
TL;DR: Hyperbaric oxygen therapy (HBOT) is a recognised adjunct, not a standalone cure, for chronic refractory osteomyelitis. Across 2024-2026 case series and retrospective cohorts, adding HBOT to culture-directed antibiotics and surgical debridement was associated with high rates of infection clearance and a reassuring safety profile. The evidence base remains observational, with no randomised controlled trials, so findings should be read as encouraging rather than definitive. For Canadian referring physicians, HBOT is most reasonable in selected patients whose bone infection persists despite optimal conventional care.
Chronic refractory osteomyelitis is one of the most stubborn problems a referring physician manages. When a bone infection refuses to clear despite appropriate surgery and antibiotics, adjunctive hyperbaric oxygen therapy becomes a reasonable next consideration. Hyperbaric oxygen therapy for refractory osteomyelitis is an oxygen-based adjunct that raises tissue oxygen tension in infected, poorly perfused bone to support healing, antibiotic activity, and host defence. This evidence review summarises what the 2024-2026 literature shows, how the treatment is delivered, and where the evidence stops, so Canadian physicians can counsel patients accurately. At Canada Hyperbarics, our role is to make that evidence easy to find and fair to read.
Reading time: about 9 minutes. Last updated: 24 June 2026.
What is refractory osteomyelitis, and why is it hard to treat?
Refractory osteomyelitis is a chronic bone infection that persists or recurs after appropriate surgical and antibiotic treatment. The Undersea and Hyperbaric Medical Society (UHMS) defines it as chronic osteomyelitis that persists or recurs after suitable interventions, or acute osteomyelitis that has not responded to accepted management. In practical terms, a 2025 review noted that patients can be classified as having chronic refractory disease when they show no meaningful improvement, or worsen, despite roughly 30 days of combined surgical and medical treatment that includes systemic antimicrobial therapy (Tettelbach, PubMed | Our Assessment).
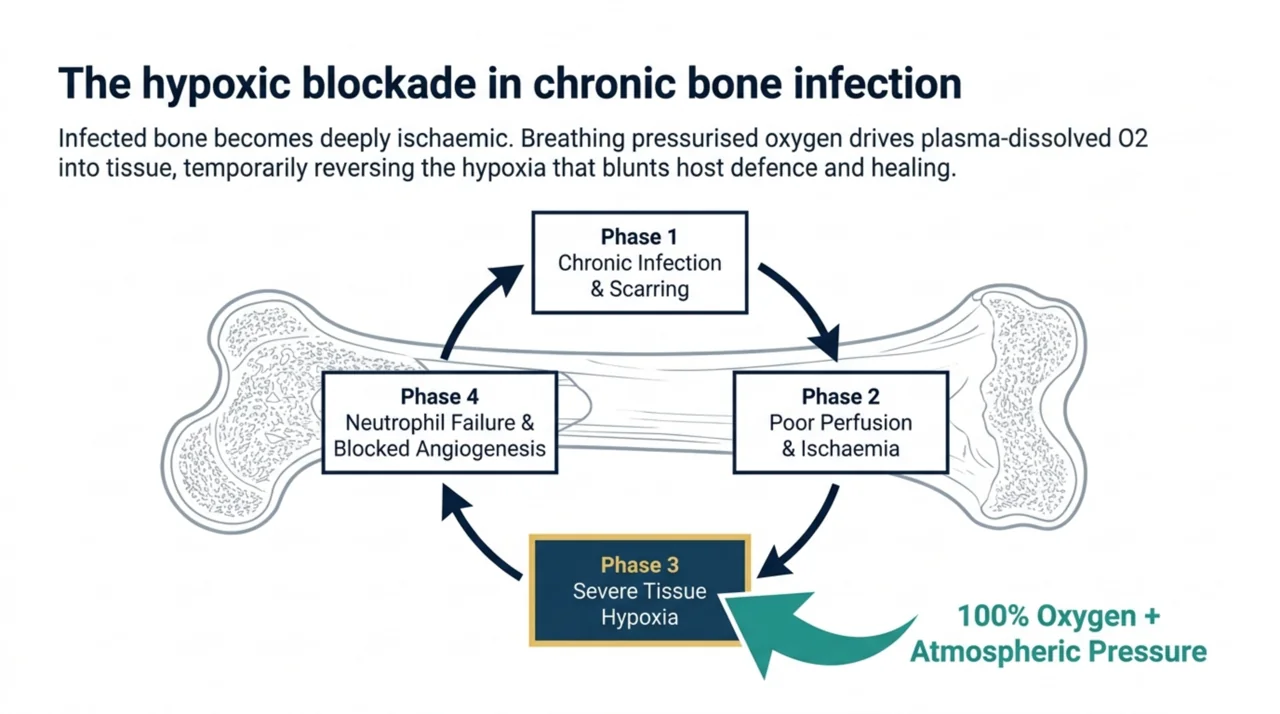
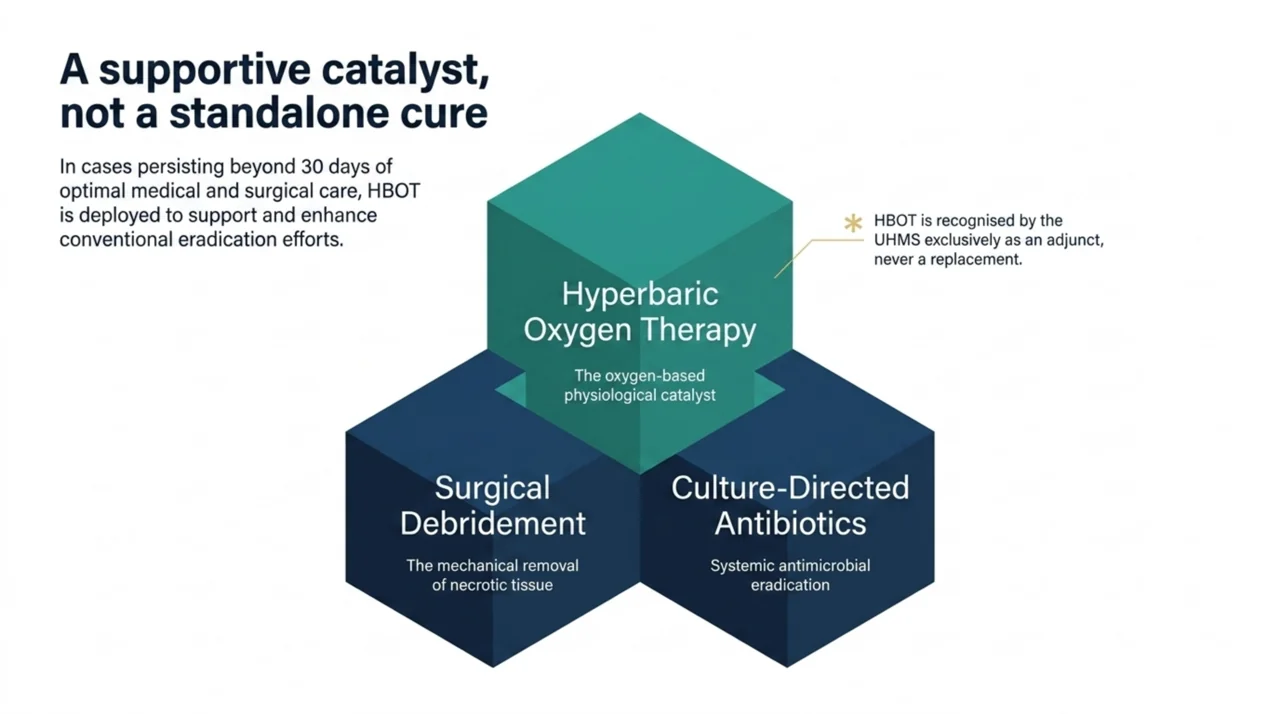
The reason these infections resist treatment is largely about oxygen. Infected and scarred bone is poorly perfused, so it becomes hypoxic. Low oxygen tension blunts the bacteria-killing function of neutrophils, limits the activity of several antibiotics, and slows the angiogenesis and osteoblast activity needed to rebuild bone. The rationale for hyperbaric oxygen is to temporarily reverse that hypoxia. Breathing 100% oxygen under increased pressure raises dissolved oxygen in plasma and drives it into ischaemic tissue, which is why HBOT is studied as an adjunct alongside, never instead of, debridement and antibiotics.
Is hyperbaric oxygen therapy a recognised indication for osteomyelitis?
Yes. Refractory osteomyelitis is one of the indications recognised by the UHMS for adjunctive hyperbaric oxygen therapy, alongside conditions such as delayed radiation injury, necrotising soft tissue infections, and compromised grafts and flaps. Recognition reflects a body of supportive clinical experience, not a claim that HBOT works in isolation. You can review how Canada Hyperbarics frames the regulatory picture on our regulatory overview, and the condition-specific summary on our refractory osteomyelitis page.
It is worth being precise with patients about language. The UHMS recognises indications based on evidence and expert consensus; it does not approve, license, or regulate therapy. Coverage and access in Canada are decided provincially, and most insured hyperbaric care is delivered through hospital programmes. Where a patient is treated, and whether costs are covered, depends on their province and referral pathway rather than on the UHMS list itself.
What does the 2024-2026 evidence show for HBOT in refractory osteomyelitis?
The recent literature is dominated by observational cohorts and case reports, which favour associational rather than causal conclusions. The signal, however, is consistent and points in a favourable direction.
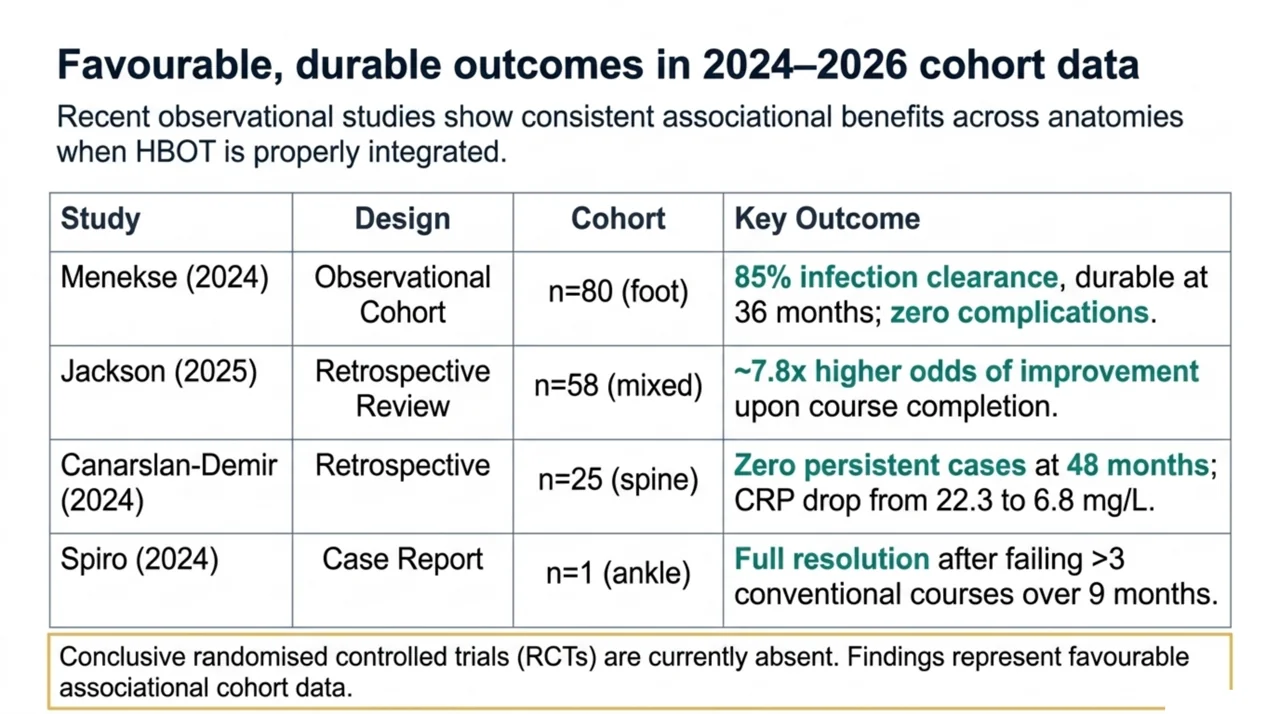
In a 2024 observational study of 80 patients with chronic refractory osteomyelitis of the foot, complete infection clearance was achieved in 85% (68 of 80) after surgical debridement, tailored antibiotics, and HBOT at 2.5 atmospheres absolute for 120 minutes, five days a week, over an average of about 50 days. That result held across a mean follow-up of 36 months, with no HBOT-related complications reported (Menekse, PubMed | Our Assessment). As a single-arm cohort, it cannot isolate the contribution of HBOT from concurrent surgery and antibiotics, but the durability of clearance is notable.
A 2025 retrospective review of 58 patients added an important nuance about who benefits. Patients who completed their HBOT course had roughly 7.8 times the odds of osteomyelitis improvement compared with those who started but did not finish, both overall (P = 0.015) and after controlling for disease stage (P = 0.006). However, completing HBOT was not significantly associated with the rate of full resolution, further surgery, or amputation, and patients with diabetes, peripheral vascular disease, or congestive heart failure had higher odds of amputation (Jackson, PubMed | Our Assessment). The practical message is that completion matters and that comorbidity burden shapes the realistic ceiling of benefit.
The evidence is not limited to the foot. In a 2024 retrospective cohort of 25 patients with spondylodiscitis (vertebral osteomyelitis), adjunctive HBOT plus targeted antibiotics was associated with lower median pain scores (from 8 to 3, P < 0.001), lower C-reactive protein (from 22.3 to 6.8 mg/L, P = 0.002), and lower white cell counts, with no persistent cases at a median follow-up of 48 months (Canarslan-Demir, PubMed | Our Assessment). A 2024 case report likewise described a 47-year-old active-duty patient whose post-fracture ankle osteomyelitis had failed more than three courses of combined surgical and medical care over nine months, then resolved after adjunctive HBOT (Spiro, PubMed | Our Assessment).
| Study (year) | Design | Patients | Key associated finding |
|---|---|---|---|
| Menekse (2024) | Observational cohort | 80 (foot) | 85% infection clearance; durable at 36 months; no HBOT complications |
| Jackson (2025) | Retrospective review | 58 | Course completion linked to ~7.8x odds of improvement; no change in resolution or amputation rate |
| Canarslan-Demir (2024) | Retrospective cohort | 25 (spine) | Lower pain, CRP and white cell counts; no persistent cases at 48 months |
| Spiro (2024) | Case report | 1 | Resolution after failure of more than three conventional courses |
How is adjunctive HBOT delivered for osteomyelitis?
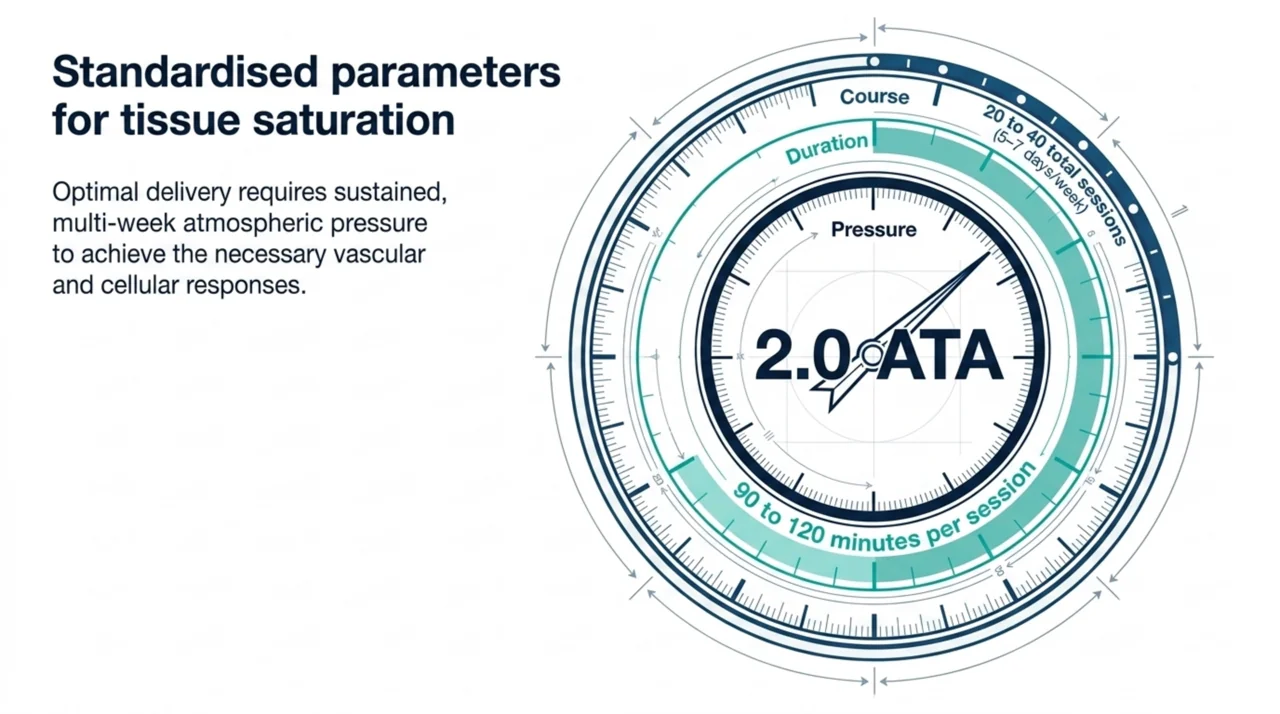
Protocols are reasonably consistent across centres. According to UHMS guidance, hyperbaric oxygen for refractory osteomyelitis is usually delivered once daily, five to seven days a week, for 90 to 120 minutes per session at 2.0 to 3.0 atmospheres absolute, with roughly 20 to 40 sessions needed to reach sustained benefit. Treatment works best when it is started soon after indicated debridement and paired with culture-directed antibiotics.
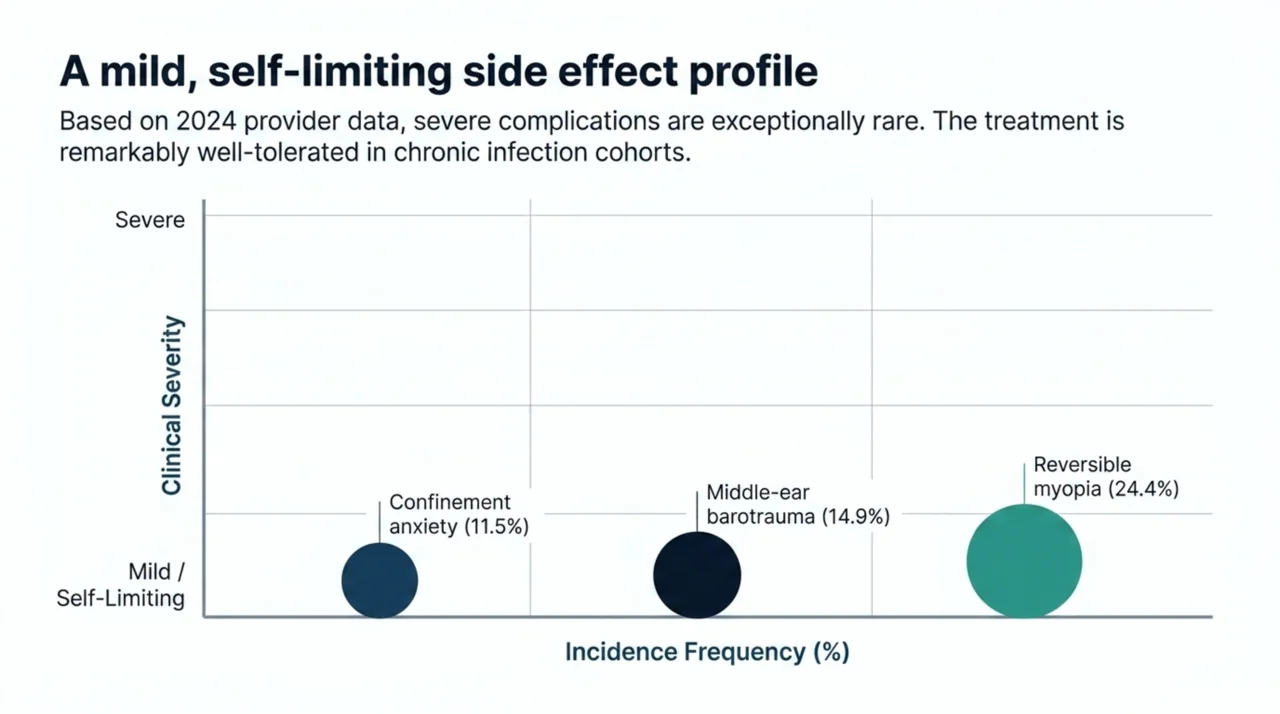
Real-world practice mirrors this. In a 2024 survey of 265 hyperbaric providers, 2.4 ATA was the single most common pressure overall (35.2%), but for chronic osteomyelitis specifically most providers chose 2.0 ATA (reported by 68.0 to 74.9% for that indication). The same survey catalogued the expected side-effect profile: reversible myopia was the most common at 24.4%, followed by middle-ear barotrauma at 14.9% and confinement anxiety at 11.5% (Laspro, PubMed | Our Assessment). These are generally mild and self-limiting, which is consistent with the strong safety record seen in the osteomyelitis cohorts above.
What are the limits of the current evidence?
Honesty about the evidence is part of good referral. To date there are no conclusive randomised controlled trials of HBOT for refractory osteomyelitis. The 2025 review that surveyed this field concluded that, on the balance of available studies, adding HBOT to routine surgical and antibiotic treatment of previously refractory osteomyelitis appears both safe and likely to improve infection resolution rates, while cautioning that many early positive results came from inpatient settings where treatment compliance was tightly controlled, and have not translated perfectly to outpatient care (Tettelbach, PubMed | Our Assessment).
For physicians, the takeaways are practical. Benefit is associational, not proven causal, so HBOT should be framed to patients as a supportive adjunct that may improve the odds of clearing a difficult infection. Surgery and culture-directed antibiotics remain the backbone of care. Patient selection and course completion appear to matter more than small differences in pressure. You can browse the full set of primary studies behind these conclusions in the Canada Hyperbarics research library.
When should a Canadian physician consider referring for HBOT?
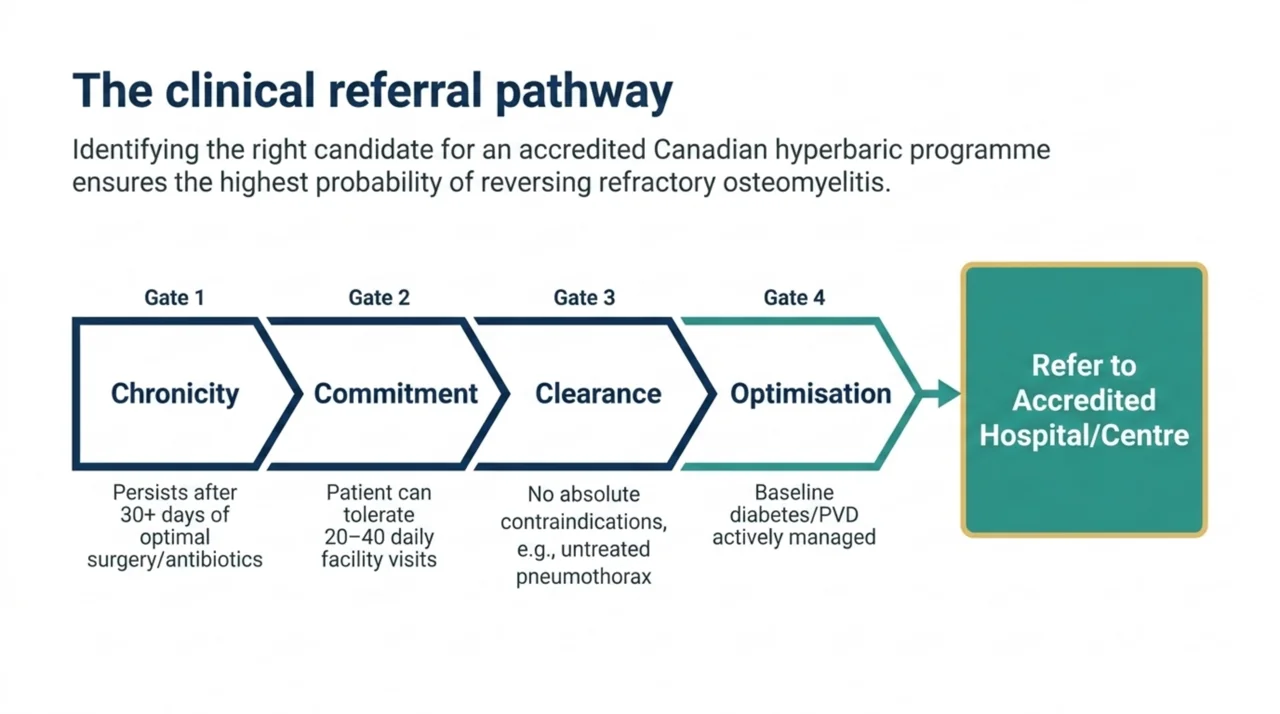
Adjunctive hyperbaric oxygen is worth considering when osteomyelitis remains active despite a genuine trial of optimal conventional care. A reasonable referral profile includes:
- Confirmed chronic osteomyelitis that has persisted or recurred despite appropriate surgical debridement and systemic antibiotics, typically over at least 30 days of combined treatment.
- A patient able to tolerate and commit to a multi-week daily course, since completion is linked to better outcomes.
- No absolute contraindication to hyperbaric exposure, such as an untreated pneumothorax or certain chemotherapy agents.
- Comorbidities such as diabetes or peripheral vascular disease identified and optimised, since they shape the realistic ceiling of benefit.
Hyperbaric oxygen therapy in Canada is delivered through hospitals and regulated facilities rather than at home, so the practical first step is identifying an accredited centre that accepts referrals for your patient’s province. You can locate one through the Canada Hyperbarics directory of hospitals and regulated facilities.
Frequently asked questions about HBOT for refractory osteomyelitis
Does hyperbaric oxygen therapy replace antibiotics or surgery for osteomyelitis?
No. In every study reviewed here, HBOT was used as an adjunct alongside surgical debridement and culture-directed antibiotics. It is intended to support conventional treatment in difficult cases, not to replace it.
How many HBOT sessions are typically needed for refractory osteomyelitis?
UHMS guidance describes roughly 20 to 40 daily sessions of 90 to 120 minutes at 2.0 to 3.0 ATA. Reported osteomyelitis cohorts have used courses lasting several weeks, and completing the full course is associated with better results.
Is HBOT safe for patients with chronic bone infection?
The osteomyelitis cohorts reported no serious HBOT-related complications. The most common side effects in hyperbaric practice are reversible short-sightedness, middle-ear barotrauma, and confinement anxiety, which are generally mild and self-limiting.
Does HBOT for osteomyelitis prevent amputation?
The evidence does not support a firm claim here. In the largest retrospective review, completing HBOT was associated with improvement but was not significantly linked to lower rates of further surgery or amputation, and amputation risk rose with diabetes, peripheral vascular disease, and heart failure.
Can HBOT help osteomyelitis outside the foot, such as the spine?
There is supportive observational evidence beyond the foot. A retrospective cohort of patients with spondylodiscitis, a form of vertebral osteomyelitis, reported lower pain scores and inflammatory markers and no persistent cases at long-term follow-up when HBOT was added to targeted antibiotics.
Is the evidence for HBOT in osteomyelitis strong?
It is supportive but not definitive. There are no randomised controlled trials, so current conclusions rest on case series and retrospective cohorts. These consistently suggest benefit and strong safety, which is enough to justify selective referral but not enough to call the matter settled.
For more common patient questions and a plain-language overview of how the therapy works, see the Canada Hyperbarics frequently asked questions.
The bottom line for referring physicians
Adjunctive hyperbaric oxygen therapy is a reasonable, recognised, and well-tolerated option for chronic refractory osteomyelitis that has not yielded to optimal surgery and antibiotics. The 2024-2026 evidence is observational, so benefit should be presented as an improved chance of clearing a hard infection rather than a guarantee. Selecting committed patients, optimising comorbidities, and ensuring course completion give the therapy its best chance to help. To match a patient with an accredited centre, start with the Canada Hyperbarics directory of hospitals and regulated facilities.
This content is for informational purposes only and does not constitute medical advice. It is intended to support, not replace, clinical judgement and the patient-physician relationship. Treatment decisions should be made with a qualified healthcare provider.