
TL;DR: Hyperbaric oxygen therapy (HBOT) for long COVID has produced conflicting results in the 2024-2026 literature. Two systematic reviews and a large international registry report cognitive, fatigue, and quality-of-life improvements, while a 2025 Swedish placebo-controlled phase II trial (HOT-LoCO) found no benefit over sham at 13 weeks. The evidence base remains immature: small samples, heterogeneous protocols, and inconsistent outcome measures make definitive conclusions premature. Canadian researchers, including the McMaster-led living systematic review team, classify HBOT as an investigational intervention for post-COVID condition.
Hyperbaric oxygen therapy is a medical intervention in which patients breathe 100% oxygen at pressures above one atmosphere absolute, typically 1.5 to 2.4 ATA, inside a sealed chamber. For researchers evaluating long COVID interventions, HBOT sits at an awkward intersection: a strong mechanistic rationale, a growing body of small clinical trials, and a recently published rigorous RCT that did not reproduce earlier positive findings. This evidence review, prepared for a Canadian research audience by Canada Hyperbarics, synthesises the 2024-2026 literature and identifies the key gaps that future trials must address.

Why is HBOT being investigated for long COVID at all?
Long COVID, formally termed post-COVID condition (PCC) in WHO clinical case definitions and post-acute sequelae of SARS-CoV-2 infection (PASC) in much of the U.S. literature, affects an estimated 75 million people globally. The mechanistic rationale for HBOT in this population rests on three converging hypotheses. First, persistent microvascular dysfunction and endothelial injury appear to underlie many long COVID symptoms, particularly cognitive impairment and exercise intolerance. Second, mitochondrial dysfunction has been documented in muscle and immune cells of patients with persistent fatigue. Third, low-grade neuroinflammation and altered cerebral perfusion are detectable on advanced imaging in patients with post-COVID brain fog.
HBOT exposes patients to a hyperoxic-hypoxic paradox that has been shown in pre-clinical models to stimulate angiogenesis, mitigate neuroinflammation, and improve mitochondrial function. The question for clinical researchers is not whether these mechanisms exist but whether they translate to clinically meaningful improvements in patients with heterogeneous, fluctuating long COVID phenotypes.
What does the 2024 living systematic review conclude about HBOT?
The most authoritative synthesis to date is the living systematic review by Zeraatkar and colleagues at McMaster University (PubMed), published in BMJ in November 2024. The McMaster team analysed 24 randomised trials covering 3,695 long COVID patients across drug, rehabilitation, behavioural, dietary, and device-based interventions. Cognitive behavioural therapy and combined physical and mental health rehabilitation showed moderate-certainty evidence of benefit. Among the interventions classified as not having compelling evidence of effect, the authors specifically named hyperbaric oxygen.
This is an important Canadian contribution to the field. The McMaster review uses GRADE methodology and updates as new trials are published, which means its conclusions on HBOT will evolve. As of the December 2023 search cutoff, the included HBOT trials were small, methodologically limited, and did not yet include the placebo-controlled phase II data later reported in 2025.
How did the HOT-LoCO randomised controlled trial change the picture?
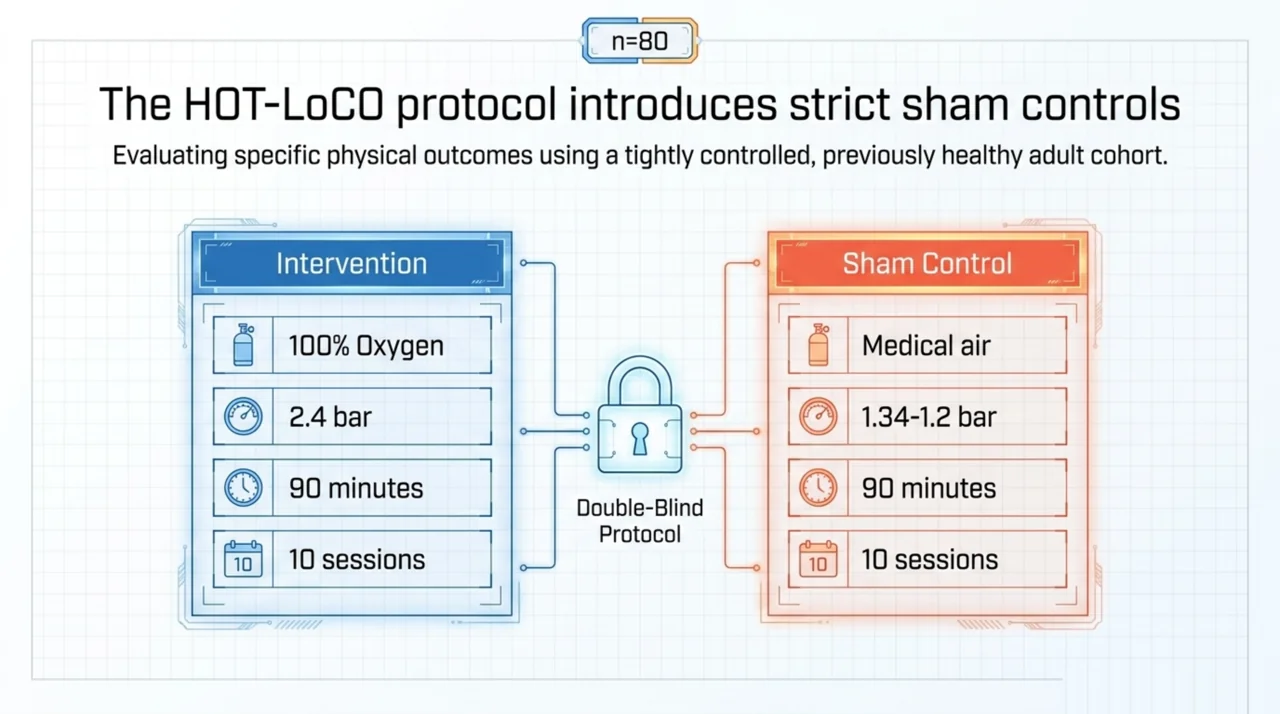
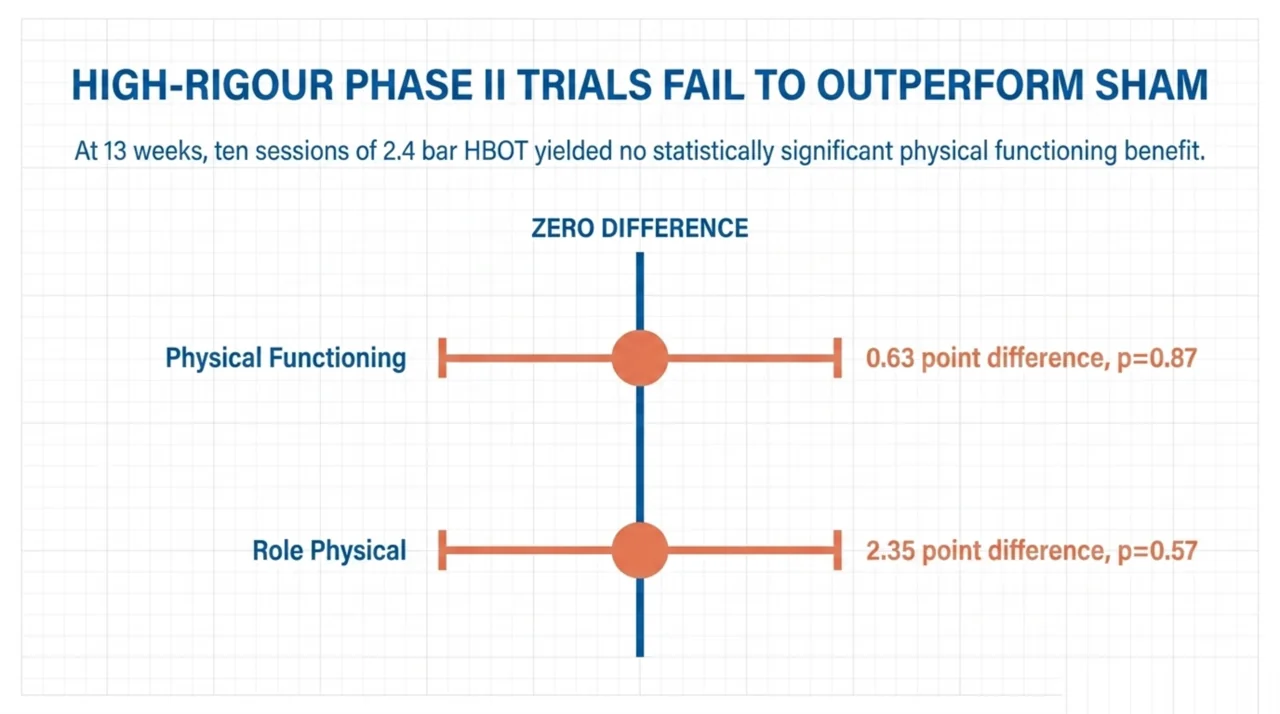
The HOT-LoCO trial (PubMed), published in BMJ Open in April 2025 by Kjellberg and colleagues at the Karolinska Institutet, is the most rigorous long COVID HBOT trial published to date. Eighty previously healthy adults aged 18-60 with diagnosed long COVID were randomised to ten sessions of either HBOT (100% oxygen, 2.4 bar, 90 minutes) or sham (medical air, 1.34-1.2 bar) over six weeks. The primary endpoints were the RAND-36 Physical Functioning and Role Physical subscales at 13 weeks.
The result was negative. Both groups improved from baseline, but the between-group difference in Physical Functioning at 13 weeks was 0.63 points (95% CI -7.04 to 8.29; p=0.87) and in Role Physical was 2.35 points (95% CI -5.95 to 10.66; p=0.57). Adverse events were common in both arms, with cough and chest discomfort predominating, but the trial reported a favourable harm profile overall. One serious adverse event occurred in the HBOT group and one death in the placebo group.
The HOT-LoCO finding diverges from earlier positive open-label and unblinded studies, which is consistent with a pattern seen across many HBOT investigations: effect sizes shrink markedly when proper sham controls and double-blinding are introduced. For Canadian researchers designing the next generation of long COVID HBOT trials, this is a methodological turning point. Any future protocol should plan for a credible sham, validated outcome measures, and statistical power adequate for clinically meaningful effect sizes rather than the large effects implied by uncontrolled case series.
What do the systematic reviews of HBOT for long COVID brain fog show?
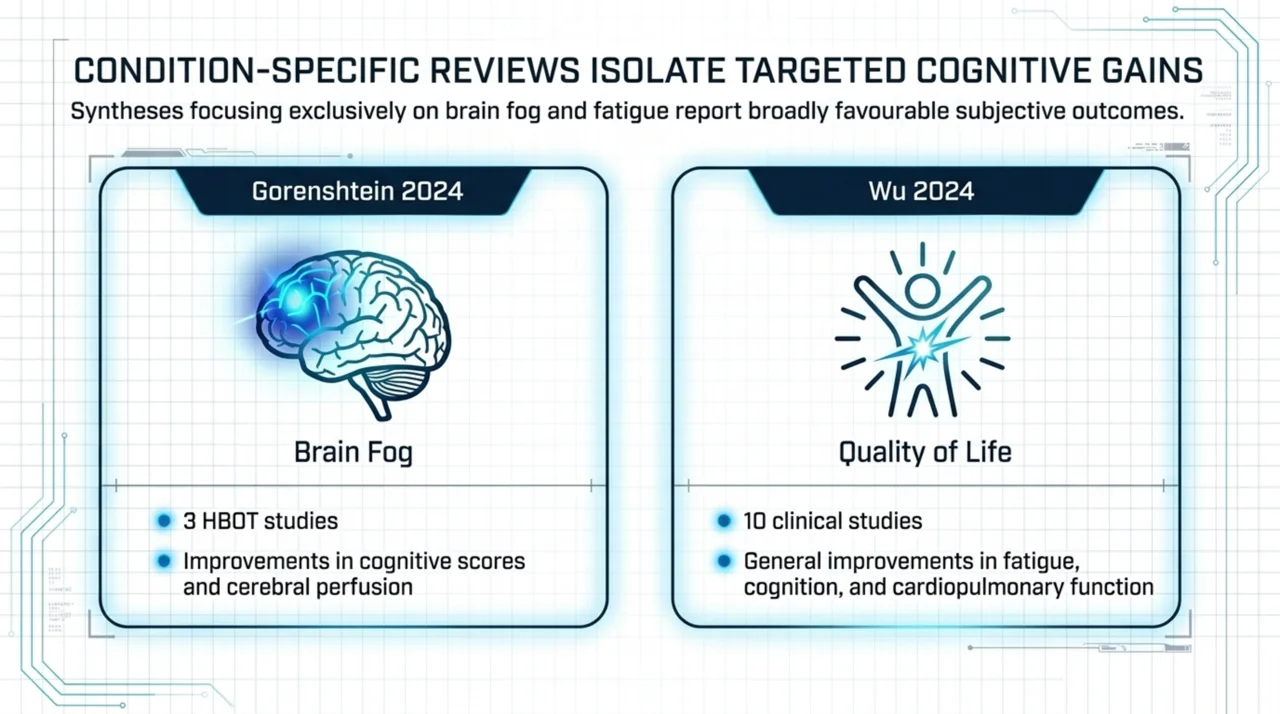
Two condition-specific systematic reviews published in 2024 reach different conclusions than the McMaster pan-intervention review. Gorenshtein and colleagues (2024) (PubMed) reviewed 17 studies of brain fog interventions and identified three HBOT studies, all of which reported improvements in cognitive assessment scores and brain perfusion measures. Wu and colleagues (2024) (PubMed) reviewed ten clinical studies of HBOT for long COVID, including three complete RCTs, and concluded that HBOT generally improved quality of life, fatigue, cognition, and cardiopulmonary function.
Both reviews acknowledge significant methodological limitations: small sample sizes, heterogeneous HBOT protocols ranging from 1.5 to 2.4 ATA, varying session counts from 10 to 60, inconsistent outcome measures, and limited use of credible sham controls. Both call for adequately powered, sham-controlled, multicentre trials before HBOT can be considered an evidence-based therapy for long COVID.
What does the international HBOT registry tell us about long COVID outcomes?
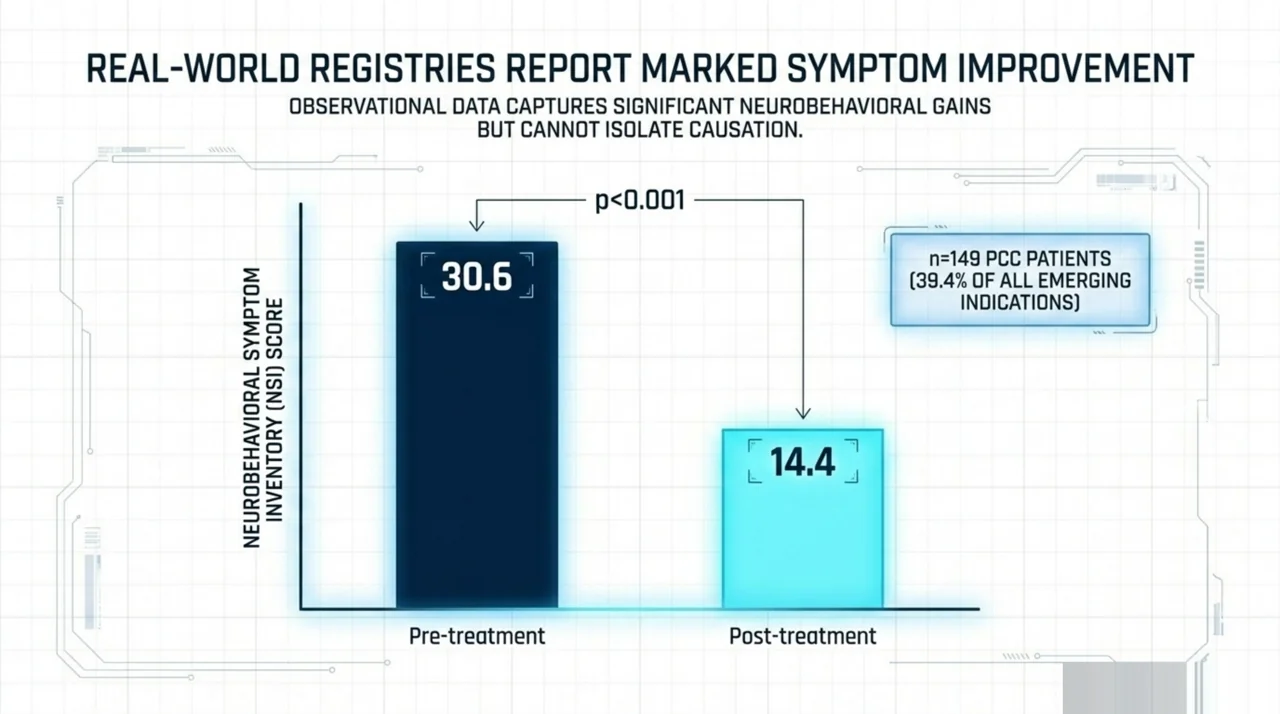
The International Multi-Centre Registry for Hyperbaric Oxygen Therapy (PubMed), reported by Tanaka and colleagues in 2024, captures real-world outcome data from HBOT centres in the United States, United Kingdom, and Australia. Of 9,726 registry entries, 378 patients (3.89%) were treated for emerging indications, and post-COVID condition was the single largest emerging-indication cohort at 149 patients (39.4% of emerging indications). Patients with PCC reported a statistically significant improvement on the Neurobehavioral Symptom Inventory, with mean scores dropping from 30.6 pre-treatment to 14.4 post-treatment (p<0.001).
Registry data has different epistemic weight than randomised trial data. It captures real-world heterogeneity and treatment patterns, but cannot adjudicate causation. The registry signal for PCC is consistent with the open-label literature and is hypothesis-generating rather than confirmatory.
What does the most recent 2026 evidence add?
A March 2026 retrospective study from the Sagol Centre, published in Frontiers in Neurology by Doenyas-Barak and colleagues (PubMed), evaluated Pittsburgh Sleep Quality Index changes after 60 HBOT sessions in three populations: healthy aging adults (n=180), long COVID patients (n=92), and patients with PTSD (n=123). All groups showed statistically significant improvements in total PSQI score (p<0.001; Cohen's d ranging from 0.37 to 0.91). Long COVID patients improved on subjective sleep quality, sleep latency, sleep disturbances, and daytime dysfunction.
This study uses 60 sessions at 2.0 ATA, considerably more than the 10-session HOT-LoCO protocol. The dose-response question is unresolved: it is plausible that long COVID HBOT trials are simply under-treating, and that benefits emerge only at higher session counts. It is equally plausible that the apparent benefit reflects regression to the mean, expectancy effects, or selection bias inherent in retrospective cohort designs. A formal dose-finding RCT in long COVID has not yet been published.
How should the conflicting evidence be interpreted by Canadian researchers?
Three observations help reconcile the apparent contradictions across these studies.
- Protocol heterogeneity is extreme. The published literature includes protocols ranging from 10 sessions at 1.34 ATA to 60 sessions at 2.4 ATA. These are clinically and biologically different exposures. Pooling them in meta-analysis obscures genuine effects in either direction.
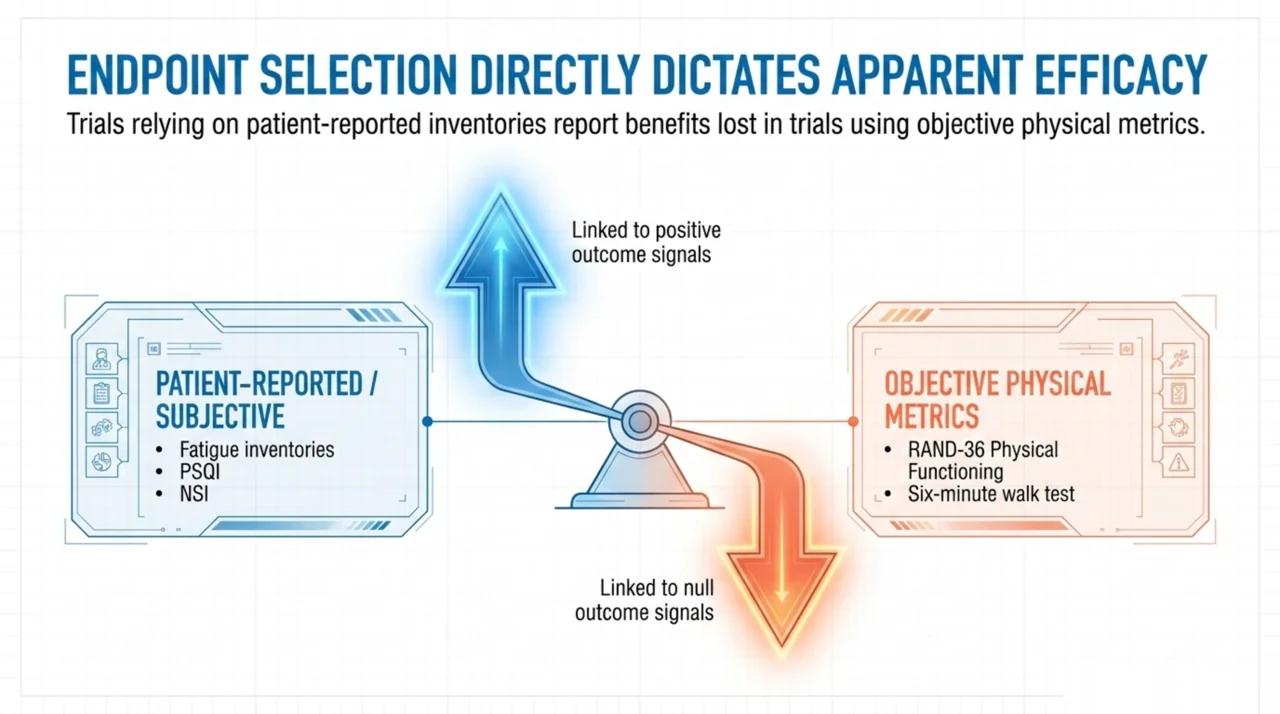
- Outcome measure selection drives apparent effects. Studies relying on patient-reported fatigue or cognitive symptom inventories tend to report benefit. Studies using objective physical-function endpoints, such as the RAND-36 PF subscale or six-minute walk test, tend to report no significant effect over sham.
- Long COVID is not one disease. Subgroups defined by predominant phenotype, including dysautonomia or postural orthostatic tachycardia syndrome, post-exertional malaise, brain fog without fatigue, or cardiopulmonary symptoms, may respond differently to HBOT. Trials that pool all long COVID phenotypes may be diluting any genuine subgroup effect.
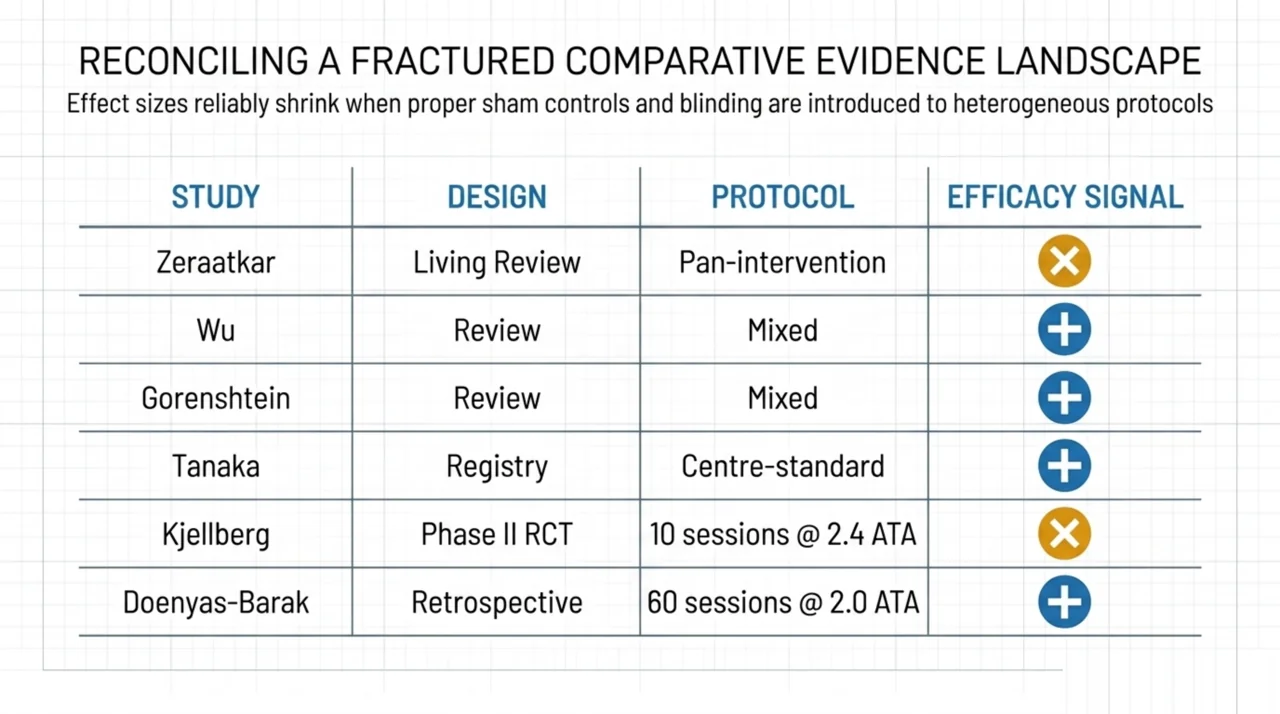
What does the comparative evidence landscape look like?
| Study | Design | n | Protocol | Primary finding |
|---|---|---|---|---|
| Zeraatkar 2024 (McMaster) | Living systematic review | 3,695 across 24 trials | Pan-intervention | HBOT: no compelling evidence |
| Wu 2024 | Systematic review | 10 studies | Mixed protocols | Generally positive on QoL, fatigue, cognition |
| Gorenshtein 2024 | Systematic review (brain fog) | 3 HBOT studies | Mixed protocols | Improvement in cognitive scores and perfusion |
| Tanaka 2024 (registry) | Prospective registry cohort | 149 PCC patients | Standard centre protocols | NSI score 30.6 to 14.4 (p<0.001) |
| Kjellberg 2025 (HOT-LoCO) | Phase II RCT, double-blind | 80 | 10 sessions, 2.4 ATA | No difference vs sham at 13 weeks |
| Doenyas-Barak 2026 | Retrospective cohort | 92 long COVID | 60 sessions, 2.0 ATA | PSQI improvement, p<0.001 |
What are the priority research gaps for Canadian investigators?
Canada has substantial unmet capacity to contribute to this field. The McMaster living systematic review represents methodological leadership, but Canadian investigator-initiated trials of HBOT in long COVID remain limited. Five gaps stand out:
- Dose-finding studies. No published trial has formally compared session counts of 20 versus 40 versus 60 in the same long COVID population. Without dose-finding data, future phase III trials risk repeating HOT-LoCO’s likely under-dosing.
- Phenotype-stratified trials. Long COVID with predominant POTS, predominant cognitive dysfunction, or predominant fatigue are clinically distinct. Stratified randomisation or restricted enrolment may detect signals lost in mixed-phenotype trials.
- Objective biomarker outcomes. Cerebral perfusion on arterial spin labelling MRI, mitochondrial respiratory capacity, and circulating inflammatory cytokines should be incorporated alongside patient-reported outcomes to identify mechanistic responders.
- Sham fidelity assessment. Several published trials use sham protocols that may not be credible to enrolled patients. Future trials should formally assess blinding success and report it transparently.
- Health-economic modelling. If a real but modest effect exists, the cost per quality-adjusted life year for HBOT in long COVID has not been modelled in a Canadian context. CIHR-funded health-economic work would inform any future provincial coverage decision.
Frequently asked questions from researchers
Is HBOT a recognised indication for long COVID?
No. Long COVID is not on the Health Canada list of recognised conditions or the Undersea and Hyperbaric Medical Society (UHMS) Indications list for hyperbaric oxygen therapy. Use for this indication is investigational. See our regulatory overview for the current Health Canada list of recognised conditions and the conditions index for evidence summaries on recognised conditions.
Are there active Canadian clinical trials of HBOT for long COVID?
As of April 2026, ClinicalTrials.gov lists no actively recruiting Canadian-sponsored randomised trials of hyperbaric oxygen therapy specifically for long COVID. Canadian sites are listed as participants in international observational registries, including the registry described in Tanaka et al. 2024.
What is the most rigorous published trial of HBOT for long COVID?
The HOT-LoCO trial by Kjellberg and colleagues, published in BMJ Open in 2025, is currently the most methodologically rigorous published study. It used double-blinding, a credible sham, intention-to-treat analysis, and pre-specified primary endpoints. The trial reported no benefit of HBOT over sham at 13 weeks.
Does the negative HOT-LoCO result rule out HBOT for long COVID?
No. HOT-LoCO tested a specific protocol, ten sessions at 2.4 bar, in a specific population of previously healthy adults. The trial does not address higher-dose protocols, longer follow-up, or specific long COVID phenotypes. It establishes that the tested protocol does not improve physical functioning above sham at three months.
Where can I find Canadian facility-level data for studies?
Canada Hyperbarics maintains an open registry of Canadian hospitals and regulated facilities offering hyperbaric oxygen therapy, including chamber types and indications treated. The dataset is available via our JSON API under a CC-BY-4.0 licence for academic use.
What outcome measures are most commonly used in HBOT long COVID trials?
The most frequently reported outcomes are RAND-36 or SF-36 quality-of-life subscales, the Pittsburgh Sleep Quality Index, the Neurobehavioral Symptom Inventory, the six-minute walk test, computerised cognitive assessment batteries, and patient-reported fatigue scales. Standardisation across trials remains poor.
What proportion of HBOT use is for emerging indications like long COVID?
According to the Tanaka 2024 international registry, 3.89% of registry entries were for emerging indications. Within that emerging-indication subset, post-COVID condition accounted for 39.4%, making it the single largest emerging-indication category, ahead of inflammatory bowel disease, calciphylaxis, and frostbite.
Conclusion: HBOT for long COVID remains an investigational therapy
The 2024-2026 evidence base does not yet support a definitive judgment for or against HBOT in long COVID. The most rigorous controlled trial reports no benefit at the tested dose. Larger registry datasets and condition-specific systematic reviews suggest meaningful improvements that may reflect a real but modest effect, expectancy bias, or selection effects. The path forward is not more underpowered open-label studies. It is dose-finding, phenotype-stratified, sham-controlled trials that incorporate objective biomarkers and report blinding fidelity. Canada has the methodological infrastructure to lead this work, and Canadian researchers are encouraged to engage with the international consortia driving the next generation of long COVID intervention trials.
Canada Hyperbarics curates open data on Canadian facilities, an indexed library of HBOT studies, and provincial coverage information for investigators and clinicians. For protocol design support and access to our facility registry, see the research library and about pages. To find Canadian hospitals and regulated facilities by province, see the facilities directory.
This content is for informational purposes only and does not constitute medical advice. Hyperbaric oxygen therapy for long COVID is investigational and is not currently a recognised indication. Patients considering HBOT should consult a qualified physician at one of Canada’s hospitals and regulated facilities. Always verify current evidence directly with primary sources before clinical or research decisions.