
TL;DR: Middle ear barotrauma is the most common side effect of hyperbaric oxygen therapy, and most cases are preventable with good operator protocols. The strongest prevention levers a Canadian clinic can control are careful pre-treatment ear screening, teaching every patient to equalise before pressure rises, slowing compression for at-risk patients, and stopping descent the moment a patient reports ear pain. This guide sets out a step-by-step protocol for clinic owners and operators.
In hyperbaric oxygen therapy, middle ear barotrauma (MEB) is a pressure-related injury to the middle ear that happens when the air space behind the eardrum cannot equalise quickly enough as chamber pressure rises. It is the single most frequently reported complication of hyperbaric oxygen therapy (HBOT), and for a Canadian clinic it is the adverse event most likely to interrupt a treatment course, cause patient distress, or lead to a missed session. The good news for operators is that MEB is largely a process problem: with the right screening, patient coaching, and compression protocol, the great majority of cases can be prevented or kept mild.
This guide is written for hyperbaric clinic owners and operators in Canada who want a practical, evidence-informed protocol to lower their MEB rate. Canada Hyperbarics is an information resource, and the protocol below draws on recent peer-reviewed research. It is operational guidance, not a substitute for your medical director’s clinical judgement or your facility’s accreditation standards.
How common is middle ear barotrauma in hyperbaric oxygen therapy?
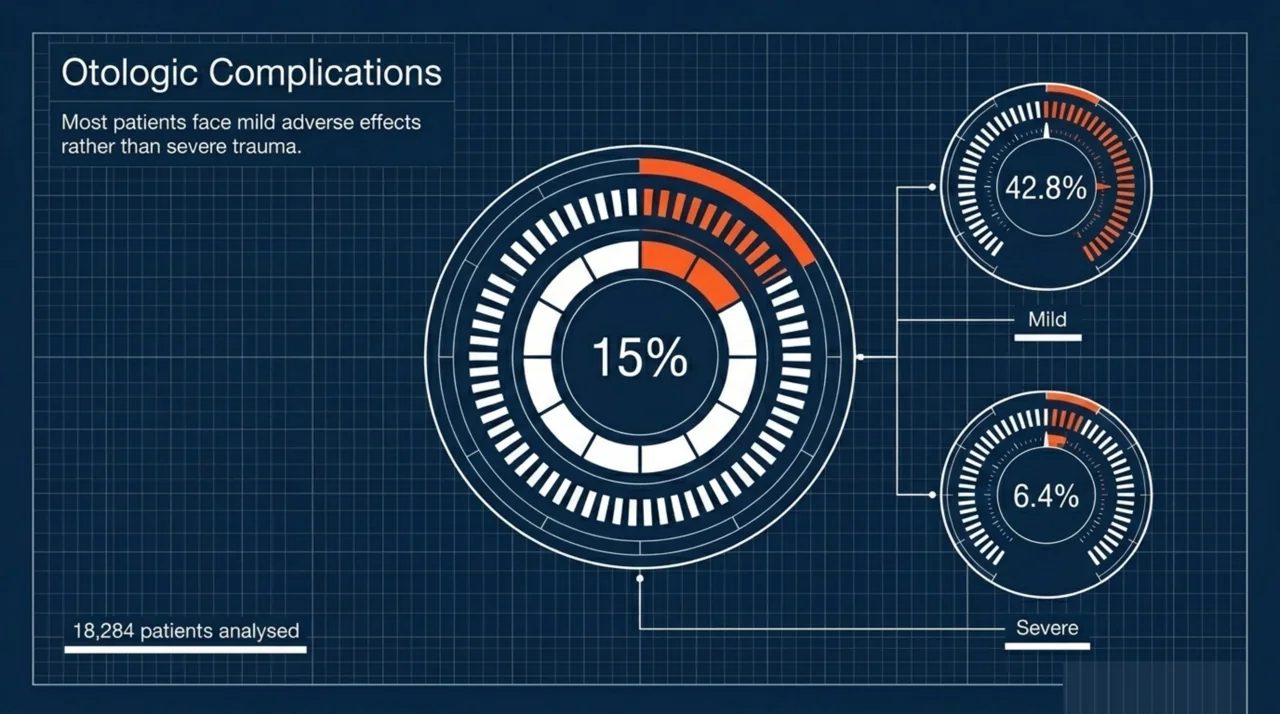
Otologic problems are common enough that every operator should plan for them. A 2025 systematic review of otologic adverse events in HBOT (Voigt et al., PubMed | Our Assessment) pooled 54 studies covering 18,284 patients and found that 15% experienced otologic complications. Reassuringly, of the middle ear barotrauma that occurred, the review reported that 42.8% of cases were mild and only 6.4% were severe. In other words, MEB is frequent but usually low-grade when it is caught and managed early.
Provider-reported data point the same way. A 2024 Undersea and Hyperbaric Medical Society survey of 265 members (Laspro et al., PubMed | Our Assessment) found barotrauma was among the most commonly reported adverse effects at 14.9%, behind myopia at 24.4% and ahead of confinement anxiety at 11.5%. The same survey reported that 2.4 ATA was the most commonly chosen treatment pressure at 35.2%. For a busy clinic, these figures translate into a steady trickle of ear complaints that a protocol must be ready to handle.
Which patients are most at risk of ear barotrauma?
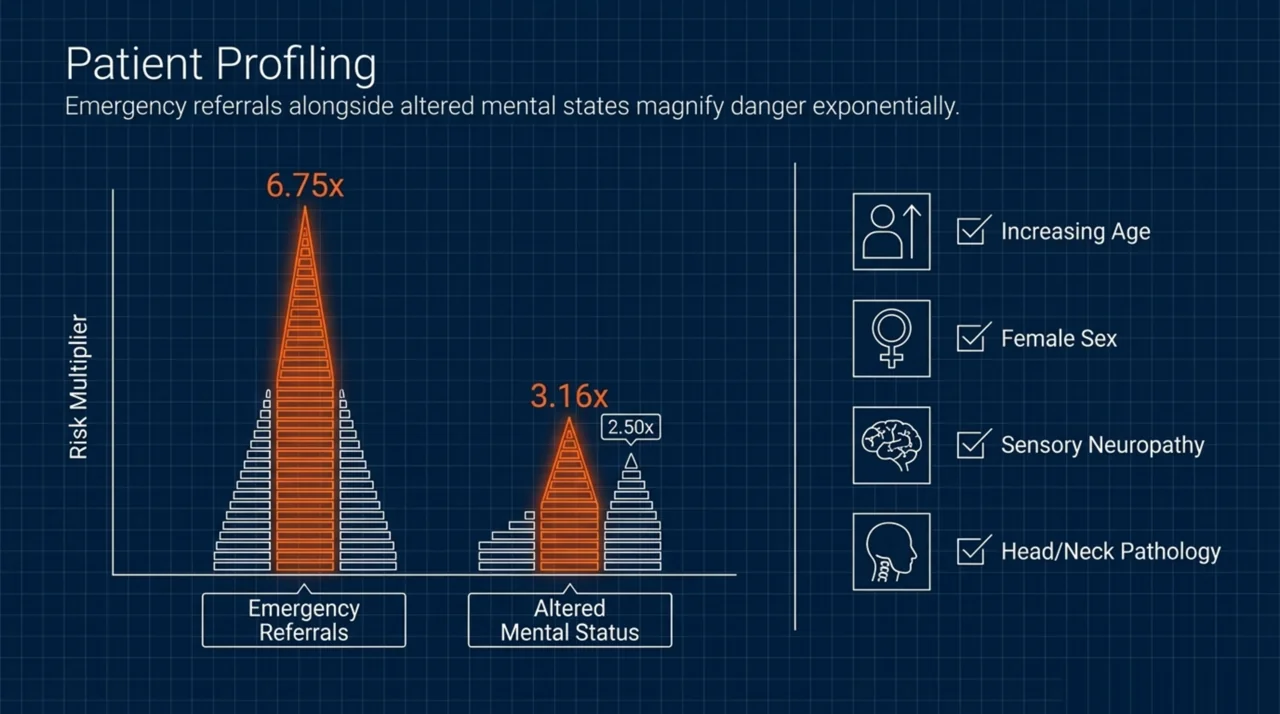
Knowing who is at risk lets you target extra coaching and slower compression where it matters. The Voigt systematic review reported that the major risk factors associated with otologic complications were increasing age, female sex, head and neck pathology, sensory neuropathy, and pre-treatment difficulty equalising ear pressure. Crucially, the main protective factor it identified was experience with effective equalisation techniques, which is something your staff can directly teach.
Patients who cannot actively equalise are a special concern. A 2025 retrospective cohort of patients treated with monoplace HBOT for carbon monoxide poisoning (Lee et al., PubMed | Our Assessment) found that altered mental status at presentation was associated with roughly three times the odds of MEB (odds ratio 3.16). Higher serum albumin and magnesium levels were associated with lower risk. Because this was an observational study, these are associations rather than proven causes, but the practical message is clear: an obtunded or confused patient cannot equalise on their own and needs special handling.
A separate 2025 single-centre study of 296 monoplace HBOT patients (Lee et al., PubMed | Our Assessment) reached a consistent conclusion: altered mental state was associated with increased odds of MEB (odds ratio 2.50), and patients in the emergency-treatment group were 6.75 times more likely to experience MEB than elective patients. Emergency and unconscious patients deserve the slowest, most closely monitored compression your protocol allows.
What is the step-by-step protocol to prevent middle ear barotrauma?
The following sequence builds prevention into every stage of a treatment, from intake to descent. Adapt the specifics to your chamber type and your medical director’s direction.
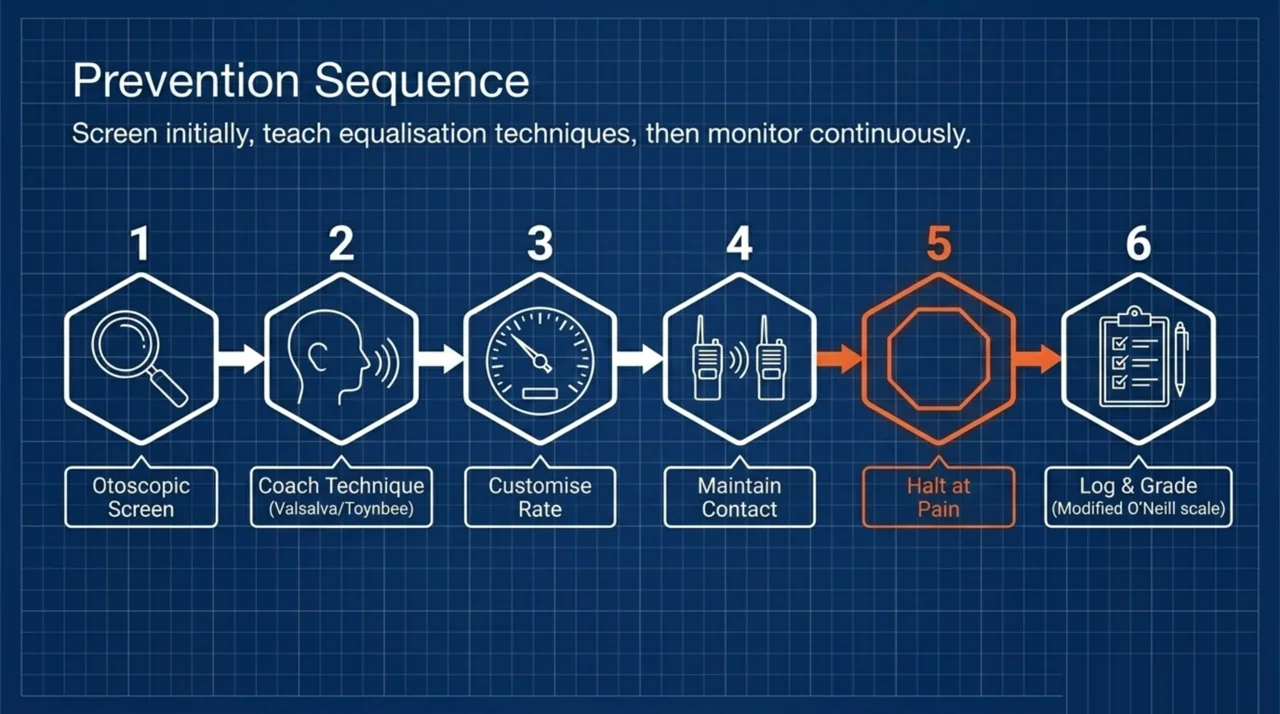
- Screen the ears before the first session. Document a baseline otoscopic examination and ask about recent upper respiratory infection, allergies, nasal congestion, prior ear surgery, and any history of difficulty equalising on flights or while diving. A 2025 multicentre study of HBOT in patients aged 75 and older (Cracchiolo et al., PubMed | Our Assessment) reported that side effects occurred in 20.3% of patients, primarily middle ear barotrauma at 8.7% and sinus barotrauma at 4.3%, and the authors credited meticulous pre-treatment ENT evaluation with minimising risk.
- Teach equalisation before anyone enters the chamber. Show every patient how to clear their ears using gentle swallowing, yawning, jaw movement, and the Valsalva or Toynbee manoeuvres. Have them demonstrate a successful clear in front of staff. Because experience with equalisation is a protective factor, this short lesson is one of the highest-value steps you can standardise.
- Slow the compression rate for at-risk patients. Ear injury happens during descent, when pressure rises. For patients flagged at intake, for elderly patients, and for anyone who struggles to equalise, compress more slowly and pause as needed so the patient can catch up.
- Keep continuous contact during descent. Maintain two-way communication and instruct patients to equalise early and often, before they feel fullness rather than after. Establish a simple signal for ear discomfort that works even with a hood or mask in place.
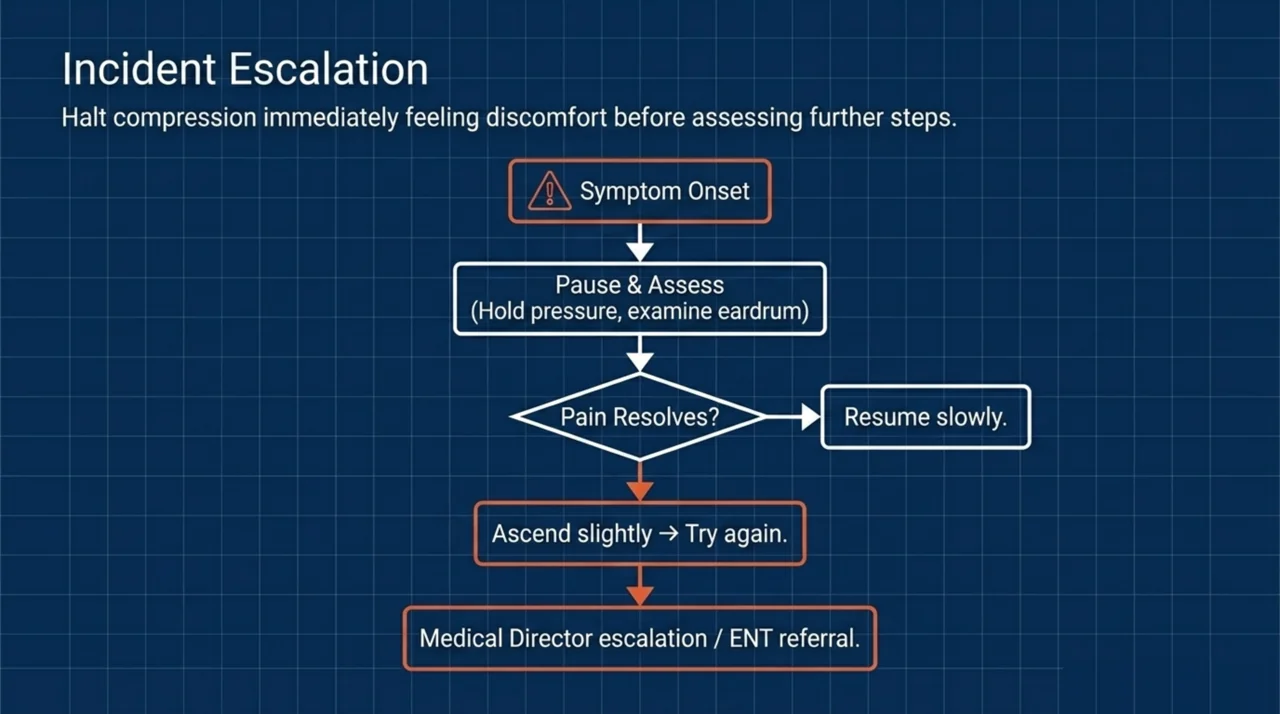
- Stop descent at the first report of pain. Pain means the ear is not equalising. Hold pressure, coach the patient to clear, and only continue once the discomfort resolves. If it does not resolve, ascend slightly and try again. Never push a patient through ear pain to stay on schedule.
- Have a plan for patients who cannot equalise. Confused, sedated, intubated, or unconscious patients cannot clear their own ears. Your medical director should pre-define an escalation pathway, which may include physician-performed manoeuvres or referral for myringotomy or pressure-equalisation tubes before treatment in selected cases.
- Document and grade every event. Record each ear complaint, examine the eardrum after the session, and grade severity consistently. Recent research has used structured scales such as the modified O’Neill grading system to standardise this assessment, as in the Lee carbon monoxide cohort above. Consistent grading lets you track your clinic’s MEB rate over time and spot problem patterns.
Do decongestants prevent ear barotrauma during HBOT?
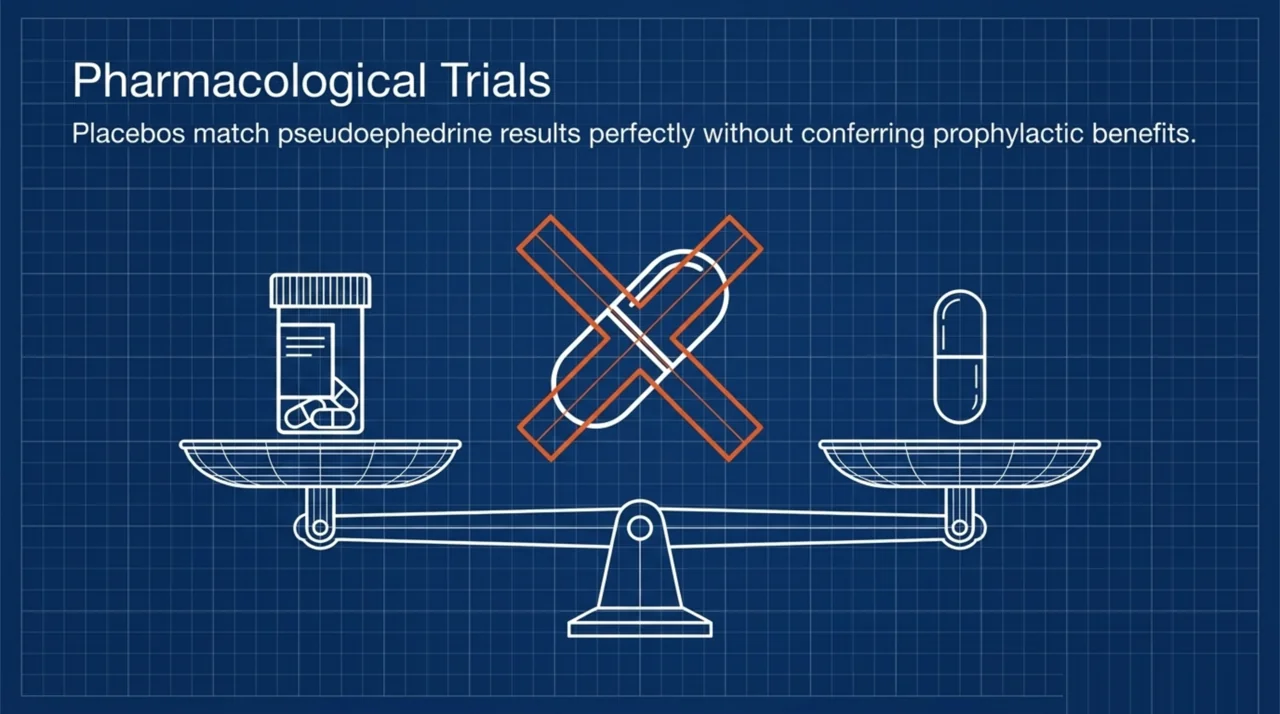
This is a common operator question, and the best recent evidence says do not rely on them. A 2025 randomised, double-blind, placebo-controlled trial (Moayedi et al., PubMed | Our Assessment) tested pseudoephedrine given before a first HBOT treatment and found no statistically significant difference between the pseudoephedrine and placebo groups in ear pain ratings, tympanic membrane injury, or the need for rescue medication. Because this was a randomised controlled trial, it is reasonable to conclude that routine pseudoephedrine prophylaxis did not prevent MEB in this setting. The takeaway for clinics is that good equalisation technique and a careful compression protocol matter far more than a pre-treatment pill.
How should clinics protect staff and inside attendants?
Your protocol should cover the people who work inside multiplace chambers, not just patients. Inside attendants are exposed to the same pressure changes as patients while breathing compressed air. A 2025 longitudinal study of inside attendant personnel (Avci et al., PubMed | Our Assessment) followed 15 attendants across 2,446 sessions and found no clinically significant hearing loss over time, with only three attendants experiencing mild middle ear barotrauma. The authors concluded that with proper precautions the risks are manageable. For owners, that means including attendant ear screening, equalisation training, and audiometry in your occupational health program.
Why does a written barotrauma protocol matter for accreditation?
Barotrauma is a recognised, expected risk of hyperbaric medicine, and accrediting bodies expect facilities to manage it deliberately. A 2024 review of safety in hyperbaric medicine (Mago, PubMed | Our Assessment) lists barotrauma among the core complications of the therapy and emphasises that safety protocols and preventive measures are central to delivering it responsibly. A documented MEB prevention and management protocol, with staff training records and event logging, demonstrates exactly the kind of structured safety culture that the Undersea and Hyperbaric Medical Society accreditation framework and Canadian peers at the Canadian Undersea and Hyperbaric Medicine Association promote. You can review how accredited and hospital-based programs operate through our directory of Canadian hospitals and regulated facilities.
Monoplace versus multiplace: how does chamber type change your protocol?
The prevention principles are the same, but the operator’s tools differ by chamber type. The table below summarises the practical differences for MEB management.
| Factor | Monoplace chamber | Multiplace chamber |
|---|---|---|
| Hands-on help during descent | Not possible inside; coaching is by intercom only | Inside attendant can assist and coach directly |
| Compression control | Operator controls rate from outside; pause for equalisation | Operator controls rate; attendant relays patient status |
| Higher-risk patients | Altered-mental-status and emergency patients need extra caution (see Lee cohorts) | Attendant presence aids monitoring of vulnerable patients |
| Staff exposure | No inside staff exposure | Attendants require ear screening and audiometry |
How should clinics manage a barotrauma event once it happens?
- Pause and assess. Stop changing pressure, examine the eardrum, and grade the injury using your standard scale.
- Treat symptoms. Most mild cases settle with decongestants, analgesia as directed by your physician, and time. The systematic review evidence suggests most MEB is mild and self-limiting.
- Decide on continuation. Your medical director determines whether to resume the course, slow future compressions, or pause treatment until the ear heals.
- Refer when needed. Severe or non-resolving cases, persistent perforation, or hearing change warrant ear, nose, and throat referral.
- Log the event. Add it to your adverse-event register so trends inform protocol updates and accreditation review.
Frequently asked questions about middle ear barotrauma in HBOT
What is middle ear barotrauma?
Middle ear barotrauma is pressure-related injury to the middle ear that occurs when the air space behind the eardrum cannot equalise as ambient pressure rises during chamber compression. It can range from mild ear fullness and redness to, rarely, eardrum perforation.
How common is it during hyperbaric oxygen therapy?
A 2025 systematic review of 18,284 patients reported that 15% experienced otologic complications, and of the middle ear barotrauma cases, 42.8% were mild and 6.4% were severe. It is the most frequently encountered ear complication in HBOT.
Can it be prevented?
Most cases can be prevented or kept mild. Pre-treatment ear screening, teaching effective equalisation, slowing compression for at-risk patients, and stopping descent at the first sign of pain are the core prevention steps. Experience with effective equalisation technique is a recognised protective factor.
Do decongestants like pseudoephedrine help?
A 2025 randomised controlled trial found that pseudoephedrine prophylaxis did not reduce ear pain, tympanic membrane injury, or the need for rescue medication compared with placebo. Clinics should prioritise technique and compression protocol over routine decongestant use.
Which patients need extra caution?
Patients with altered mental status, emergency referrals, older patients, those with head and neck pathology, and anyone with a history of difficulty equalising are at higher risk. Patients who cannot actively clear their ears need a pre-defined escalation plan from your medical director.
Does middle ear barotrauma affect staff too?
Inside attendants in multiplace chambers face the same pressure changes as patients. A 2025 study of 15 attendants over 2,446 sessions found no clinically significant hearing loss and only three mild MEB cases, supporting the value of ear screening and audiometry in an occupational health program.
Where can Canadian clinics learn more?
Building a strong safety culture starts with knowing how established programs operate. Explore our directory of Canadian hospitals and regulated facilities to see accredited and hospital-based hyperbaric centres, review our research library for the latest peer-reviewed evidence, and visit our FAQ for plain-language answers patients commonly ask. A documented, well-rehearsed middle ear barotrauma protocol protects your patients, your staff, and your clinic’s standing.
Medical disclaimer: This content is for informational purposes only and does not constitute medical advice. It is operational guidance for hyperbaric facilities and is not a substitute for the clinical judgement of a qualified hyperbaric physician or your facility’s accreditation standards. Always follow your medical director’s protocols and applicable Canadian regulations.