
Hyperbaric oxygen therapy (HBOT) is a medical treatment in which a patient breathes pure oxygen inside a pressurised chamber. This Canadian patient and family guide explains how HBOT relates to traumatic brain injury (TBI): what the current research actually shows, what care looks like in 2026, what it costs, and how to ask the right questions before you commit to treatment.
TL;DR. Traumatic brain injury is not one of the 14 conditions that Health Canada has licensed hyperbaric chambers to treat, and it is not on the Undersea and Hyperbaric Medical Society’s approved indications list. HBOT for TBI is still considered investigational. A 2026 comprehensive review of the recent literature reported mixed outcomes: some studies described cognitive and clinical improvements, while others raised concerns about methodology and reproducibility. Standard TBI rehabilitation should come first. If you are considering HBOT, the right path is to talk to your physician, understand the evidence honestly, and choose a regulated Canadian facility that screens patients carefully.
What is hyperbaric oxygen therapy, and how is it used for brain injury?
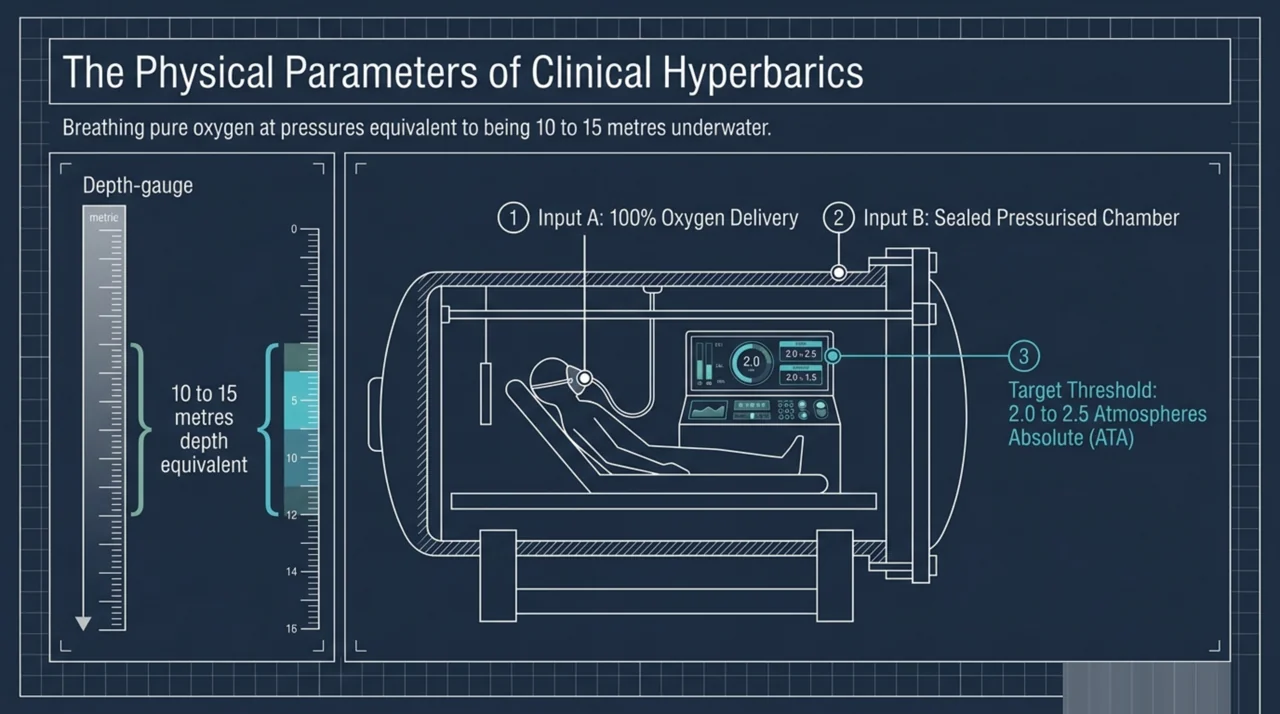
Hyperbaric oxygen therapy is a medical treatment in which a person breathes 100 percent oxygen inside a sealed chamber at a pressure higher than normal sea level air pressure. Most clinical HBOT in Canada is delivered at around 2.0 to 2.5 atmospheres absolute (ATA), which is roughly the pressure you would feel about 10 to 15 metres underwater. A typical session lasts 60 to 90 minutes, and treatment courses range from a few sessions for acute conditions to 30 to 40 sessions for chronic ones.
The reason researchers have been interested in HBOT for traumatic brain injury is that the physics of the treatment can dramatically increase the amount of oxygen dissolved in the blood. In theory, more oxygen reaching injured brain tissue could support repair processes such as new blood vessel growth (angiogenesis), reduced inflammation, and improved energy production inside cells. A 2026 review of HBOT in neurosurgery noted that hyperbaric oxygen has been described as having positive effects on craniocerebral trauma, cerebrovascular diseases, intracranial infections, and intracranial tumours (Wang, 2026; PubMed | Our Assessment).
That said, the gap between a plausible mechanism and a proven benefit in real patients is large. Showing that HBOT works for TBI in a way that matters to everyday life (better thinking, better mood, fewer headaches, more independence) requires careful clinical trials. That is where the picture gets more complicated.
Is HBOT an approved treatment for traumatic brain injury in Canada?
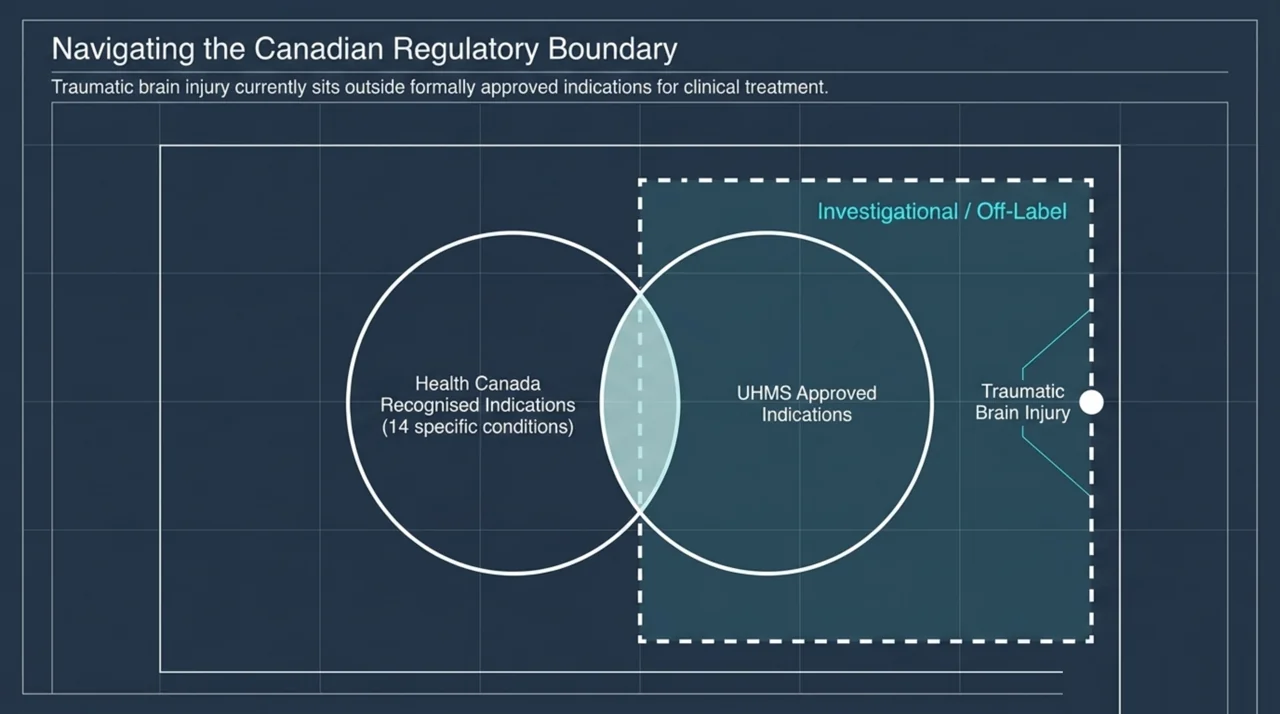
No. Traumatic brain injury is not on the list of conditions Health Canada has licensed hyperbaric chambers to treat. According to Health Canada’s public guidance, hyperbaric chambers in Canada are Class 3 medical devices that must be licensed before they can be imported and sold, and Health Canada has issued licences only for 14 specific indications. TBI is not one of them.
TBI is also not on the Undersea and Hyperbaric Medical Society (UHMS) approved indications list, which is the standard reference North American hyperbaric programmes use to decide which conditions qualify for clinical HBOT. Use of HBOT for TBI in Canada is therefore considered “off-label” or investigational. That does not mean it is illegal, and it does not mean the science is hopeless. It does mean two important things for patients and families:
- Provincial health insurance plans will not pay for HBOT sessions when the indication is TBI.
- The treatment is delivered without the formal regulatory backing it has for recognised indications (such as carbon monoxide poisoning, decompression sickness, certain non-healing wounds, and a short list of others).
Hospital-based hyperbaric programmes in Canada generally focus on recognised indications. A patient seeking HBOT for TBI in 2026 is almost always doing so at a private, regulated facility, paying out of pocket or through certain extended health benefits. Our national directory of hospitals and regulated facilities shows which programmes exist in each province.
What does the research actually show for HBOT in TBI?
This is where families need a clear-eyed summary, because there is a lot of marketing in this space.
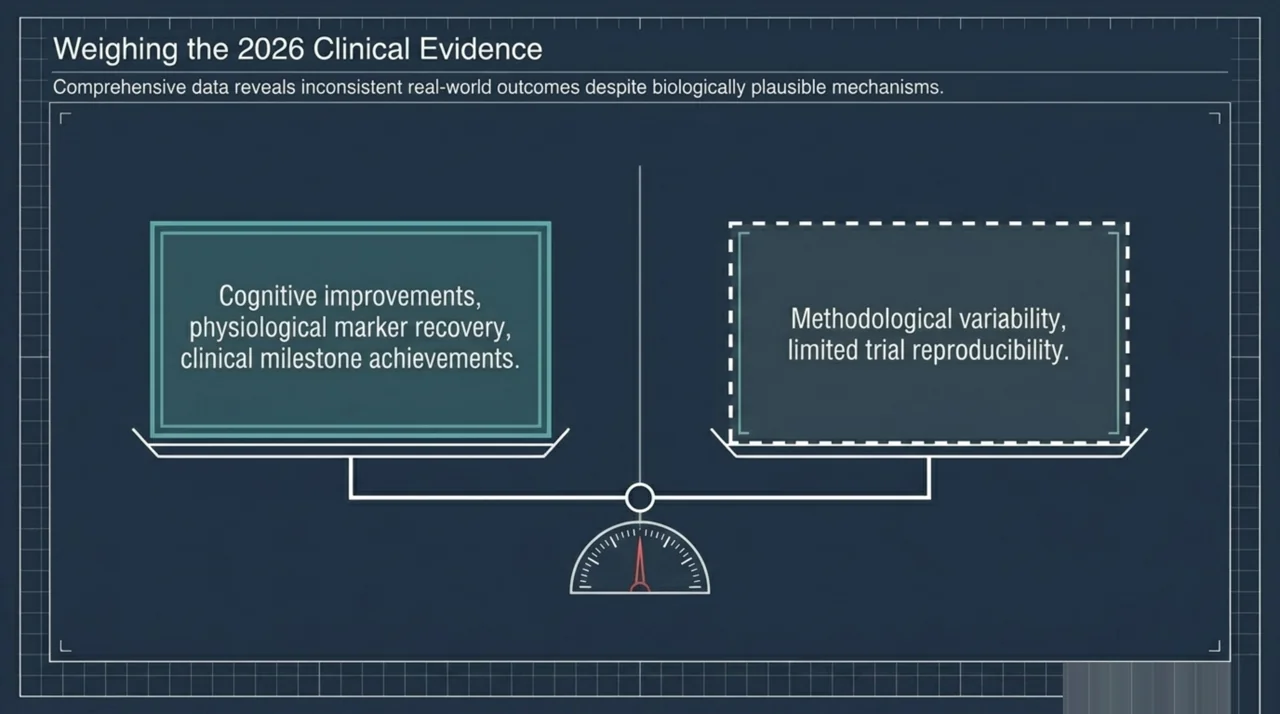
A 2026 comprehensive review in Undersea and Hyperbaric Medicine looked at studies of HBOT for TBI published between 2015 and 2024 (Jusoh and colleagues, 2026; PubMed | Our Assessment). The headline finding was mixed outcomes. Some studies in the dataset reported significant improvements in cognition, in physiological markers, and in clinical recovery measures. Other studies raised concerns about methodological variability and limited reproducibility. The mechanism work was more consistent: HBOT was linked to changes in inflammation-related and growth-related cellular pathways (such as TLR4/NF-kB and VEGF/ERK) that could plausibly support neuroprotection, new blood-vessel growth, and the formation of new connections between brain cells.
In plain language: there are biological reasons to think HBOT might help injured brain tissue, and there are individual patients who appear to improve. But the body of clinical research is not consistent enough yet for major regulators or hyperbaric societies to call HBOT a proven treatment for TBI.
A 2026 broad review of HBOT in hypoxia-related conditions reached a similar conclusion. It described HBOT as providing neuroprotection following central nervous system trauma, while emphasising that current applications are guided by evidence-based protocols set by international hyperbaric medicine associations such as the UHMS (Bhargava and colleagues, 2026; PubMed | Our Assessment). Translation: the mechanism is interesting, but the formal indication list is what governs day-to-day clinical use.
There is also one promising signal that is more specific. Sleep problems are common after TBI and they are one of the things HBOT has been studied for most carefully. A 2026 systematic review and network meta-analysis of 22 randomised controlled trials in 1,299 patients with sleep disorders following TBI reported that several non-drug therapies, including HBOT, were associated with significant improvements in sleep quality measures compared with control treatments (Wang and colleagues, 2026; PubMed | Our Assessment). A separate 2026 systematic review and meta-analysis of non-pharmacologic therapies for post-TBI sleep disturbances similarly included HBOT among the interventions evaluated, alongside cognitive behavioural therapy, blue-wavelength light therapy, and transcranial magnetic stimulation (Loong and colleagues, 2026; PubMed | Our Assessment).
Finally, large adaptive trials are still trying to settle the question of whether HBOT changes important clinical outcomes after acute TBI. The Hyperbaric Oxygen Brain Injury Treatment (HOBIT) trial is one such effort, and a 2026 methodology paper describes how the trial uses Bayesian predictive power to handle interim looks at the data while protecting blinding (Gajewski and colleagues, 2026; PubMed | Our Assessment). The headline take-away for patients is not the statistics; it is that researchers are still actively trying to answer the question and the verdict is not in yet.
How is HBOT for TBI usually delivered?
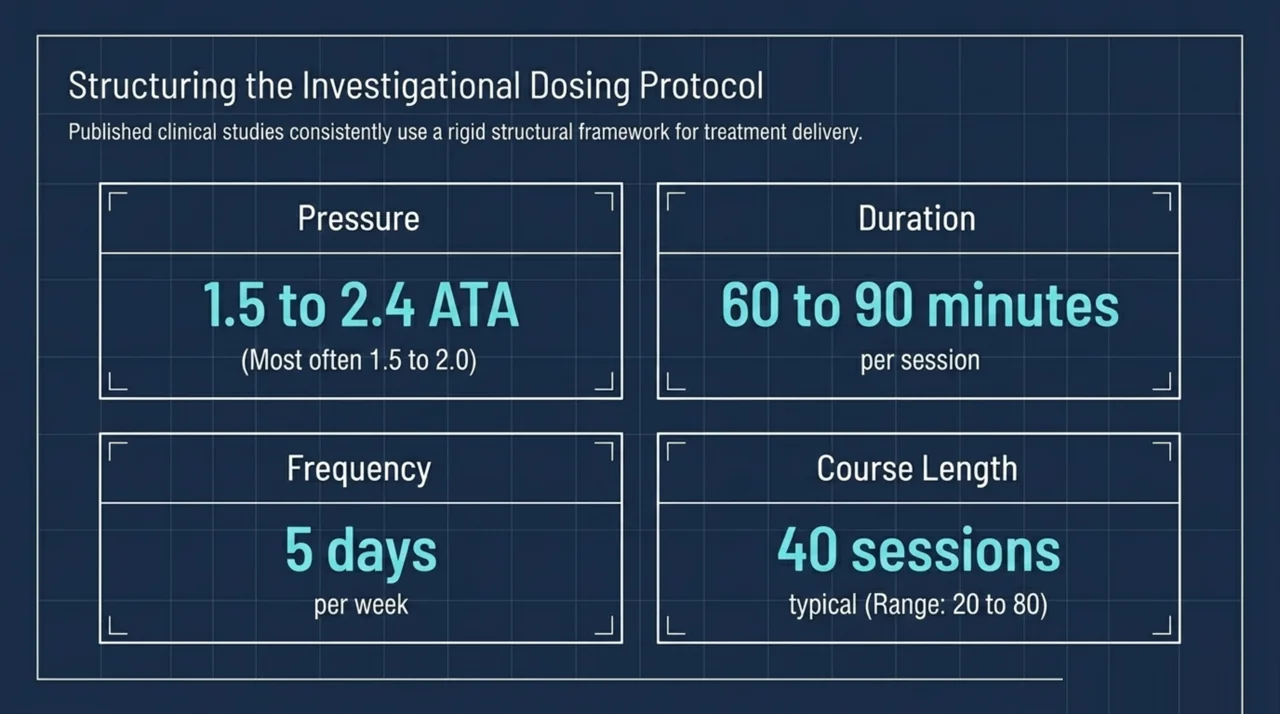
Protocols vary considerably between studies and facilities, but most published TBI work uses some version of the following pattern.
| Element | Typical range in TBI research |
|---|---|
| Chamber pressure | 1.5 to 2.4 ATA (most often 1.5 to 2.0 ATA) |
| Oxygen breathing time | 60 to 90 minutes per session |
| Frequency | 5 days per week |
| Course length | 40 sessions in many protocols (range 20 to 80) |
| Setting | Regulated outpatient facility, monoplace or multiplace chamber |
| Cost in Canada | Out of pocket; not covered by provincial health plans |
If a clinic is offering you something dramatically different from this (for example, very high pressures, very long sessions, or treatment of a child without close medical screening), that is a reason to slow down and ask more questions. A complete patient-screening pathway is the single most important quality marker for a hyperbaric clinic. We discuss screening in more detail in our master FAQ.
What does an HBOT session feel like?
For someone with TBI, the experience inside the chamber is the same as for any other patient. You change into cotton scrubs (no synthetic fabrics, no perfumes, no electronics, no lighters), enter the chamber, and the pressure is slowly increased over about 10 to 15 minutes. Your ears will feel similar to descending in an airplane and you will be coached on how to clear them. Once you reach treatment pressure, you breathe pure oxygen for the prescribed time, usually with one or two short “air breaks” to reduce the small risk of oxygen toxicity. The chamber is then slowly depressurised. Many patients read, sleep, or watch screens visible outside the chamber during sessions.
For more detail on the experience, see our patient overview of what conditions HBOT is used for in Canada and our general frequently asked questions.
What are the risks for someone with a brain injury?
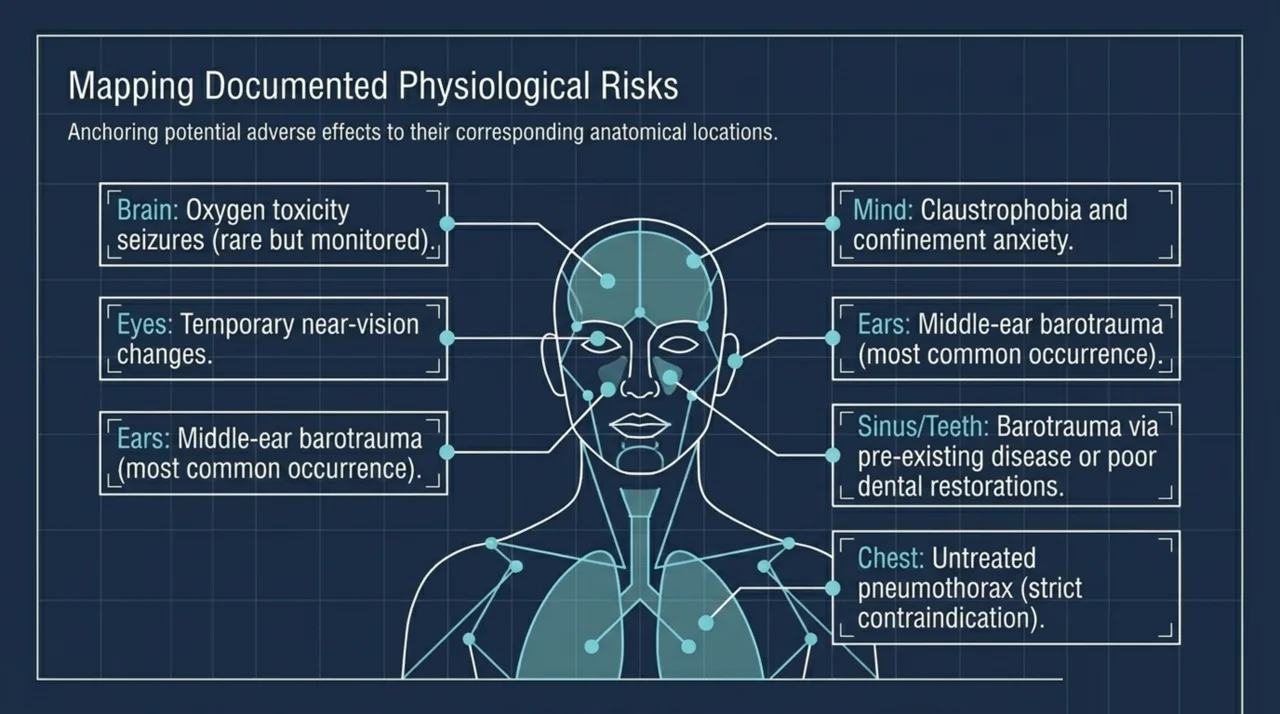
HBOT, when delivered in a regulated facility with proper screening, has a strong safety record for its recognised indications. Most side effects are mild and temporary. Common ones include:
- Ear discomfort or middle-ear barotrauma. The most common side effect. Risk is reduced by teaching patients to equalise their ears and by going slowly through pressure changes. People with sinus congestion or a recent cold may need to delay treatment.
- Temporary near-vision changes. Some patients experience a small shift in vision over a long course of treatment. This usually returns to baseline within weeks to months after stopping HBOT.
- Claustrophobia or anxiety. Multiplace chambers (which fit several patients at once) often feel less confining than monoplace chambers. Staff coaching helps.
- Oxygen toxicity seizures. Rare at the pressures used clinically, but a real risk. Properly trained facilities monitor for warning signs and use scheduled air breaks.
- Sinus or dental barotrauma. Less common, but possible if there is pre-existing sinus disease or a poorly sealed dental restoration.
Some TBI patients have specific factors that need extra attention. Seizure history, untreated pneumothorax, certain heart and lung conditions, and some medications (for example, particular chemotherapy drugs) can be reasons to delay or avoid HBOT. A complete medical history and physical examination by an HBOT-trained physician should happen before any treatment.
Should patients try HBOT for traumatic brain injury?
This is the question every family asks, and there is no single right answer. What we can offer is a framework.
- Standard care comes first. Evidence-based TBI rehabilitation (cognitive therapy, physiotherapy, occupational therapy, mental-health care, vision rehabilitation, sleep treatment, and well-managed medications) has the strongest evidence base for improving function after brain injury. Make sure you have access to a coordinated team before adding anything else.
- Talk to your own physician. Your treating doctor or neurologist knows your full medical history. They are the right person to weigh in on whether HBOT is reasonable for you, what to ask, and what to watch for. Bring this article and the research links above to the conversation.
- Understand that this is investigational. If you proceed with HBOT for TBI, you are choosing an off-label treatment with mixed evidence. That can still be a reasonable choice, especially if standard care has plateaued, but go in with clear expectations.
- Choose a regulated facility. In Canada, HBOT should be delivered in a facility using a Health Canada-licensed hard-shelled chamber, with physician oversight, trained operators, written safety protocols, and proper screening. Avoid unlicensed soft-shell chambers used at home for medical reasons.
- Set milestones. Decide in advance what improvement would justify continuing. Many TBI protocols include a re-evaluation point at 20 to 40 sessions. If nothing has changed, that is meaningful information.
How is HBOT for TBI covered (or not) by Canadian insurance?
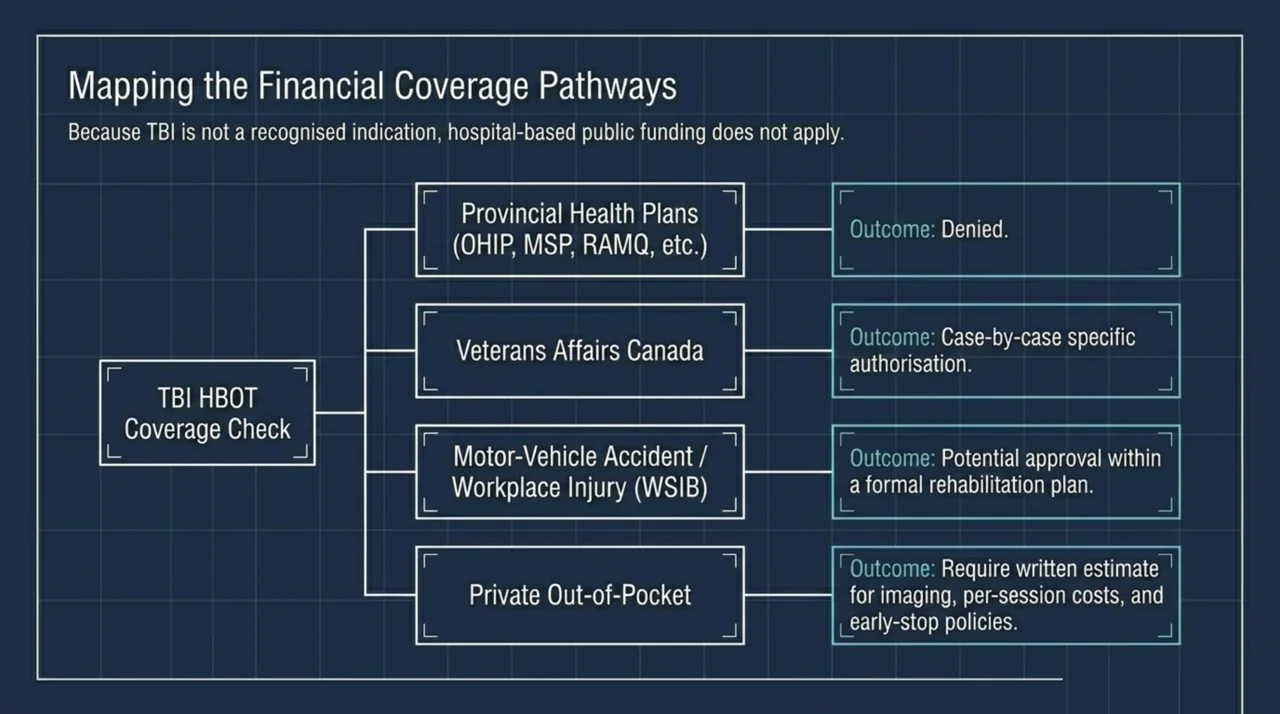
Because TBI is not a licensed Health Canada indication, provincial health insurance plans (Ontario’s OHIP, British Columbia’s MSP, Alberta’s AHCIP, Manitoba Health, Saskatchewan Health, Quebec’s RAMQ, Nova Scotia’s MSI, New Brunswick Medicare, PEI Health, Newfoundland’s MCP, and the territorial plans) do not pay for HBOT sessions for traumatic brain injury. Hospital-based hyperbaric programmes treat recognised indications under public funding; TBI is treated, when it is treated, in private facilities.
Some patients are able to access HBOT through:
- Veterans Affairs Canada benefits in specific cases
- Motor-vehicle accident insurance coverage where the TBI was acquired in a covered collision
- Long-term disability or workplace injury (WSIB and equivalent provincial bodies) where HBOT is approved as part of a rehabilitation plan
- Some private extended-health-benefit policies (rare and usually capped)
If you are paying out of pocket, ask the facility for a written cost estimate that includes any required pre-treatment imaging and assessments, the per-session price, the total expected number of sessions, and the policy if you need to stop early. For more on coverage by province, see our Canadian coverage overview.
How can I find a hyperbaric facility in Canada?
Canada Hyperbarics maintains a national directory of hospitals and regulated facilities across the country. Hospital-based programmes accept patients with Health Canada-recognised indications, and private facilities accept patients across a wider range of conditions, including investigational ones such as TBI. The directory is independent: we list every regulated facility we can verify, and we do not steer patients to any one of them.
When you contact a facility, useful questions include:
- Is your chamber Health Canada-licensed, and is it a hard-shelled medical-grade unit?
- Who is the supervising physician, and how are they trained in hyperbaric medicine?
- What is your full screening protocol before starting treatment?
- What is your emergency procedure for events such as oxygen toxicity, claustrophobia, or chamber pressure problems?
- How many sessions do you recommend for TBI, and at what point will we reassess?
- What is the total cost, and are any portions invoiced in a way that an insurer might reimburse?
What about Brain Injury Canada and other support organisations?
For broader support, education, and connection with other families navigating brain injury in Canada, Brain Injury Canada is a national charitable organisation that has been providing resources for the brain injury community. Provincial brain-injury associations run support groups, education sessions, and family services. These groups do not endorse HBOT and they do not oppose it; they help you and your family build a wider support system around whatever care plan you choose.
Frequently asked questions about HBOT for traumatic brain injury
Is HBOT for TBI covered by OHIP, MSP, or other provincial plans?
No. Because traumatic brain injury is not one of the conditions Health Canada has licensed hyperbaric chambers to treat, provincial health insurance plans across Canada do not pay for HBOT for TBI. Hospital-based programmes treat recognised indications under public funding.
How many sessions of HBOT are needed for traumatic brain injury?
Published protocols vary. Many TBI studies use 40 sessions delivered five times per week, at pressures between 1.5 and 2.0 atmospheres absolute, with sessions lasting 60 to 90 minutes. Some protocols are shorter (20 sessions) and some are longer (60 to 80). Ask any clinic to share their specific protocol and the milestone at which they will reassess your progress.
Is mild hyperbaric oxygen therapy (mHBOT) the same as clinical HBOT?
No. Mild HBOT, often delivered in soft-shelled chambers at pressures around 1.3 atmospheres, is not the same therapy. Health Canada has not licensed any soft-shelled hyperbaric chambers for sale in Canada, meaning they have not been evaluated for safety, quality, or effectiveness as medical devices. Clinical hyperbaric research in TBI is mostly conducted at pressures of 1.5 atmospheres or higher in hard-shelled chambers.
Could HBOT make my brain injury worse?
Serious harm from HBOT in a properly screened patient at a regulated facility is uncommon. The most relevant risks for a person with TBI are seizure threshold considerations, anxiety and claustrophobia, and ear-related pressure problems. A thorough screening visit before treatment, including a complete medication review, is the best protection.
How long after a brain injury can I start HBOT?
This is not standardised. Some research has studied HBOT relatively soon after acute injury; other work has tested it in patients years out from their injury who had reached a recovery plateau. Talk to your treating clinician about timing; there is no published “must start within X weeks” rule for TBI, partly because the indication itself is not formally approved.
Does HBOT help post-concussion symptoms?
Concussion is a form of mild traumatic brain injury, and the same overall picture applies: mixed evidence, no Health Canada approval, ongoing research. Our separate concussion patient FAQ goes into more detail on that specific question.
What signs should make me stop a course of HBOT?
New or worsening seizures, persistent ear pain that does not resolve, significant vision changes beyond a small refractive shift, claustrophobia that does not settle with coaching, and any sense that your symptoms are getting consistently worse rather than better. Report all of these to your treating clinician promptly.
Is Canada Hyperbarics a clinic?
No. Canada Hyperbarics is an independent Canadian information resource that maintains a national directory of hospitals and regulated facilities, summarises HBOT research, and helps patients navigate the field. We do not provide treatment ourselves and we do not steer patients to specific clinics. Read more about Canada Hyperbarics.
Bottom line for patients and families considering HBOT for TBI
HBOT for traumatic brain injury sits in a particular zone of medicine: biologically plausible, intermittently encouraging in the research, but not yet established to the satisfaction of Health Canada, the UHMS, or most public payers. Some patients will encounter strong testimonials and aggressive marketing. Others will hear blanket dismissals. Neither extreme matches the careful picture that the 2026 reviews actually draw: mixed clinical evidence, real mechanistic interest, ongoing trials, and a clear consensus that the field is still being worked out.
If you decide to explore HBOT, do it as one element of a broader, well-rehabilitated TBI recovery plan, at a regulated Canadian facility, with clear milestones and honest expectations. Bring this guide and its citations to your physician, ask the screening and protocol questions above, and use the Canada Hyperbarics national directory of hospitals and regulated facilities to find a unit that meets the standards in this article.
This content is for informational purposes only and does not constitute medical advice. Hyperbaric oxygen therapy for traumatic brain injury is considered investigational in Canada. Always discuss treatment decisions with your own physician.