
TL;DR: Fournier’s gangrene is a rare, rapidly progressive necrotizing soft tissue infection of the perineum and genitals that is a surgical emergency. The two pillars of treatment are immediate, repeated surgical debridement and broad-spectrum antibiotics with resuscitation. Hyperbaric oxygen therapy (HBOT) is an adjunct, not a substitute for surgery, and a 2026 systematic review and meta-analysis associated it with lower mortality in Fournier’s gangrene. Necrotizing soft tissue infections are a UHMS-recognised HBOT indication. Refer early and in parallel with surgery, never instead of it. This guide from Canada Hyperbarics explains when and how to involve a hyperbaric centre.
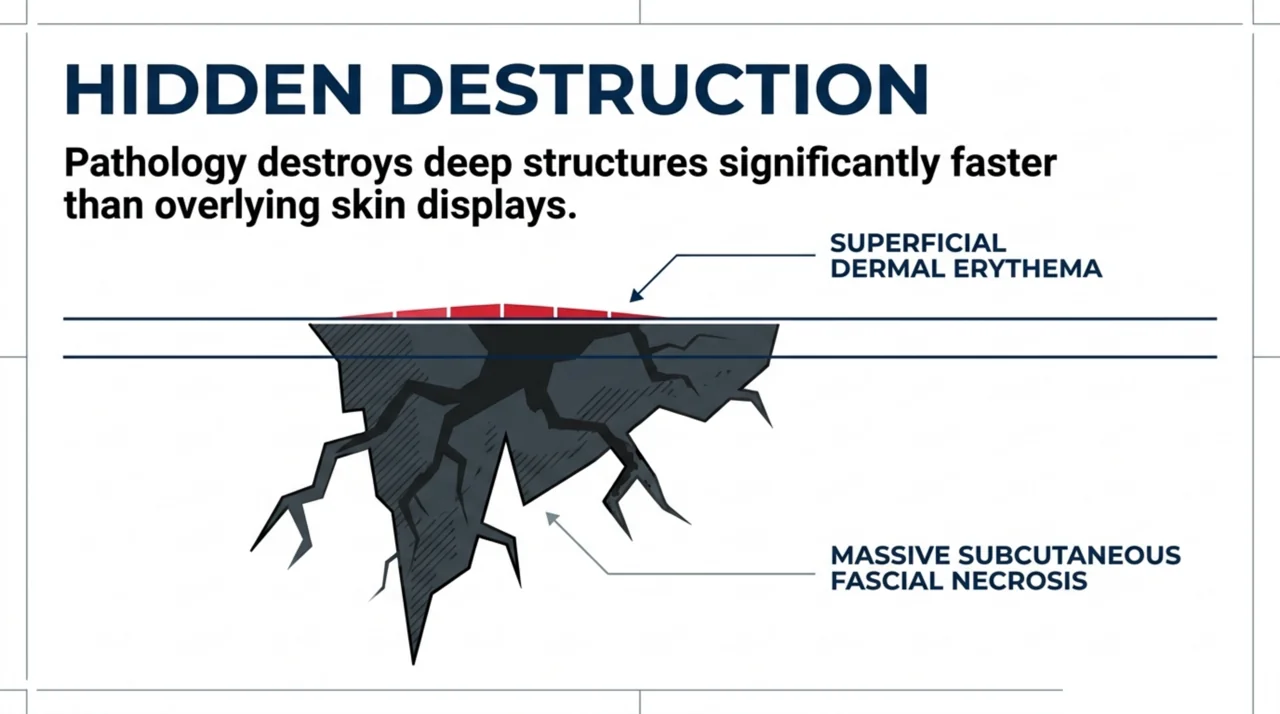
Fournier’s gangrene is a necrotizing soft tissue infection of the perineum, genitals, and perianal region that destroys fascia and subcutaneous tissue faster than the overlying skin reveals. For a referring physician, the single most important fact is that the diagnosis is a surgical emergency: outcomes hinge on how quickly the patient reaches the operating room for debridement and receives broad-spectrum antibiotics. Hyperbaric oxygen therapy for Fournier’s gangrene has a defined but supporting role, and the question this guide answers is a practical one – when should you refer, and how urgently?
Canada Hyperbarics is an independent, research-backed directory of Canadian hyperbaric medicine. This article is written for emergency physicians, urologists, general surgeons, and family physicians who may be the first to recognise this condition and who need to know where hyperbaric oxygen therapy fits in the treatment pathway.
What is Fournier’s gangrene, and why is it a surgical emergency?
Fournier’s gangrene is a form of necrotizing soft tissue infection (NSTI) that tracks along fascial planes of the genital, perineal, and perianal area. It is usually polymicrobial, combining aerobic and anaerobic organisms, and it progresses over hours rather than days. A 2026 systematic review and meta-analysis (Patel and colleagues, PubMed | Our Assessment) describes it as a rare, rapidly progressive infection that continues to carry a high mortality rate, which is why early recognition matters so much.
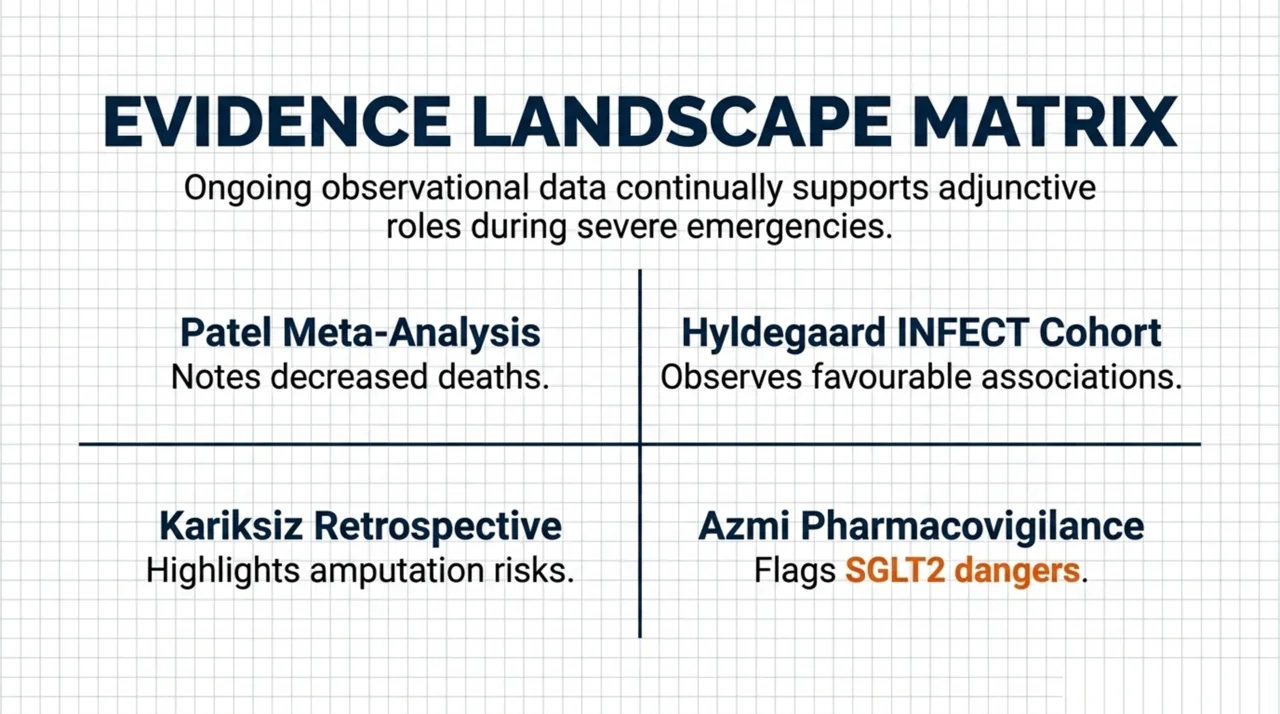
The clinical lesson from the broader NSTI literature is sobering. A 2025 retrospective study of 50 patients with lower-extremity necrotizing soft tissue infection (Kariksiz and colleagues, PubMed | Our Assessment) reported a mortality rate of 20 percent and an amputation rate of 60 percent. In that cohort, longer hospital and intensive-care stays were significantly associated with mortality, and diabetes was significantly associated with amputation. The authors used the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score as part of assessment, a reminder that the diagnosis is often delayed because early symptoms are non-specific.
The practical takeaway: pain out of proportion to physical findings, rapidly spreading swelling, crepitus, or systemic toxicity in the perineal or genital region should prompt urgent surgical consultation. You can review related conditions in the conditions index on Canada Hyperbarics.
How does hyperbaric oxygen therapy work as an adjunct in necrotizing infection?
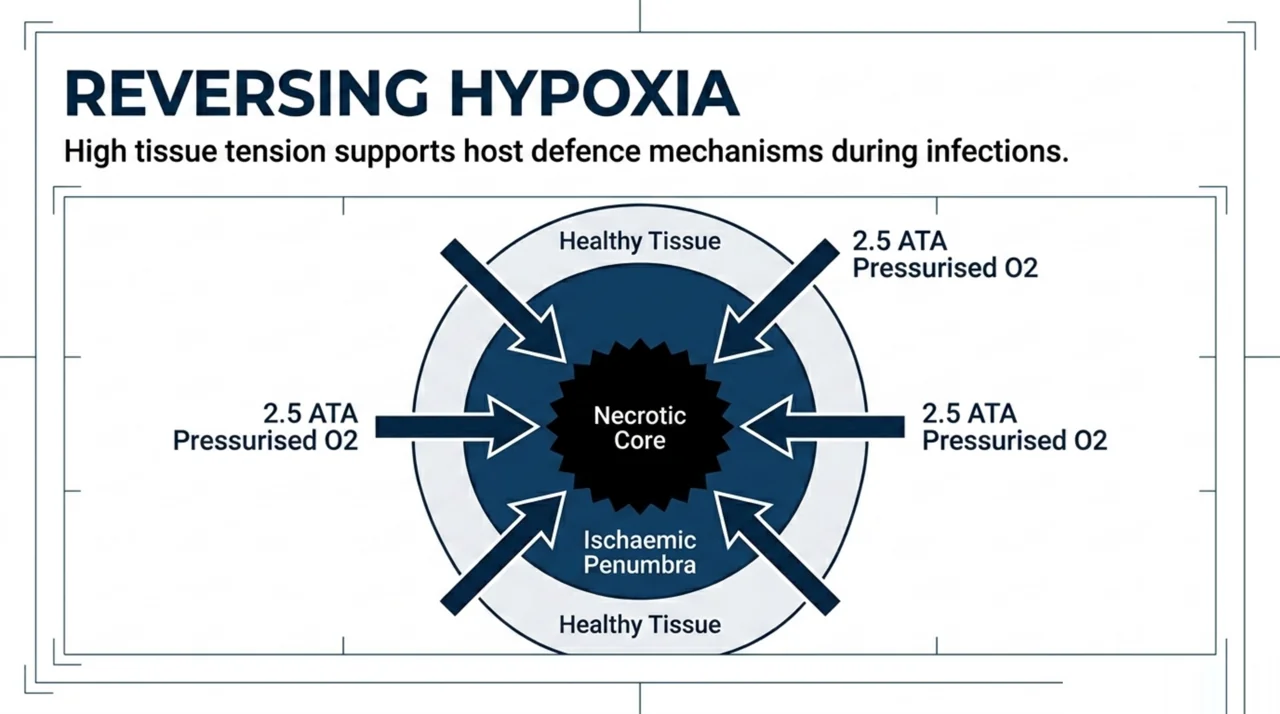
Hyperbaric oxygen therapy involves breathing near-100 percent oxygen at pressures above one atmosphere, typically around 2 to 2.5 atmospheres absolute. A 2026 review of HBOT in hypoxia-induced conditions (Bhargava and colleagues, PubMed | Our Assessment) notes that this raises oxygen levels in hypoxic and ischaemic tissues, that the effect is often dose-dependent, and that Fournier’s gangrene and chronic osteomyelitis are among the conditions in which HBOT is applied adjunctively. The same review situates HBOT within evidence-based protocols set by the Undersea and Hyperbaric Medical Society (UHMS) and the European Underwater and Baromedical Society.
The rationale in necrotizing infection is that infected, swollen tissue becomes profoundly hypoxic, which impairs the oxygen-dependent killing that neutrophils rely on and favours anaerobic organisms. Raising tissue oxygen tension is proposed to support host defence and tissue viability around the zone of surgical debridement. A 2026 narrative review of HBOT and immune function (Mei and colleagues, PubMed | Our Assessment) reports that HBOT modulates immune effector responses, while cautioning that treatment parameters and immune endpoints vary widely across studies. HBOT is an adjunct to surgery and antibiotics, never a replacement for them.
What does the latest evidence say about HBOT for Fournier’s gangrene?
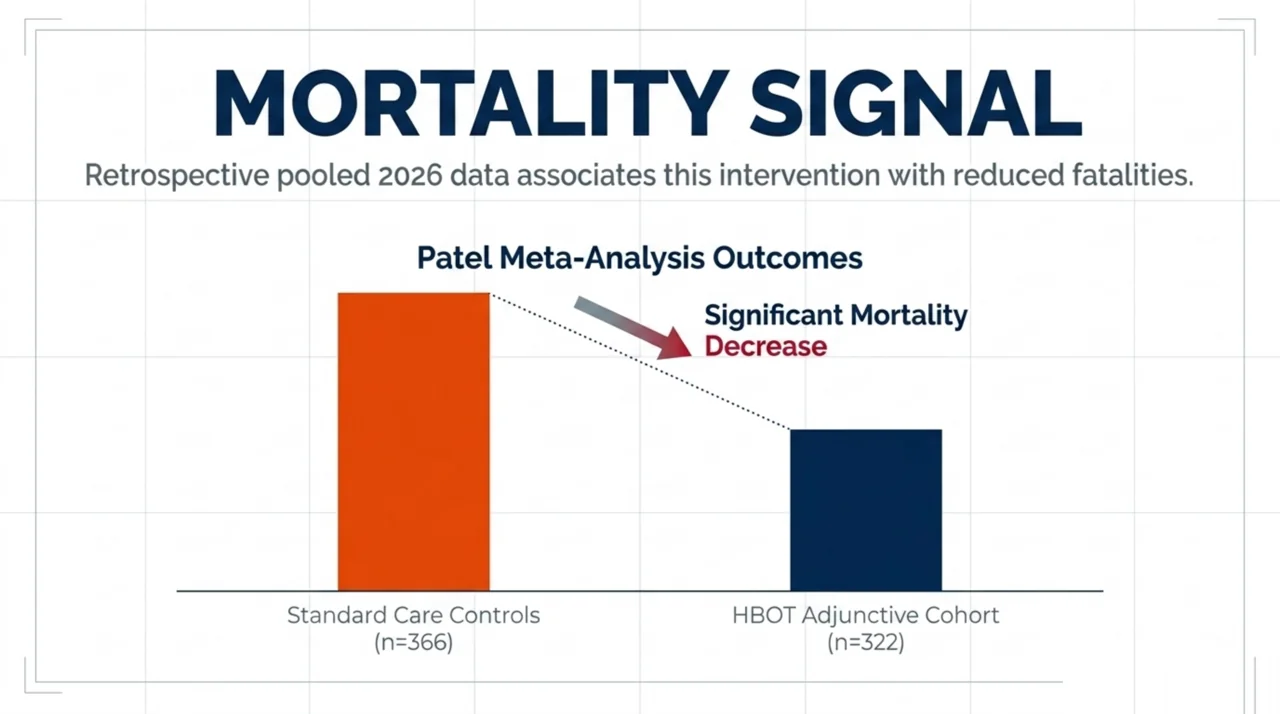
The most relevant recent evidence is the 2026 systematic review and meta-analysis by Patel and colleagues (PubMed | Our Assessment). It pooled thirteen retrospective studies comprising 322 patients treated with hyperbaric oxygen therapy and 366 controls. HBOT was associated with a significantly lower mortality rate compared with control groups. Because every included study was retrospective, this is an association rather than proof of causation, and the authors frame HBOT as a therapy that could be considered adjunctively rather than one that is definitively established.
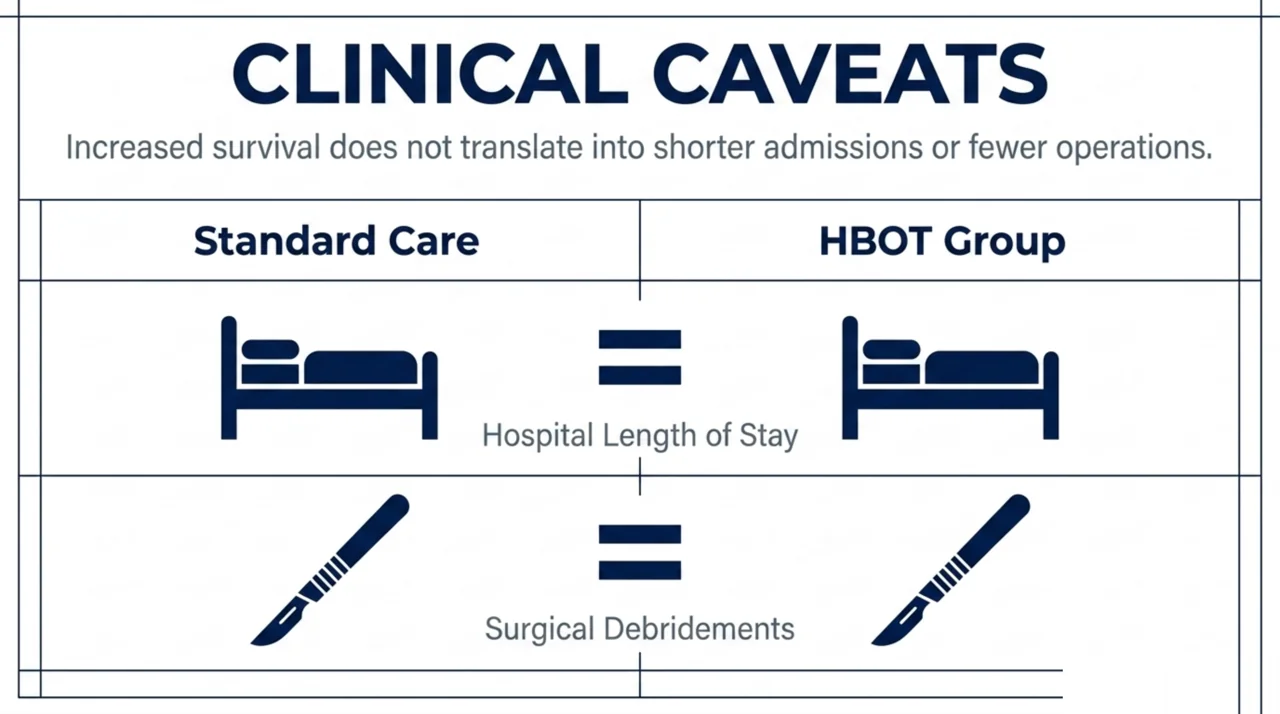
Two caveats are important when you counsel a patient or a colleague. First, the same meta-analysis found no statistically significant difference in hospital length of stay or in the number of surgical debridements between the HBOT and control groups, so the mortality signal did not translate into shorter admissions or fewer trips to the operating room. Second, retrospective designs are vulnerable to selection bias, because the patients chosen for HBOT may differ systematically from those who are not. The honest summary is that the observational evidence is encouraging on mortality but is not high-certainty, and no randomised controlled trial has settled the question.
What does the broader necrotizing soft tissue infection evidence show?
Because Fournier’s gangrene is a subtype of necrotizing soft tissue infection, the largest prospective dataset is informative. The Scandinavian INFECT study (Hyldegaard and colleagues, PubMed | Our Assessment) prospectively enrolled 409 consecutive NSTI patients across five centres in Denmark, Norway, and Sweden, of whom 329 received hyperbaric oxygen and 80 did not. The median time from arrival at a specialised hospital to the first hyperbaric oxygen treatment was 4.3 hours. The authors note that several observational studies have suggested an association between hyperbaric oxygen and improved survival, but that the evidence remains inconclusive and that the benefit may be largest in the most severely ill patients.
The INFECT investigators also flag a real-world referral constraint that Canadian physicians should anticipate: not every patient in that cohort could receive hyperbaric oxygen, because haemodynamic instability, chamber capability, and availability all affect access, which can introduce selection bias into the literature.
Gas-forming necrotizing infection can still be managed with HBOT as part of a multidisciplinary plan. In a 2024 case report of non-clostridial gas gangrene after an open pelvic fracture (Takeno and colleagues, PubMed | Our Assessment), the patient underwent three surgical debridements and antibiotics with adjunctive hyperbaric oxygen and was walking with a cane five months after injury.

Which patients should you refer for HBOT, and how urgently?
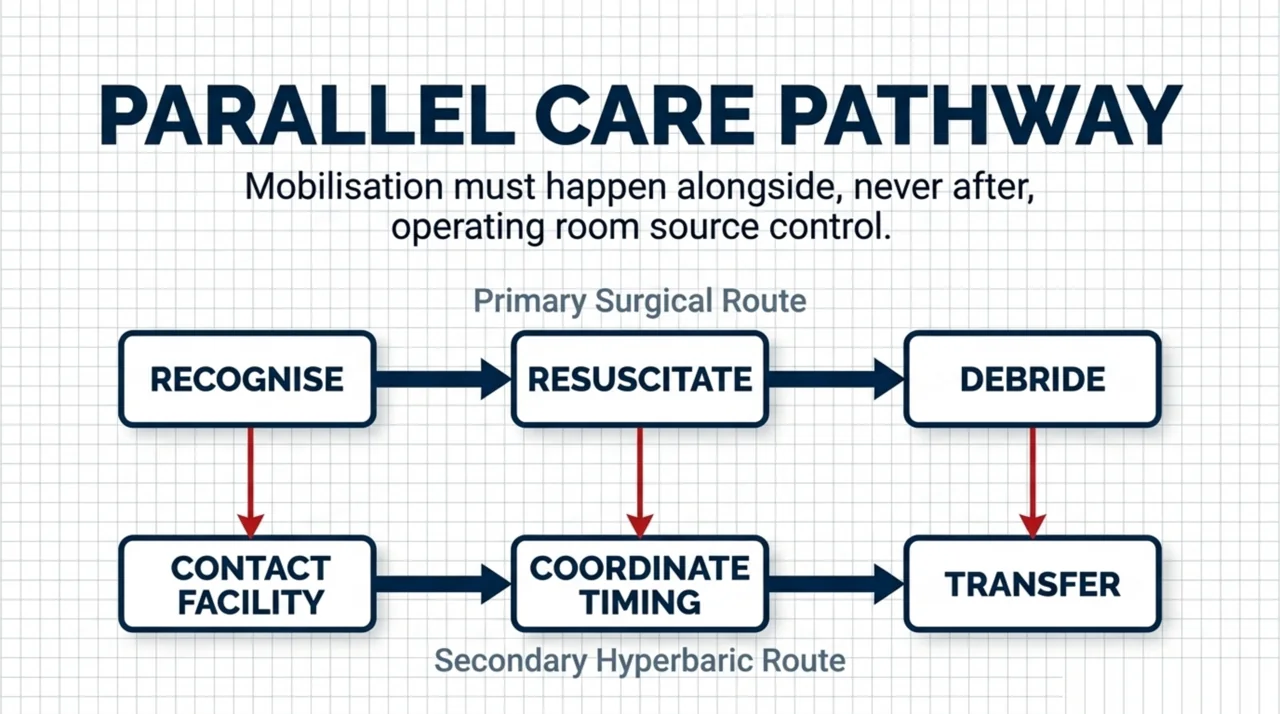
The referral principle is simple: hyperbaric oxygen runs in parallel with surgery, not instead of it, and surgical debridement always comes first. A patient with suspected Fournier’s gangrene needs immediate surgical and infectious-disease involvement, source control in the operating room, broad-spectrum antibiotics, and resuscitation. Hyperbaric referral should happen alongside that workup so the patient can begin treatment quickly once stabilised, mirroring the median 4.3-hour arrival-to-treatment window seen in the INFECT cohort.
- Recognise and resuscitate. Treat suspected Fournier’s gangrene as a surgical emergency and arrange urgent surgical consultation rather than waiting for imaging to confirm.
- Achieve source control. Debridement and antibiotics are the established, non-negotiable foundation of care. HBOT does not replace either.
- Contact a hyperbaric centre early. Ask whether the receiving hospital has, or can transfer to, a facility that treats NSTI, because chamber availability and the ability to manage a critically ill patient vary by site.
- Coordinate timing. Hyperbaric treatment is most practical once the patient is haemodynamically stable enough for the chamber and surgical source control is underway.
To find hospitals and regulated facilities that offer hyperbaric oxygen therapy in your region, see the Canada Hyperbarics directory of facilities, and review province-by-province access on the coverage guide. Necrotizing soft tissue infection is one of the indications on the UHMS hyperbaric oxygen indications list, and Canadian practice guidance is supported by the Canadian Undersea and Hyperbaric Medical Association (CUHMA).
What risk factors and red flags should prompt earlier suspicion?
Diabetes is the most consistent risk factor across the necrotizing infection literature, and in the lower-extremity NSTI cohort it was significantly associated with amputation. A newer signal concerns sodium-glucose cotransporter-2 (SGLT2) inhibitors. A 2025 systematic review of case reports (Azmi and colleagues, PubMed | Our Assessment) examined Fournier’s gangrene in patients taking SGLT2 inhibitors. It included 14 case reports, noted that this complication is rare, and observed that management was multimodal, including discontinuation of the drug, aggressive debridement, antibiotics, and in several cases hyperbaric oxygen therapy, with reported discharge ranging from 9 to 51 days.
Because case reports cannot establish incidence or causation, the practical message is one of awareness rather than alarm: in a diabetic patient on an SGLT2 inhibitor who presents with perineal pain, swelling, or infection, keep Fournier’s gangrene on the differential and act quickly. Red flags that should lower your threshold for surgical referral include pain disproportionate to examination findings, rapidly advancing redness or swelling, crepitus, blistering, and signs of systemic sepsis.
Fournier’s gangrene and HBOT: evidence at a glance
| Study (year) | Design | Population | Key finding for HBOT |
|---|---|---|---|
| Patel et al. (2026) | Systematic review and meta-analysis (13 retrospective studies) | 322 HBOT vs 366 controls, Fournier’s gangrene | HBOT associated with significantly lower mortality; no significant difference in length of stay or debridements |
| Hyldegaard et al. (2025) | Prospective observational cohort (INFECT) | 409 NSTI patients; 329 received HBOT | Observational association with survival; evidence inconclusive; benefit may be largest in the most severely ill |
| Kariksiz et al. (2025) | Retrospective cohort | 50 lower-extremity NSTI patients | 20% mortality, 60% amputation; diabetes linked to amputation |
| Azmi et al. (2025) | Systematic review of case reports | 14 SGLT2-inhibitor-associated Fournier’s gangrene cases | Multimodal management often included HBOT; emerging risk signal |
Frequently asked questions about HBOT for Fournier’s gangrene
Does hyperbaric oxygen therapy cure Fournier’s gangrene on its own?
No. Hyperbaric oxygen therapy is an adjunct. The established foundation of treatment is urgent surgical debridement, broad-spectrum antibiotics, and resuscitation. HBOT is added to that care, and observational evidence associates it with lower mortality, but it does not replace surgery.
Is HBOT for necrotizing infection an approved indication?
Yes. Necrotizing soft tissue infections are listed among the indications recognised by the Undersea and Hyperbaric Medical Society. Fournier’s gangrene falls within that category as a necrotizing infection of the perineum and genitals.
How strong is the evidence that HBOT lowers mortality in Fournier’s gangrene?
The 2026 meta-analysis by Patel and colleagues pooled retrospective data and found an association with lower mortality, but no randomised controlled trial exists. Retrospective studies cannot rule out selection bias, so the finding is encouraging rather than definitive.
How quickly should hyperbaric treatment start?
Surgery always comes first. Hyperbaric referral should run in parallel so treatment can begin once the patient is stabilised. In the Scandinavian INFECT cohort, the median time from hospital arrival to the first hyperbaric treatment was 4.3 hours.
Which patients are at higher risk of Fournier’s gangrene?
Diabetes is the most consistent risk factor, and a 2025 systematic review of case reports flagged SGLT2 inhibitor use as an emerging signal. Keep the diagnosis on the differential in any diabetic patient with rapidly progressing perineal or genital infection.
Where can I find a hyperbaric facility in Canada for an urgent referral?
The Canada Hyperbarics facilities directory lists hospitals and regulated facilities across Canada, and the FAQ answers common questions about access. For urgent necrotizing infection, contact your nearest hospital-based hyperbaric programme and surgical service without delay.
The bottom line for referring physicians
Fournier’s gangrene is a surgical emergency where minutes matter. Hyperbaric oxygen therapy is a recognised adjunct, supported by observational data that associate it with lower mortality, and it should be arranged in parallel with, never instead of, surgical debridement and antibiotics. If you have a patient who may benefit, identify a hyperbaric centre early through the Canada Hyperbarics directory of hospitals and regulated facilities, and explore the underlying studies in our research library.
This content is for informational purposes only and does not constitute medical advice. It is intended to support, not replace, the clinical judgement of qualified healthcare professionals. Treatment decisions for necrotizing soft tissue infections should be made by the responsible surgical and infectious-disease teams.