
TL;DR: Hyperbaric oxygen therapy (HBOT) is an emerging adjunctive treatment for severe frostbite, not a Health Canada-recognised or UHMS-recognised indication. The current evidence is limited to case series, retrospective cohorts, and one prospective study with a historical control. A 2021 multicentre study reported more preserved digit segments when HBOT was added to iloprost, while a 2023 matched cohort found no difference in amputation. A 2020 Cochrane review concluded the benefits and harms remain unclear. For Canadian physicians, HBOT is best considered early, alongside rewarming and thrombolytic or vasodilator therapy, for grade 3 to 4 injuries at an accredited hyperbaric programme.
Frostbite is a freezing injury in which ice crystals form in tissue exposed to sub-zero temperatures, triggering ischaemia, thrombosis, and potential tissue death. For Canadian referring physicians, it is a recurring winter problem, particularly among people working outdoors, those experiencing homelessness, and patients with intoxication or psychiatric illness. This evidence review summarises what the 2000 to 2026 literature says about HBOT for frostbite, where hyperbaric oxygen therapy fits within current management, and when referral may be worth considering. The goal is a precise, evidence-matched summary you can use at the bedside, not a treatment recommendation.
Canada Hyperbarics maintains an independent research library and a directory of Canadian hyperbaric facilities. Every study cited below links to both the primary source on PubMed and our own structured assessment, so you can verify each claim against the original abstract.
What is frostbite, and why might hyperbaric oxygen help?
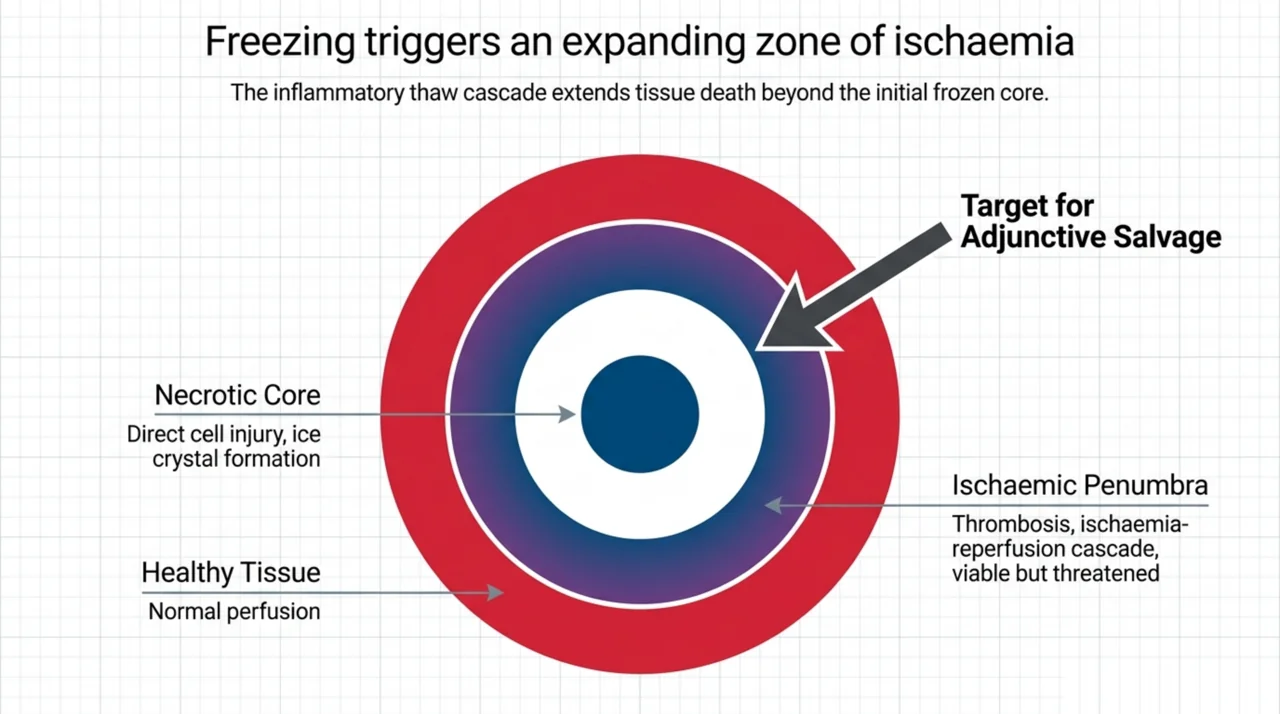
Frostbite progresses in stages. Initial freezing causes direct cell injury, and the subsequent thaw drives an inflammatory, thrombotic, and ischaemia-reperfusion cascade that extends tissue loss well beyond the original frozen zone. The viable but threatened tissue around the necrotic core is often called the ischaemic penumbra, and it is the target of most adjunctive therapies.
The mechanistic rationale for hyperbaric oxygen is that breathing 100 percent oxygen under pressure sharply increases the amount of oxygen dissolved in plasma, raising oxygen delivery to hypoxic tissue independent of red blood cell flow. A 2025 Hyperbaric Medicine Indications Manual chapter groups frostbite with the other “acute traumatic ischaemias” such as crush injury, burns, and compromised flaps, noting that these conditions share a common ischaemia-reperfusion pathophysiology that HBOT mechanisms are proposed to mitigate (Strauss, 2025, PubMed | Our Assessment). This shared mechanism is one reason frostbite is studied alongside the more established acute traumatic ischaemia indications, several of which appear on our conditions index.
Is hyperbaric oxygen therapy an approved treatment for frostbite in Canada?
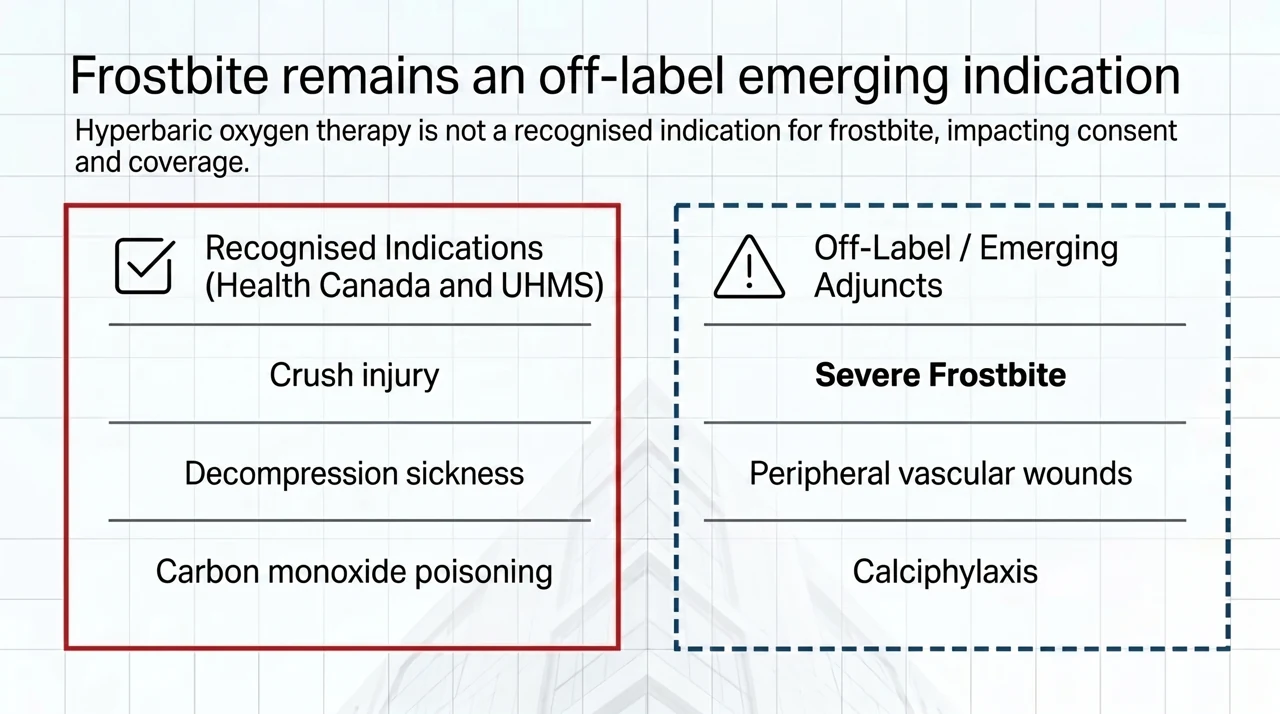
No. Frostbite is not currently a Health Canada-recognised or UHMS-recognised indication for hyperbaric oxygen therapy. It is used off-label as an adjunct. The Undersea and Hyperbaric Medical Society (UHMS) recognised indications list includes established indications such as decompression sickness, carbon monoxide poisoning, crush injury, and selected problem wounds, but frostbite is not among them. That regulatory status matters for documentation, consent, and any coverage discussion.
Frostbite does, however, appear in real-world hyperbaric practice as an emerging indication. A 2024 international registry study of 9,726 hyperbaric treatment entries found that 378 (3.89 percent) were for emerging indications, and frostbite accounted for 18 of those 378 cases (4.8 percent), placing it among the more frequently treated emerging indications alongside calciphylaxis and peripheral vascular wounds (Tanaka et al., 2024, PubMed | Our Assessment). In other words, clinicians are already reaching for HBOT in severe frostbite, even though the formal evidence base remains thin.
What does the clinical evidence on HBOT for frostbite show?
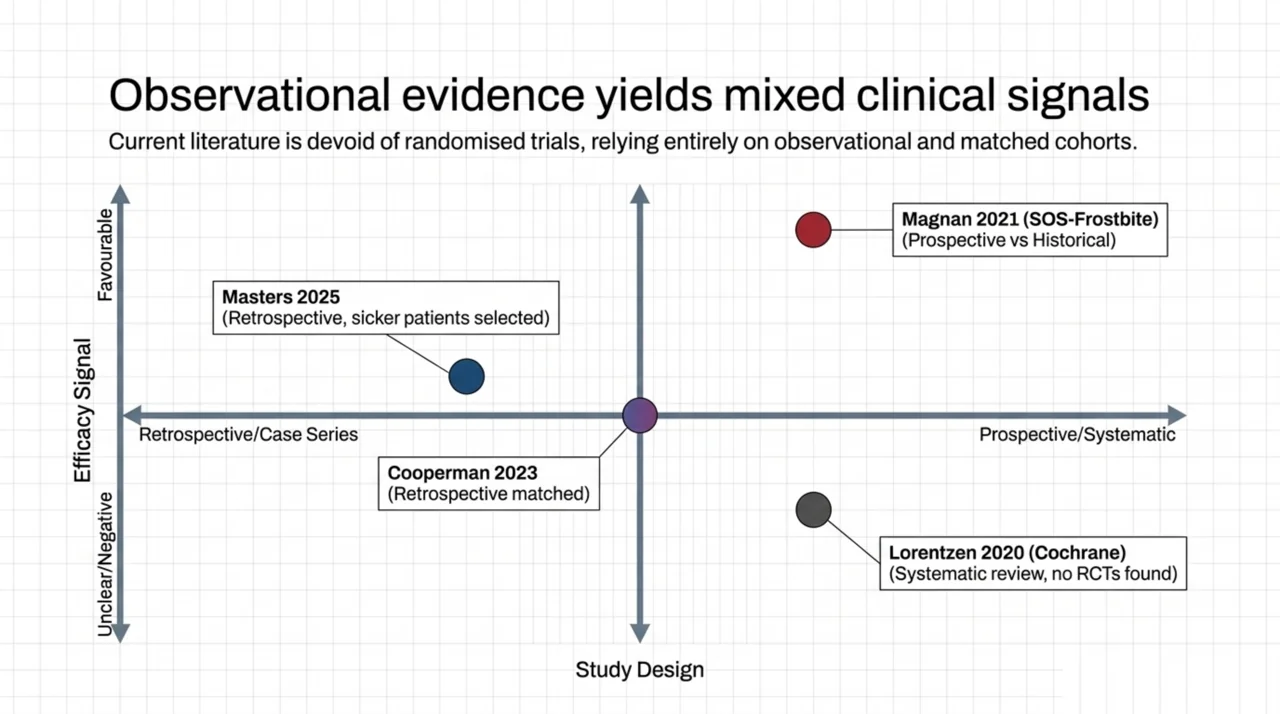
The honest summary is that the evidence is limited, mostly observational, and mixed. There are no randomised controlled trials. The strongest positive signal comes from the SOS-Frostbite study, a multicentre prospective single-arm study run across hyperbaric centres in Geneva, Lyon, and Mont-Blanc. Patients with stage 3 or 4 frostbite who started care within 72 hours received early HBOT in addition to standard iloprost, and outcomes were compared to a historical cohort treated with iloprost alone. The prospective HBOT-plus-iloprost group preserved significantly more tissue, with a mean of 13 preserved segments per patient versus 6 in the historical group (p = 0.006), and the adjusted odds ratio favoured the HBOT group by 45-fold (95 percent CI 6 to 335, p < 0.001) (Magnan et al., 2021, PubMed | Our Assessment). Because this was a prospective group compared to a historical control rather than a randomised trial, the result is associational and should be read with caution.
A counterbalancing finding comes from a 2023 multicentre retrospective comparative cohort of digital frostbite, one of the largest to date. Using one-to-one matching of HBOT-treated and non-HBOT-treated patients, the investigators found a low overall amputation rate of 5.2 percent and no statistically significant difference in amputation outcomes between the matched groups. Patients treated with HBOT did have a longer hospital stay (22.2 days versus 6.39 days) (Cooperman et al., 2023, PubMed | Our Assessment). A 2025 retrospective cohort at a high-volume burn centre studied 214 patients, 62 of whom received HBOT, and reported that the HBOT-treated patients tended to have larger areas of tissue injury and to undergo more surgical interventions, reflecting that the sickest patients were selected for treatment. The authors described a complex relationship and underscored the need for controlled trials (Masters et al., 2025, PubMed | Our Assessment). This is a classic example of confounding by indication, and it cautions against reading better outcomes into uncontrolled comparisons.
A Canadian perspective is available too. A single major Canadian university hospital reported its experience with 22 frostbite patients treated with HBOT as an adjunct to wound care between 2000 and 2015. The cohort was mostly men (18, or 81.8 percent), with a mean age of 40 years; intoxication was present in 45.5 percent and psychiatric illness was implicated in 40.9 percent, and the upper extremity was affected in 77.3 percent (Ghumman et al., 2019, PubMed | Our Assessment). That demographic profile mirrors what many Canadian emergency departments see and is worth keeping in mind when planning follow-up. Finally, a 2020 Cochrane systematic review of interventions for frostbite, which searched specifically for randomised controlled trials of HBOT, sympathectomy, thrombolytics, and vasodilators, concluded that the benefits and harms of these interventions remain unclear (Lorentzen et al., 2020, PubMed | Our Assessment).
| Study (year) | Design | Population | Key finding (associational) |
|---|---|---|---|
| Magnan, 2021 (SOS-Frostbite) | Prospective single-arm vs historical control | 28 prospective vs 30 historical, stage 3 to 4 | More preserved segments with HBOT plus iloprost (13 vs 6, p = 0.006) |
| Cooperman, 2023 | Retrospective matched comparative cohort | Digital frostbite, matched pairs | No amputation difference; longer stay with HBOT (22.2 vs 6.39 days) |
| Masters, 2025 | Retrospective cohort, burn centre | 214 patients, 62 treated with HBOT | HBOT patients sicker; complex relationship, calls for trials |
| Ghumman, 2019 | Retrospective single-centre (Canada) | 22 patients | Describes Canadian usage; intoxication and psychiatric illness common |
| Lorentzen, 2020 (Cochrane) | Systematic review | RCTs sought | Benefits and harms unclear; no HBOT RCTs identified |
| Tanaka, 2024 | International registry cohort | 18 frostbite cases of 378 emerging | Frostbite is a recognised emerging indication (4.8 percent) |
How does HBOT fit within current frostbite management?
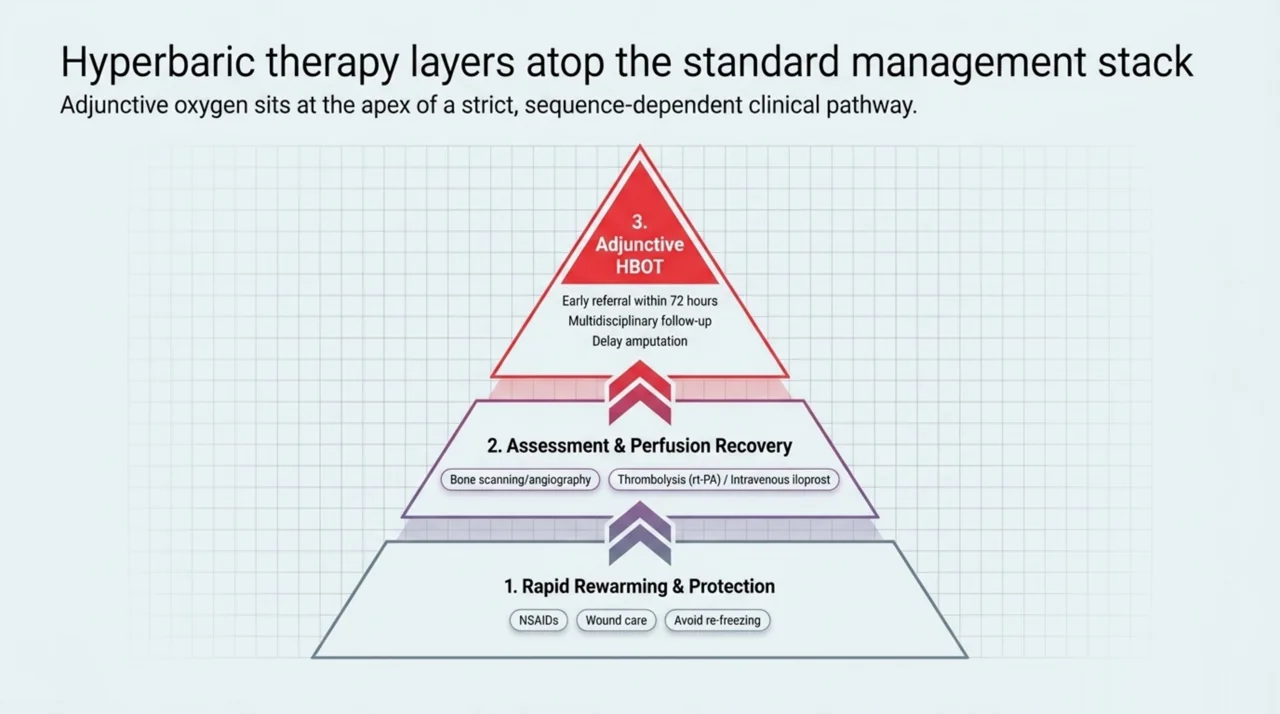
Hyperbaric oxygen is never a standalone frostbite treatment. A 2025 updated review of upper-limb frostbite describes the current management pathway as early and rapid rewarming, avoiding any re-freezing of warmed tissue, wound dressings and protection, and NSAIDs for analgesia and to limit inflammatory injury. The review notes that thrombolysis with tissue plasminogen activator (rt-PA) and intravenous iloprost have improved outcomes for severe frostbite, and that arteriography can help monitor perfusion (Saraoui et al., 2025, PubMed | Our Assessment). Across the broader literature reviewed in this post, HBOT consistently sits within that standard framework as an adjunct layered on top of rewarming, wound care, and thrombolysis, rather than as a replacement for them.
For a Canadian physician weighing a referral, a practical sequence based on the reviewed literature looks like this:
- Provide rapid rewarming of the affected tissue and protect it from re-freezing, the foundational first step in every frostbite review.
- Treat pain and inflammation with NSAIDs and give appropriate wound care.
- Assess injury depth and perfusion, using bone scanning or angiography where available, to identify grade 3 to 4 injuries with tissue at risk.
- For severe injury presenting early, consider thrombolysis with rt-PA and/or intravenous iloprost within the therapeutic window, as supported by current reviews.
- If HBOT is being considered as an adjunct, refer early to an accredited hyperbaric programme; the SOS-Frostbite protocol enrolled patients who began care within 72 hours.
- Coordinate multidisciplinary follow-up with plastic surgery and wound care, and delay any amputation decision until tissue demarcation is clear.
Which patients might a Canadian physician consider referring?
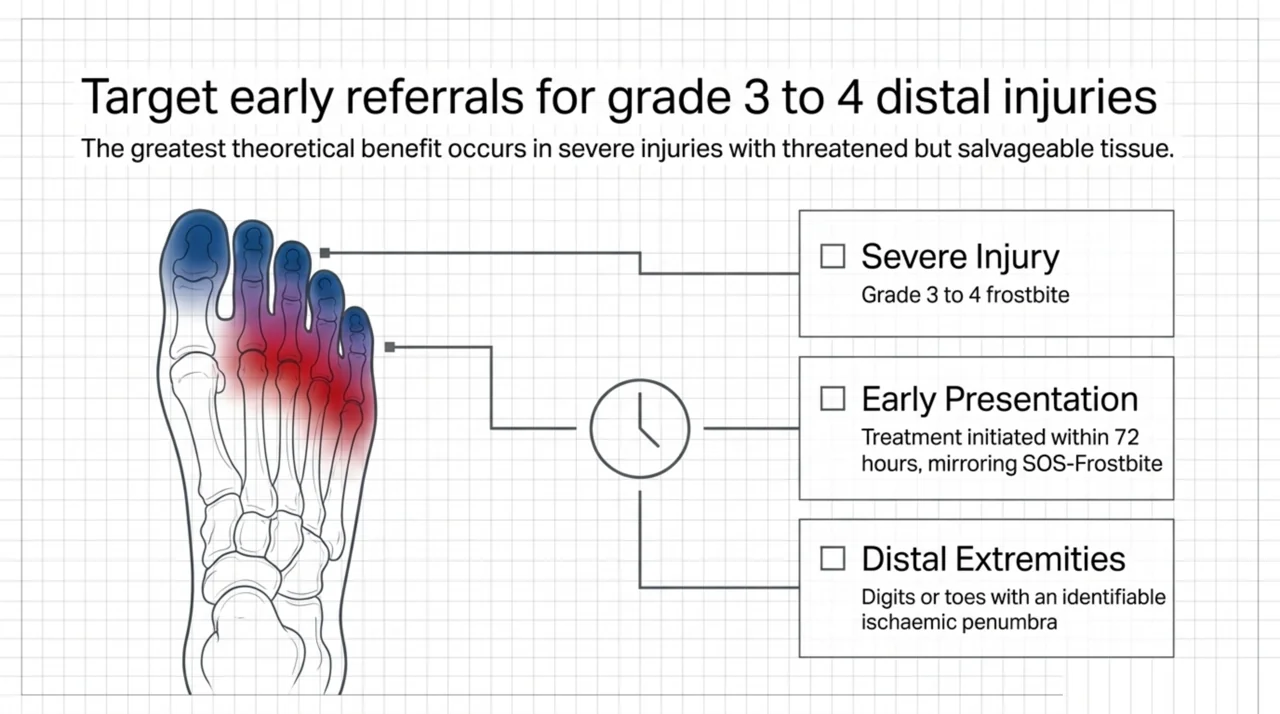
The patients most often described in the HBOT literature have severe, deep (grade 3 to 4) frostbite of the digits or distal extremities, present relatively early, and have tissue that is threatened but not yet clearly necrotic. A 2026 case from Tasmania illustrates the typical use: a patient with grade 3 to 4 frostbite of both feet received adjunctive HBOT along with vasodilators and rheological agents, and the authors reported that HBOT seemed to reduce the ischaemic penumbra and possibly reduced the level of joint amputation in the toes, while stressing that the best protocol is still unknown and more studies are needed (Stevens, 2026, PubMed | Our Assessment). That cautious, hedged language is typical of the entire frostbite-HBOT literature and should shape how the option is presented to patients.
Access is the other practical constraint. HBOT for frostbite is only deliverable where a multiplace or monoplace chamber is staffed and available, which in Canada means hospitals and regulated facilities with hyperbaric programmes. You can use the Canada Hyperbarics directory of Canadian hospitals and regulated facilities to identify the nearest accredited programme before making a time-sensitive referral, and the research library to review the underlying studies in full.
Frequently asked questions about HBOT for frostbite
Is HBOT approved for frostbite in Canada?
No. Frostbite is not a Health Canada-recognised or UHMS-recognised hyperbaric indication. It is used off-label as an adjunct to standard frostbite care, which should be reflected in your consent and documentation.
How might hyperbaric oxygen help in frostbite?
The proposed mechanism is increased oxygen delivery to the ischaemic penumbra. Breathing oxygen under pressure raises the oxygen dissolved in plasma, which may support tissue in the zone of injury that surrounds frankly necrotic areas.
When should HBOT be started after frostbite?
Earlier is generally considered better, and the SOS-Frostbite protocol enrolled patients who began care within 72 hours. That said, several case reports describe delayed HBOT used days after injury, so the optimal timing is not firmly established.
Does HBOT prevent amputation in frostbite?
The evidence is mixed. One prospective study reported more preserved tissue when HBOT was added to iloprost, while a matched retrospective cohort found no difference in amputation. Because there are no randomised trials, a definitive prevention claim cannot be made.
Is HBOT used alone or with other treatments?
Always with other treatments. HBOT is layered on top of rapid rewarming, wound care, NSAIDs, and, in severe cases, thrombolysis with rt-PA or intravenous iloprost. It is an adjunct, not a substitute for standard frostbite management.
Where is HBOT available for frostbite in Canada?
Only at hospitals and regulated facilities with a staffed hyperbaric chamber. Because frostbite is time-sensitive, identify the nearest accredited programme early using the Canada Hyperbarics facilities directory rather than after the fact.
Key takeaways for referring physicians
HBOT for frostbite is a reasonable adjunct to consider in severe, early-presenting injury, but it is an emerging and off-label use supported by observational data rather than randomised trials. Match the strength of any claim you make to the strength of the evidence, treat rewarming and thrombolysis or vasodilators as the backbone of care, and refer early when a hyperbaric programme is accessible. If you are deciding where to send a patient, the Canada Hyperbarics directory of hospitals and regulated facilities lists Canadian hyperbaric programmes by province.
This content is for informational purposes only and does not constitute medical advice. It is intended to support, not replace, the clinical judgement of qualified healthcare professionals. Treatment decisions should be made on a case-by-case basis in consultation with the treating team.