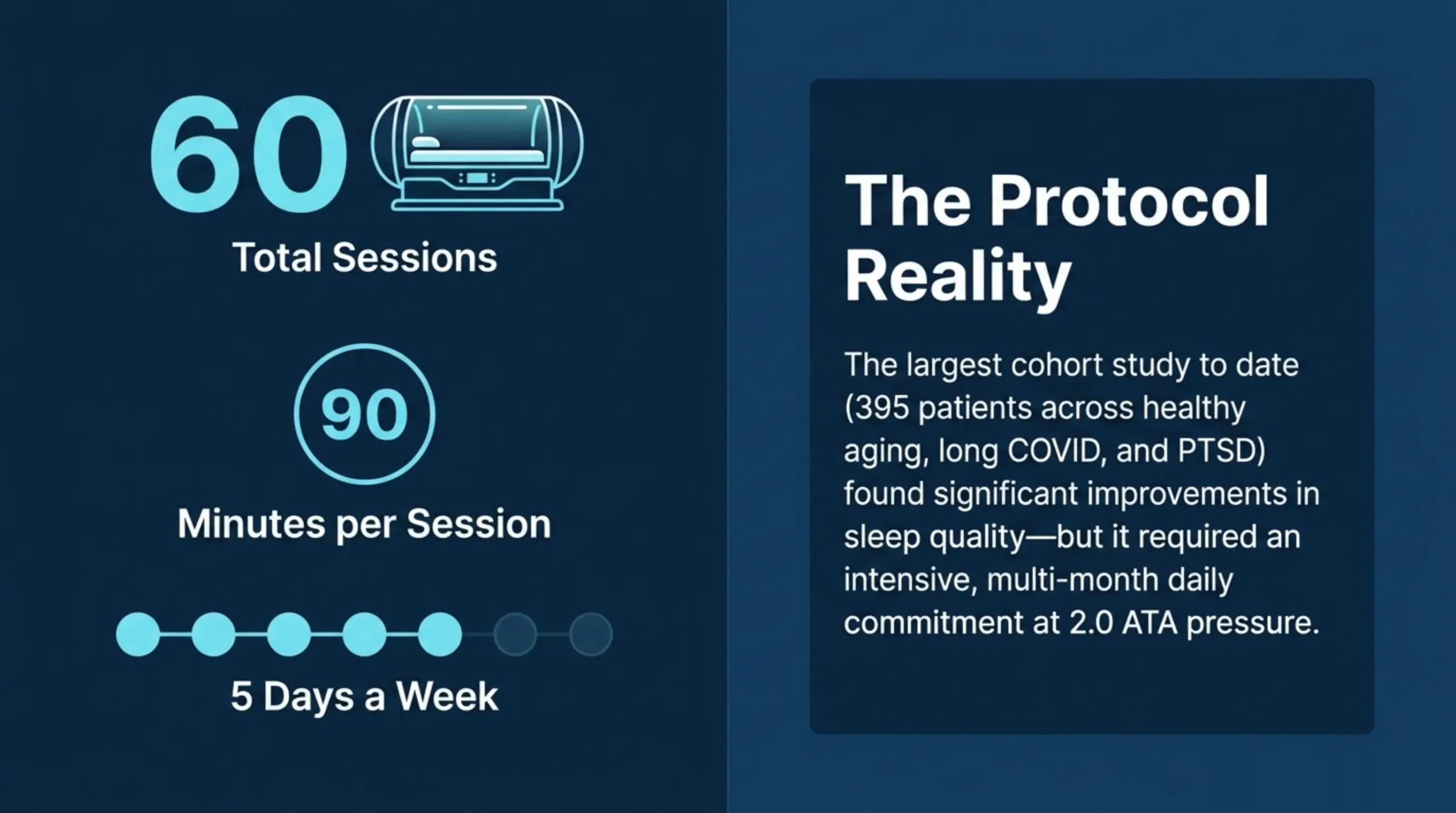
Doenyas-Barak et al. 2026 (Front Neurol) (PubMed) reported the largest single cohort to date evaluating HBOT for sleep quality outside the TBI literature. Their retrospective longitudinal analysis included 395 patients across three diagnostic groups: healthy aging (n=180), long COVID (n=92), and PTSD (n=123). All participants underwent the same protocol: 60 HBOT sessions at 2.0 ATA on 100 percent oxygen, 90 minutes per session, five days per week. Pre and post Pittsburgh Sleep Quality Index scores were compared with paired t-tests, and component scores were analysed with Wilcoxon signed-rank tests.
Across all three groups, total PSQI scores improved significantly post-treatment (p < 0.001), with Cohen’s d ranging from 0.37 to 0.91. PTSD patients had the highest baseline PSQI burden. Subjective sleep quality, sleep latency, and sleep disturbances improved in all three groups; daytime dysfunction improved in the aging and long COVID groups but not in the PTSD group. Medication use was unchanged across the cohort. Regression analysis identified baseline PSQI as a strong predictor of improvement, which the authors interpret as evidence that patients with worse baseline sleep have the largest absolute gains.
For Canadian clinical investigators, two features of this dataset are notable. First, the protocol (60 sessions, 2.0 ATA, 100 percent oxygen, 90 minutes, five days per week) matches dose ranges used in several Canadian academic and private hyperbaric programmes and could plausibly be replicated. Second, the use of PSQI as a primary endpoint is consistent with the sleep medicine literature and enables direct comparison with future Canadian cohorts. The principal limitations the authors acknowledge are the retrospective design and the absence of a sham or no-treatment control.
What does the 2026 evidence show for HBOT in sleep breathing disorders?
Duong-Quy et al. 2026 (Pulm Ther) (PubMed) published a systematic review focused on HBOT for sleep breathing disorders, which the authors define as obstructive sleep apnea, central sleep apnea, and high-altitude-related sleep breathing disturbances. The review synthesises emerging evidence on HBOT effects on sleep architecture and efficiency, framed by the physiological observation that sleep is highly sensitive to oxygen homeostasis.
The authors describe several plausible mechanisms by which HBOT could modulate sleep breathing physiology, including reduction of inflammation and oxidative stress, reversal of tissue hypoxia, improvement of pulmonary function and oxygenation, enhancement of neurocognitive function, modulation of arousal threshold and loop gain, and influence on brain regions involved in sleep regulation. The review concludes that current studies offer promising but preliminary evidence supporting HBOT’s role in selected sleep-breathing-disorder populations. It also identifies heterogeneity in protocols, small sample sizes, and limited long-term follow-up as the principal constraints on interpretation, and the authors call for future multicentre trials focused on protocol optimisation.
For sleep medicine researchers, this review does not establish HBOT as a treatment for OSA. It outlines the rationale and synthesises what little controlled data exists. Continuous positive airway pressure remains the standard of care. The question Duong-Quy et al. open is whether HBOT might play an adjunctive role in CPAP-intolerant patients or in selected phenotypes, which is a defensible focus for future Canadian trial design.
What are the methodological limitations of the current sleep and HBOT literature?
Four limitations recur across the 2026 publications and constrain the strength of any current clinical recommendation:
- Single-trial anchoring. In the Wang 2026 network, HBOT contributes one RCT. In the Loong 2026 review, HBOT is evaluated against pooled outcomes but without a head-to-head against CBT. Single-trial estimates are highly sensitive to outlier results and replication failures.
- Protocol heterogeneity. Pressure (1.5 to 2.5 ATA), session count (20 to 60), session length, and frequency vary widely across included trials. A dose-response analysis specifically for sleep endpoints has not been published.
- Endpoint heterogeneity. PSQI, ISI, ESS, actigraphy, and polysomnography are not interchangeable. Most current evidence is anchored to PSQI, which is patient-reported and subject to expectancy effects in unblinded trials.
- Sham control scarcity. The Doenyas-Barak cohort, the largest dataset to date, is uncontrolled. Sham HBOT designs are methodologically demanding but feasible, and only a small minority of the underlying RCT corpus uses them.
Where should Canadian sleep and hyperbaric researchers focus next?
Canada has both the academic sleep medicine capacity and the hyperbaric programme density to contribute meaningfully to this evidence base. The Canadian Undersea and Hyperbaric Medical Association (CUHMA) provides a national professional infrastructure for protocol harmonisation, and Health Canada regulates the chambers and conditions of use that any clinical trial would operate within. Four research priorities follow directly from the 2026 evidence:
- A head-to-head HBOT vs CBT-I RCT for post-concussion or mild TBI insomnia. Loong et al. 2026 identified this as the largest gap in the post-TBI literature. A pragmatic trial design with a non-inferiority endpoint would be informative.
- A multicentre prospective HBOT cohort for long COVID sleep disturbance. Doenyas-Barak’s signal for long COVID sleep is among the strongest in the 2026 cohort. A Canadian replication using the same PSQI primary endpoint would meaningfully extend the evidence base.
- A pilot sham-controlled HBOT trial for CPAP-intolerant moderate OSA. Duong-Quy et al. 2026 explicitly frame this population as a defensible target for early trial work.
- A standardised reporting checklist for HBOT sleep trials. A CUHMA-led consensus on pressure, sessions, frequency, and minimum endpoint reporting would reduce future heterogeneity and improve trial pooling.
Investigators planning a Canadian study should review the regulatory framework that applies to HBOT chambers. Health Canada classifies hyperbaric chambers as medical devices and requires licensing for clinical use. The Undersea and Hyperbaric Medical Society publishes the international clinical indications most commonly referenced in Canadian protocols. Canada Hyperbarics maintains a directory of hospitals and regulated facilities across the country, several of which already deliver HBOT under protocols compatible with the trial designs above.
Frequently asked research questions
Does HBOT improve sleep quality in randomised trials?
In the 2026 network meta-analysis by Wang et al., HBOT was one of five non-pharmacologic interventions that produced statistically significant improvements in the Pittsburgh Sleep Quality Index for post-TBI sleep disorders. The HBOT estimate is supported by one included randomised controlled trial, so confidence in the effect size is limited.
Is HBOT better than CBT for insomnia?
The current literature cannot answer this question. No published RCT randomises post-TBI or general adult insomnia patients between HBOT and CBT-I in a head-to-head design. Loong et al. 2026 found CBT to be the most consistently effective intervention for post-TBI sleep, but their review did not include a direct HBOT-versus-CBT comparison trial.
What HBOT protocol has been most studied for sleep outcomes?
The largest single dataset, Doenyas-Barak et al. 2026, used 60 sessions at 2.0 atmospheres absolute on 100 percent oxygen, 90 minutes per session, five days per week. Other included trials in the systematic reviews used pressures between 1.5 and 2.5 ATA and session counts between 20 and 60. Protocol heterogeneity is a recurring theme in the current literature.
Does HBOT treat obstructive sleep apnea?
HBOT is not an established treatment for obstructive sleep apnea. Continuous positive airway pressure remains the standard of care. Duong-Quy et al. 2026 review the rationale for HBOT in sleep breathing disorders and characterise the available evidence as promising but preliminary, with heterogeneity in protocols, small sample sizes, and limited long-term follow-up.
Is HBOT for sleep disturbances approved in Canada?
Sleep disturbance is not among the conditions for which HBOT has Health Canada approval. The studies summarised in this review describe HBOT use in research and selected clinical contexts, not recognised indications. Researchers planning Canadian trials should engage Health Canada early on the regulatory pathway for off-label investigation.
Where can I find Canadian hyperbaric programmes for collaboration?
Canada Hyperbarics maintains a directory of Canadian hospitals and regulated facilities that deliver HBOT. The directory lists hospital-based programmes and private facilities by province and includes pressure capabilities relevant to research protocol selection.
Conclusion and next steps for researchers
The 2026 evidence base for HBOT in sleep disturbances has matured from scattered single studies to four substantive publications that frame the field. The within-subject effect on PSQI is reproducible across populations; the comparative effect against CBT-I is unanswered; the mechanism is plausible but not biomarker-validated; and the sleep-breathing-disorder evidence remains hypothesis-generating. Canada is well positioned, through CUHMA, Health Canada regulatory infrastructure, and an established hyperbaric programme footprint, to lead the confirmatory trial work the current evidence base calls for. The complete Canadian HBOT research database tracks every new study as it is published. Researchers and clinicians can also browse our conditions index to see how the sleep evidence is contextualised against other HBOT indications.
This content is for informational purposes only and does not constitute medical advice. The studies discussed describe research findings and do not establish HBOT as a treatment for sleep disturbances outside of clinical research contexts. Patients with sleep concerns should consult a licensed physician.