
Reading time: about 10 minutes
TL;DR: Arterial gas embolism is a medical emergency in which gas bubbles enter the arterial circulation and block blood flow to the brain or heart. Hyperbaric oxygen therapy is the recognised definitive treatment, and it works best when started early. For any patient with sudden neurological collapse after diving, central-line manipulation, or a surgical or imaging procedure that introduces air, the referring physician’s job is to stabilise, give high-flow oxygen, position the patient correctly, and arrange urgent transfer to a hospital with a hyperbaric chamber. Canada Hyperbarics maintains a directory of hospitals and regulated facilities that offer emergency recompression.
Arterial gas embolism (AGE) is a life-threatening condition in which gas bubbles enter the arterial bloodstream and obstruct circulation to vital organs, most often the brain. When the brain is affected, the condition is called cerebral arterial gas embolism (CAGE). It is one of the conditions the Undersea and Hyperbaric Medical Society lists as a primary indication for hyperbaric oxygen therapy (HBOT). For Canadian referring physicians, the single most important fact is this: outcomes depend on how quickly the patient reaches a recompression chamber, so recognition and referral are time-critical. This guide explains when to suspect gas embolism, what to do in the first minutes, and how to access hyperbaric care in Canada.
What is arterial gas embolism, and why is it a medical emergency?
Gas can enter the circulation through two broad routes. Venous gas embolism occurs when air enters a vein and travels toward the lungs, where small volumes are usually filtered and absorbed. Arterial gas embolism occurs when gas reaches the arterial side, either directly or by passing through a right-to-left shunt such as a patent foramen ovale, and then lodges in end-arteries that supply the brain or heart. Because arterial bubbles obstruct perfusion to tissue that tolerates very little ischaemia, even a small volume can cause sudden, severe injury.
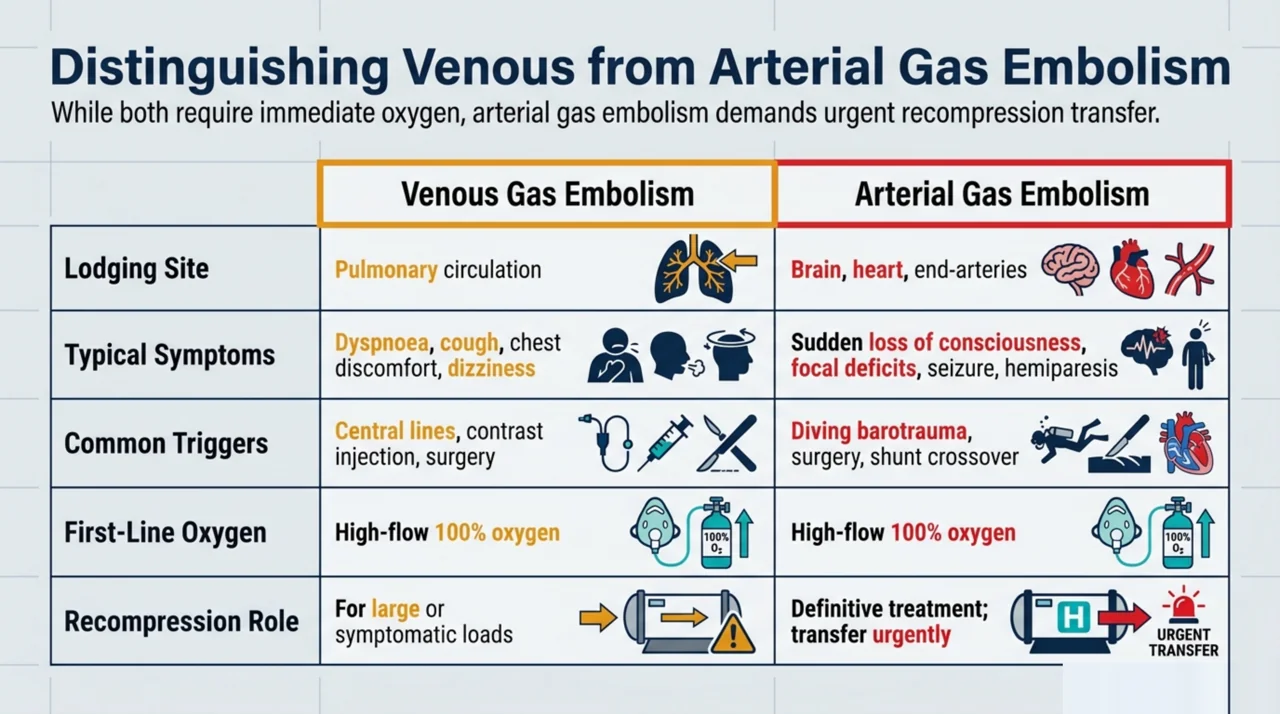
The two presentations differ in urgency and management, which is why distinguishing them matters at the bedside.
| Feature | Venous gas embolism | Arterial gas embolism |
|---|---|---|
| Where gas lodges | Pulmonary circulation | Brain, heart, other end-arteries |
| Typical symptoms | Dyspnea, cough, chest discomfort, dizziness | Sudden loss of consciousness, focal deficits, seizure, hemiparesis |
| Common triggers | Central lines, contrast injection, surgery | Diving barotrauma, surgery, shunt crossover from venous gas |
| First-line oxygen | High-flow 100% oxygen | High-flow 100% oxygen |
| Role of recompression | For large or symptomatic loads | Definitive treatment; transfer urgently |
Gas embolism is most familiar from diving medicine, where rapid ascent and pulmonary barotrauma can force gas into the pulmonary veins. But a growing share of cases in Canadian hospitals is iatrogenic, arising from medical procedures rather than diving. Recognising that an embolism can follow an everyday intervention is the first step toward an early referral.
How does hyperbaric oxygen therapy treat arterial gas embolism?
Hyperbaric oxygen therapy treats gas embolism through a combination of physics and physiology. Placing the patient under increased ambient pressure mechanically compresses the gas bubbles, following Boyle’s law, so they shrink and are more readily reabsorbed. Breathing 100% oxygen at pressure also steepens the gradient that washes inert nitrogen out of the bubble and floods ischaemic tissue with dissolved oxygen. A 2026 review by Bhargava and colleagues (PubMed | Our Assessment) describes HBOT as breathing pure oxygen at roughly 2 to 2.5 atmospheres, notes that its effect is dose-dependent within hypoxic tissue, and highlights its neuroprotective role after central nervous system injury under protocols set by bodies such as the Undersea and Hyperbaric Medical Society and the European Underwater and Baromedical Society.
Beyond bubble compression, hyperoxia appears to trigger protective cellular responses. A 2026 mechanistic review by Zhou and colleagues (PubMed | Our Assessment) explains that hyperbaric oxygen was first used in diving and aerospace settings for denitrogenation, and that its broader protective effects are thought to be driven by reactive oxygen species acting as signalling molecules. These signals upregulate protective proteins such as heme oxygenase-1, heat shock proteins, and vascular endothelial growth factor, which the authors associate with improved tolerance to ischaemic, inflammatory, and oxidative injury. For embolism, this means HBOT may do more than physically shrink bubbles; it may also support the brain tissue left hypoxic in the bubble’s wake. The standard recompression protocol for acute arterial gas embolism is the US Navy Treatment Table 6, a higher-pressure schedule that begins at 2.8 atmospheres absolute (60 feet of seawater) on 100% oxygen and can escalate to 6.0 atmospheres on Table 6A if severe symptoms persist. You can review the condition framing on the Canada Hyperbarics air or gas embolism resource.
When should you refer a patient with suspected gas embolism?
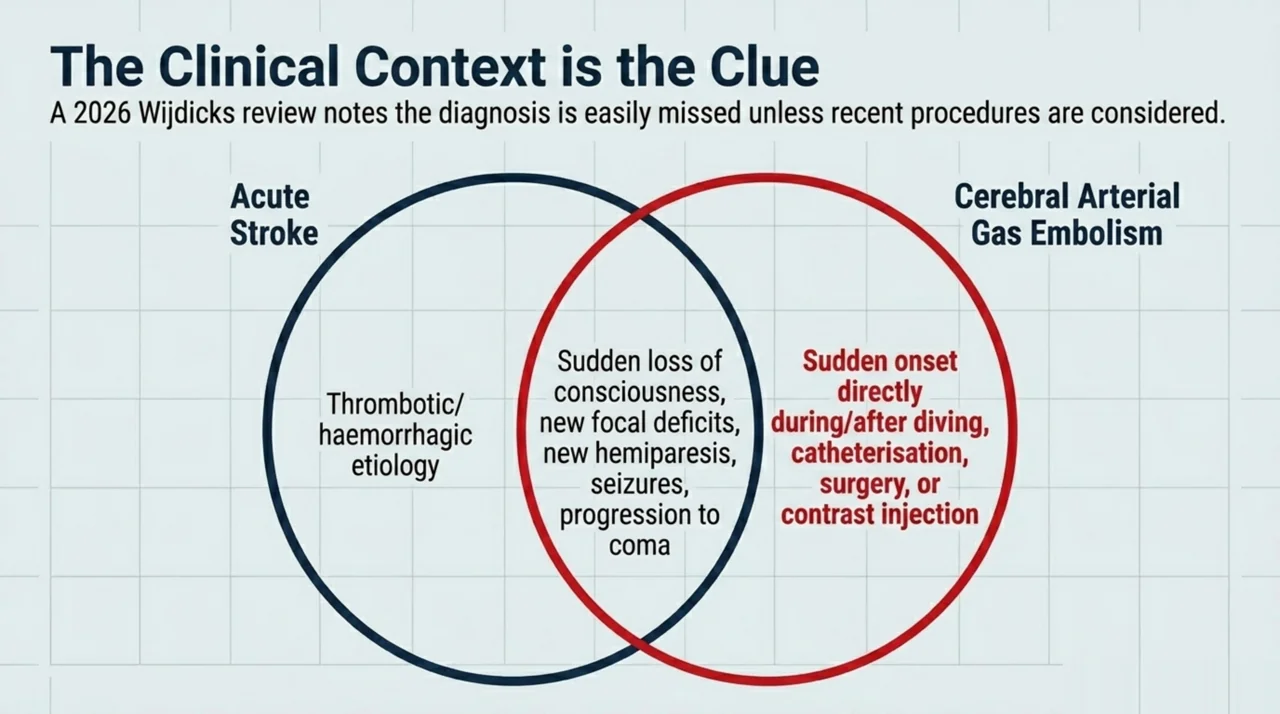
Refer urgently whenever a patient develops sudden neurological or cardiopulmonary collapse in a setting where gas could have entered the circulation. A 2026 review by Wijdicks and colleagues (PubMed | Our Assessment) describes the classic picture as an acute decline in level of consciousness with new focal deficits, often a new hemiparesis, and notes that a single seizure can be the heralding sign. Patients may progress to deep coma. Because these features overlap with stroke, the diagnosis is easy to miss unless the recent procedure or dive is kept in mind.
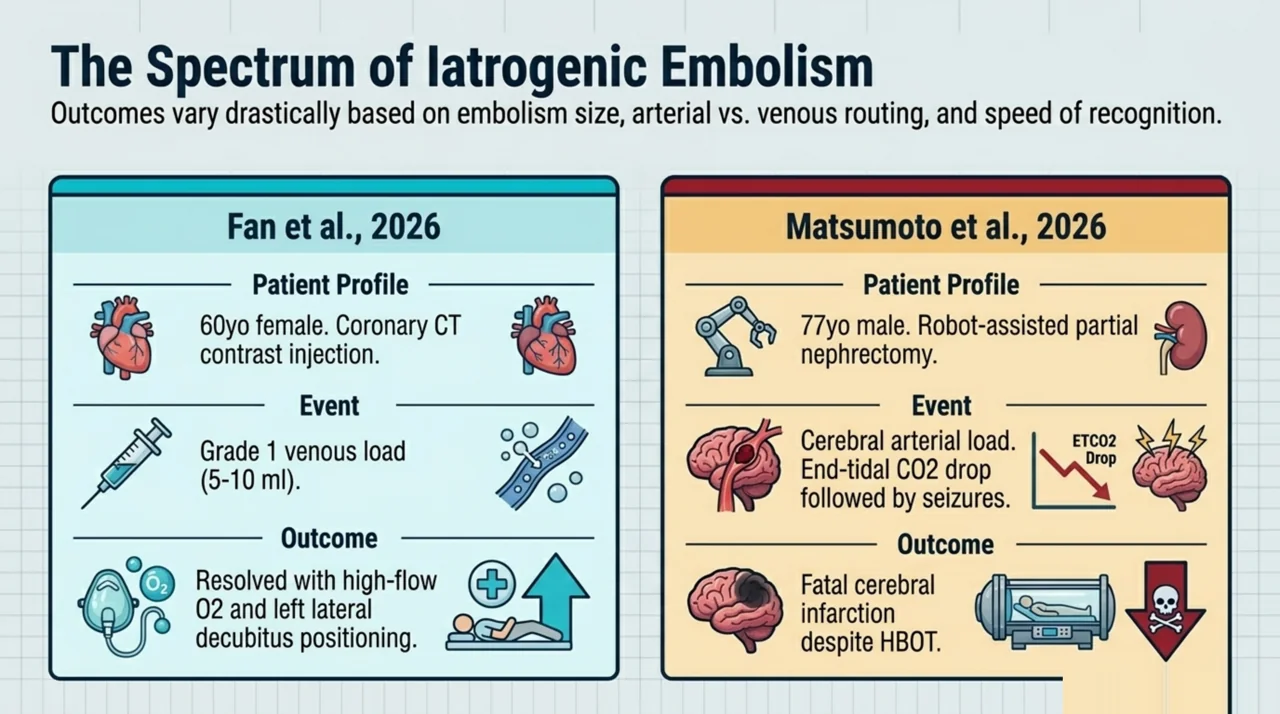
The clinical context is the clue. Suspect gas embolism after diving with a rapid ascent, after central venous catheter insertion or removal, during or after thoracic, neurosurgical, or laparoscopic surgery, and after contrast-enhanced imaging. A 2026 case report by Fan and colleagues (PubMed | Our Assessment) documented a 60-year-old woman who developed dyspnea and dizziness about one minute after contrast injection during coronary CT angiography. She was diagnosed with a grade 1 venous air embolism of an estimated 5 to 10 millilitres, and her symptoms settled with high-flow oxygen at 10 litres per minute, fluids, and left lateral decubitus positioning, with the air fully absorbed on a follow-up scan seven days later. The case is a reminder that even routine imaging can introduce gas, and that mild venous cases may resolve with prompt oxygen and positioning rather than recompression.
What are the immediate first steps before transfer to a chamber?
While arranging transfer, the referring team can take several steps that the Wijdicks review identifies as first-line for air embolism to the brain. These measures buy time and may limit injury before recompression.
- Position the patient. Keep the patient supine (lying flat). Current guidance does not recommend the head-down Trendelenburg position for arterial gas embolism, as it can worsen cerebral oedema; the head-down left lateral decubitus (Durant) position is used for venous air embolism, which is a separate entity.
- Give high-flow oxygen. Deliver oxygen through a closed face mask at 10 to 15 litres per minute, or high-flow nasal cannulae up to 60 litres per minute. Breathing 100% oxygen helps wash out inert gas.
- Support circulation and airway. Provide fluid resuscitation and standard resuscitative care as the clinical state requires.
- Call the hyperbaric service early. The review recommends hyperbaric oxygen therapy if a facility can be reached within an eight-hour window, so do not wait for full diagnostic certainty before making contact.
- Arrange urgent transfer. Treat transport as time-critical and coordinate directly with the receiving hospital and regulated facility.
Early contact matters because the chamber team can advise on stabilisation, accept the patient, and prepare a treatment table while transport is underway. You can identify the nearest emergency chamber through the directory of hospitals and regulated facilities maintained by Canada Hyperbarics.
What do recent cases reveal about iatrogenic gas embolism?
Procedure-related embolism can be devastating, which is why prevention and rapid recognition are so important. A 2026 case report by Matsumoto and colleagues (PubMed | Our Assessment) described a 77-year-old man who developed cerebral air embolism during robot-assisted partial nephrectomy. The first intraoperative sign was a sudden drop in end-tidal carbon dioxide; the patient then developed seizures, and imaging confirmed cerebral air embolisation. Despite hyperbaric oxygen therapy and intensive care, he progressed to a fatal cerebral infarction. The authors emphasise surgical precautions to prevent gas entry, and the case underscores an honest point for referrers: HBOT is the definitive treatment, but it does not guarantee survival, so speed and prevention both matter.
These two procedural cases bracket the spectrum. A small venous load after contrast may resolve with oxygen and positioning, while a cerebral arterial embolism during surgery can be fatal even with full treatment. The variable that the referring physician most influences is time: the sooner gas embolism is suspected and the hyperbaric service is contacted, the better the window for meaningful recovery.
What outcomes can physicians expect after hyperbaric treatment?
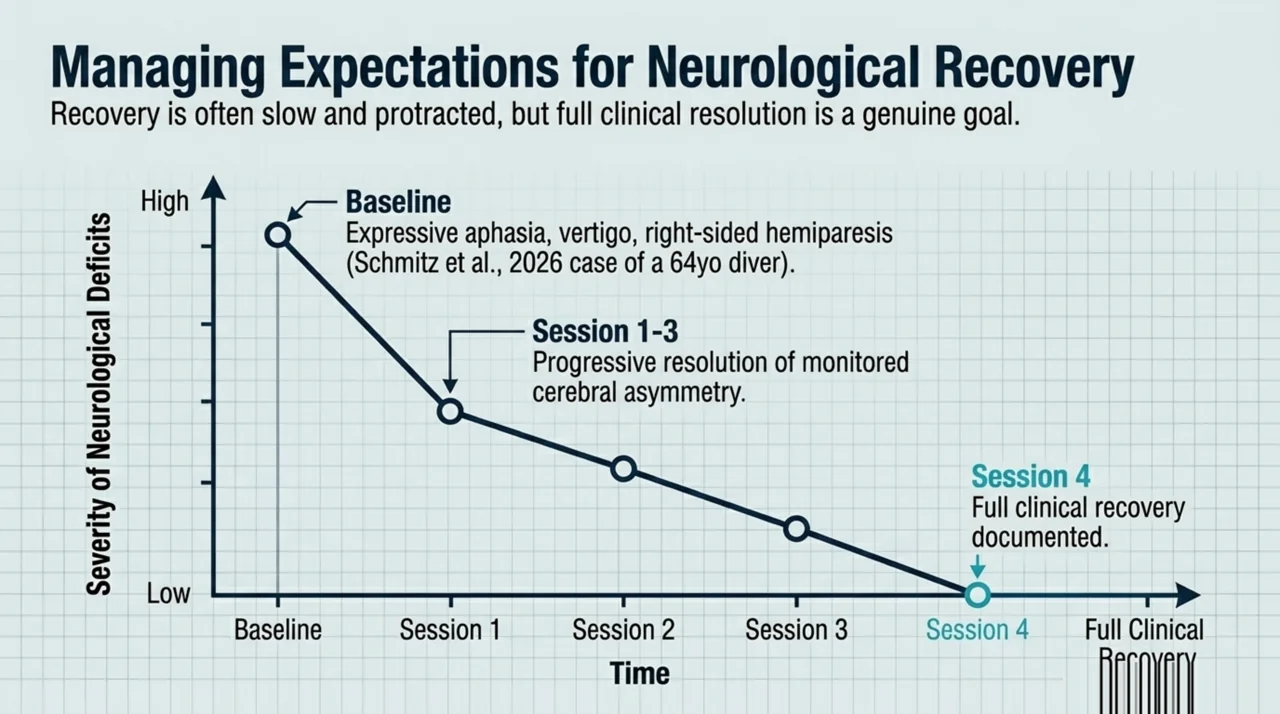
Recovery is possible, but it is rarely instant. The Wijdicks review notes that awakening from coma, improvement of hemiparesis, and good functional outcome may occur after treatment, while cautioning that progress is likely to be slow and protracted. This realistic framing helps physicians counsel families without overpromising. Meaningful neurological recovery is a genuine goal, and the published literature includes reports of substantial improvement even when treatment begins hours after the event.
The closely related diving injury, decompression sickness, offers an encouraging illustration of recovery with recompression. A 2026 case report by Schmitz and colleagues (PubMed) described a 64-year-old diver who developed expressive (Broca’s) aphasia, vertigo, and right-sided hemiparesis 30 to 120 minutes after a rapid ascent. He was treated with hyperbaric oxygen, and the authors report full clinical recovery after four sessions, with the cerebral asymmetry they monitored resolving progressively over three sessions. Decompression sickness and arterial gas embolism are distinct, but both are dysbaric brain injuries treated with recompression, and this case shows how complete the recovery can be when treatment is delivered promptly. You can read more about the diving sibling of this condition on the Canada Hyperbarics decompression sickness resource.
How do Canadian physicians access hyperbaric facilities for an emergency?
Emergency recompression in Canada is delivered through hospital-based hyperbaric programs in several provinces. Because gas embolism is a recognised emergency indication, treatment at these hospital programs is covered by provincial health insurance in the participating provinces, and no private referral pathway is required for the emergency itself. The practical barrier is geography, not coverage: not every hospital has a chamber, and the nearest one may be in another city or province.
For that reason, Canada Hyperbarics recommends that referring physicians know their regional pathway before they need it. The Undersea and Hyperbaric Medical Society lists air or gas embolism among its approved hyperbaric indications, and the Canadian Undersea and Hyperbaric Medicine Association maintains a national perspective on hyperbaric practice, including a directory of Canadian hyperbaric facilities. You can also browse our directory of hospitals and regulated facilities, and explore the wider evidence base in the Canada Hyperbarics research library.
Frequently asked questions about HBOT for arterial gas embolism
Is hyperbaric oxygen therapy the standard treatment for arterial gas embolism?
Yes. Hyperbaric oxygen therapy, delivered as recompression, is the recognised definitive treatment for arterial gas embolism. The Undersea and Hyperbaric Medical Society lists air or gas embolism as a primary hyperbaric indication. Recompression mechanically shrinks gas bubbles and improves oxygen delivery to ischaemic tissue.
How quickly does a patient need to reach a hyperbaric chamber?
As fast as safely possible. The 2026 Wijdicks review recommends hyperbaric oxygen therapy when a facility can be reached within an eight-hour window, and earlier is better. Because chambers are not available at every hospital, contacting the nearest hyperbaric service early is essential so transfer can begin without delay.
What should I do before the patient is transferred?
Keep the patient supine (lying flat) rather than head-down, give high-flow 100% oxygen through a closed mask at 10 to 15 litres per minute or high-flow nasal cannulae up to 60 litres per minute, support the airway and circulation, and call the hyperbaric service early. Current guidance favours supine positioning for arterial gas embolism, since the head-down Trendelenburg position can worsen cerebral oedema; the head-down left lateral decubitus (Durant) position is used for venous air embolism. The oxygen and transfer steps are consistent with the 2026 Wijdicks review on air embolism to the brain.
Can gas embolism happen during routine procedures, not just diving?
Yes. Iatrogenic gas embolism can follow central line insertion or removal, surgery, and contrast-enhanced imaging. Recent 2026 case reports describe embolism after coronary CT contrast injection and during robot-assisted kidney surgery. Any sudden neurological or cardiopulmonary change during or after such a procedure should raise suspicion.
Is the difference between venous and arterial gas embolism important?
Yes. Venous gas embolism usually lodges in the pulmonary circulation and small loads may resolve with high-flow oxygen and positioning. Arterial gas embolism obstructs end-arteries supplying the brain or heart and is treated as a recompression emergency. Both warrant immediate oxygen, but arterial cases need urgent transfer to a chamber.
Is emergency hyperbaric treatment covered in Canada?
Emergency recompression for gas embolism is delivered through hospital-based hyperbaric programs and is covered by provincial health insurance in the participating provinces, since gas embolism is a recognised emergency indication. The main constraint is distance to the nearest chamber, so knowing your regional pathway in advance is valuable.
What outcomes are realistic after treatment?
Outcomes vary with the size of the embolism, the organ affected, and how quickly treatment begins. The Wijdicks review notes that awakening from coma, improvement of hemiparesis, and good functional outcome may occur, though recovery is often slow and protracted. Prompt referral gives the patient the best chance of meaningful neurological recovery.
The bottom line for referring physicians
Arterial gas embolism is rare, but it is a true emergency where the referring physician’s speed shapes the outcome. Keep the diagnosis in mind whenever a patient collapses neurologically after diving or a procedure that can introduce air, start high-flow oxygen and correct positioning immediately, and call your nearest hyperbaric service early. Hyperbaric oxygen therapy is the definitive treatment, and the earlier it begins, the better the window for recovery. To find the closest emergency chamber, consult the directory of hospitals and regulated facilities and review our frequently asked questions on hyperbaric care in Canada.
Medical disclaimer: This content is for informational purposes only and does not constitute medical advice. It is intended to support, not replace, the clinical judgement of qualified health professionals. Always rely on local emergency protocols and direct consultation with a hyperbaric medicine service when managing a suspected gas embolism.