
TL;DR: Hyperbaric chamber air quality is the purity of the compressed breathing air supplied to a chamber, and it is one of the most important safety systems a Canadian hyperbaric clinic owns. Clean air means no carbon monoxide, oil mist, excess moisture, or other contaminants reaching the patient. Canadian and international standards (CSA Z180.1, CSA Z275.1, ASME PVHO-1, and Health Canada medical device rules) set the requirements. This guide explains the contaminants that matter, the standards that apply, how to test your gas supply, and how pressure changes the way gases behave once the chamber is sealed.
Hyperbaric chamber air quality is the measure of how clean and contaminant-free the compressed breathing air supplied to a hyperbaric chamber is. For a Canadian clinic owner, it is not a background detail. It is a frontline safety control. When a patient breathes oxygen or air under pressure, any contaminant in that gas is delivered to the lungs more efficiently and at a higher dose than it would be at the surface. A small impurity that would be harmless in room air can become a genuine hazard at depth. At Canada Hyperbarics, we treat breathing air quality and compressed gas handling as core operational topics, on the same level as fire safety and emergency procedures.
This guide is written for clinic owners and operators. It covers what air quality means, which standards apply in Canada, why carbon monoxide is the contaminant of greatest concern, how to test and monitor your gas supply, and how pressure itself changes gas delivery inside the chamber. The goal is practical: a clear mental model and a checklist you can use to build or audit your own air-quality program.
What is hyperbaric chamber air quality, and why does it matter?
Compressed breathing air is ordinary atmospheric air (about 21 percent oxygen, 78 percent nitrogen) that has been compressed, filtered, and dried so it is safe to breathe. Air quality refers to how well that air meets defined purity limits. The contaminants that matter most in a hyperbaric setting are carbon monoxide, carbon dioxide, condensed oil and hydrocarbons, water vapour, and any noticeable odour. Each one has a specific limit set out in the applicable standards.
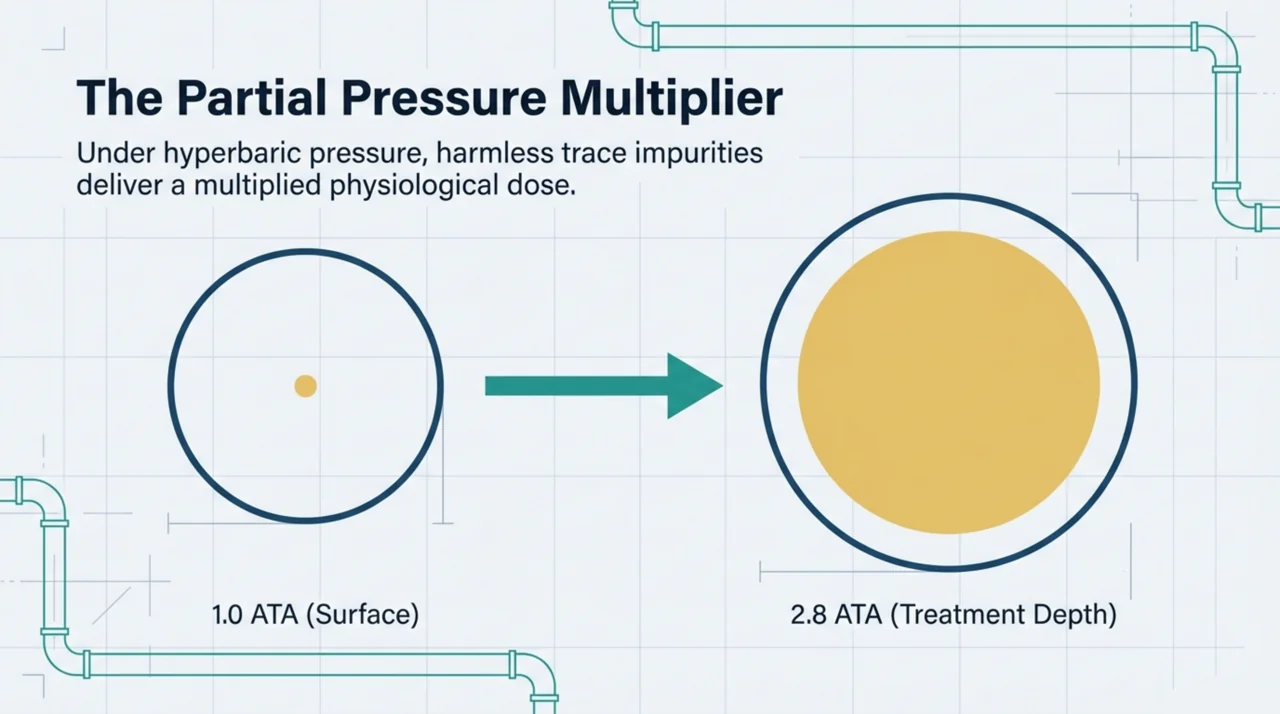
The reason these limits exist is straightforward. Under pressure, the partial pressure of every gas the patient breathes rises. A trace of carbon monoxide that is barely measurable at surface pressure delivers a far larger effective dose at 2.0 to 2.8 atmospheres absolute. Oil mist drawn in from a poorly maintained compressor can irritate the airways. Excess moisture promotes microbial growth in the air system and corrodes components. Clean, dry, contaminant-free air is therefore not a luxury. It is the baseline condition for safe treatment.
Which standards govern compressed breathing air in Canadian hyperbaric clinics?
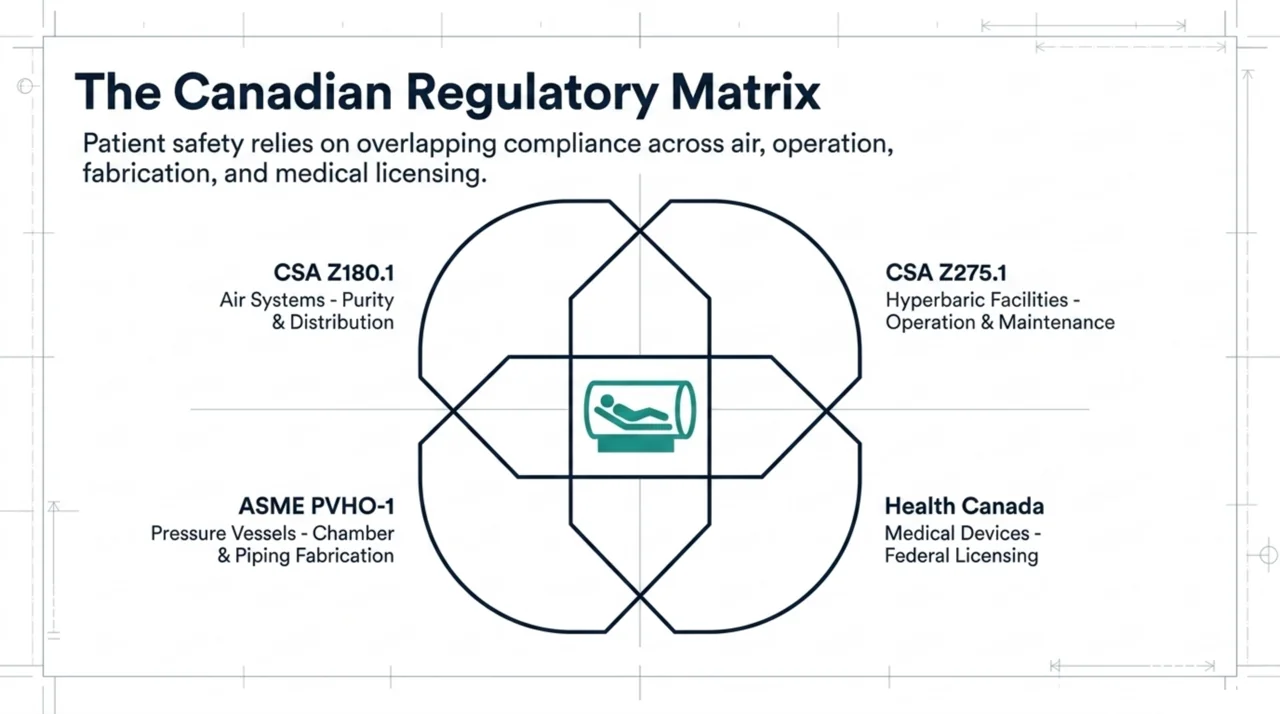
Several standards and regulations overlap to govern the air a Canadian hyperbaric facility delivers. The most directly relevant is CSA Z180.1, Compressed breathing air and systems, which sets the minimum purity requirements for compressed breathing air supplied to a service outlet, and covers the design, testing, operation, and maintenance of the systems that produce, store, and distribute it. Chamber operation itself falls under CSA Z275.1, Hyperbaric facilities, which establishes minimum requirements for the operation, design, construction, maintenance, and testing of hyperbaric chambers.
The chamber as a pressure vessel is built to ASME PVHO-1, the Safety Standard for Pressure Vessels for Human Occupancy, which also covers the piping systems that carry gas into and out of the vessel. On the regulatory side, a medical hyperbaric chamber is a licensed medical device in Canada. Most chambers fall into the moderate-to-high risk classes, so they require a licence under Health Canada medical device licensing. Facilities that pursue accreditation can also follow the UHMS Hyperbaric Facility Accreditation program, which includes environmental controls and gas-safety requirements in its survey.
| Standard or rule | Issuing body | What it governs | Why it matters to a clinic |
|---|---|---|---|
| CSA Z180.1 | CSA Group | Purity of compressed breathing air and the systems that produce, store, and distribute it | Sets the contaminant limits your air must meet and how the supply system is tested and maintained |
| CSA Z275.1 | CSA Group | Operation, design, construction, maintenance, and testing of hyperbaric chambers | The core Canadian standard for running the chamber itself safely |
| ASME PVHO-1 | ASME | Design, fabrication, and testing of pressure vessels for human occupancy and their piping | Confirms the chamber and its gas piping are built to a recognised safety standard |
| Health Canada medical device licence | Health Canada | Federal licensing of moderate-to-high risk medical devices | A medical hyperbaric chamber must be a licensed device, with post-market safety reporting |
Why is carbon monoxide the most dangerous air contaminant?
Carbon monoxide is the contaminant clinic operators worry about most, and for good reason. It is colourless, odourless, and binds to haemoglobin far more strongly than oxygen does, so even small amounts in the breathing supply can reduce the blood’s ability to carry oxygen. Carbon monoxide poisoning remains a major cause of illness and death worldwide. In a 2026 retrospective cohort of 272 patients (Yuceer, PubMed | Our Assessment), 103 of the 272 patients received hyperbaric oxygen therapy, and those with more severe neurological or cardiac involvement (lower Glasgow Coma Scale scores and ischaemic ECG findings) were the ones more likely to be selected for it. In other words, the very poisoning that hyperbaric medicine is used to treat is the contaminant a clinic must keep out of its own air supply.
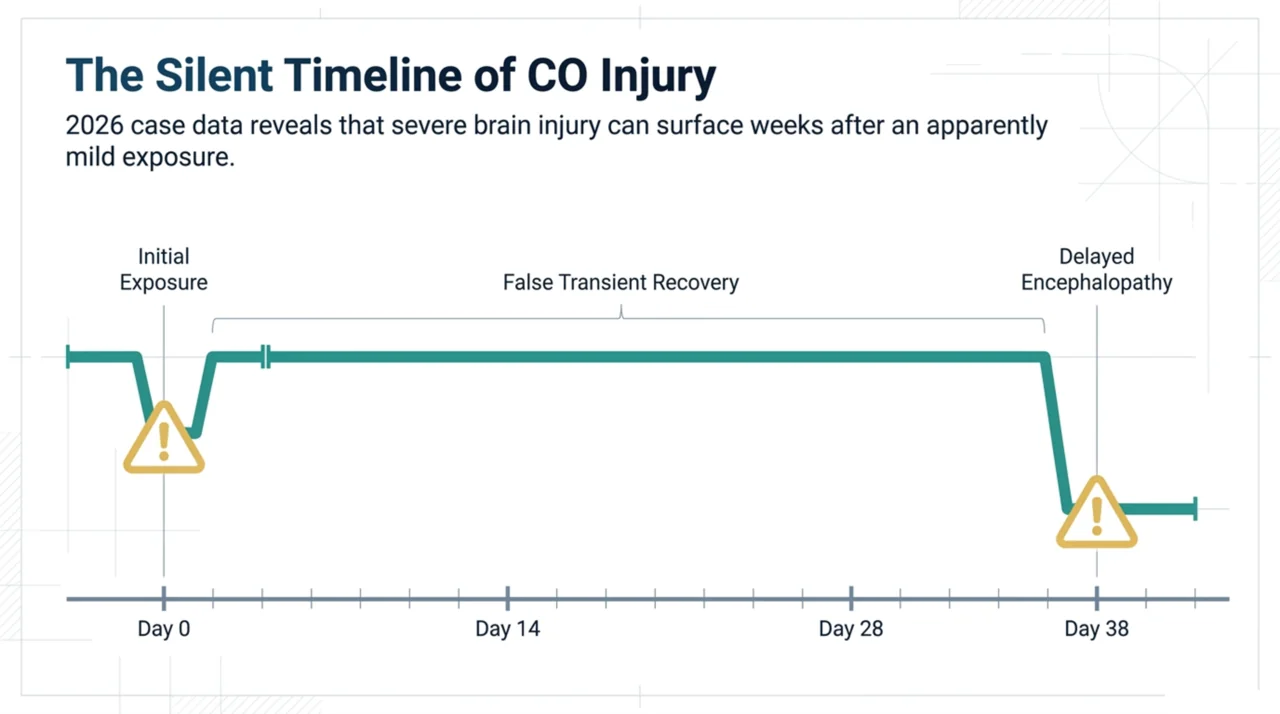
The danger does not always appear right away. A 2026 case report (Malopolska and colleagues, PubMed | Our Assessment) described a 29-year-old woman who improved after treatment for acute carbon monoxide poisoning, including hyperbaric oxygen therapy, then developed delayed encephalopathy 38 days later. The authors note that this kind of delayed brain injury can follow even an apparently mild exposure or a transient recovery. That is exactly why undetected carbon monoxide in a clinic’s breathing air supply is so serious: the harm can be silent at first and surface weeks afterward.
The practical takeaway is that carbon monoxide monitoring is non-negotiable. The most common source is a contaminated compressor intake, for example air drawn in near a loading dock, a parking area, or an exhaust vent. Engine exhaust, nearby combustion, and overheated compressor oil can all introduce carbon monoxide. The fix is partly placement (intakes away from any combustion source) and partly continuous detection.
How do you test and monitor compressed breathing air?
Air-quality assurance is a layered process, not a single test. The standards set specific numeric limits for each contaminant; the exact values are defined in CSA Z180.1 and should be read directly from the current edition. A practical monitoring program for a Canadian clinic generally includes the following steps.
- Position the compressor intake correctly. Keep it well away from vehicle traffic, exhaust vents, generators, and any combustion source. This is the single most effective way to prevent carbon monoxide and hydrocarbon contamination.
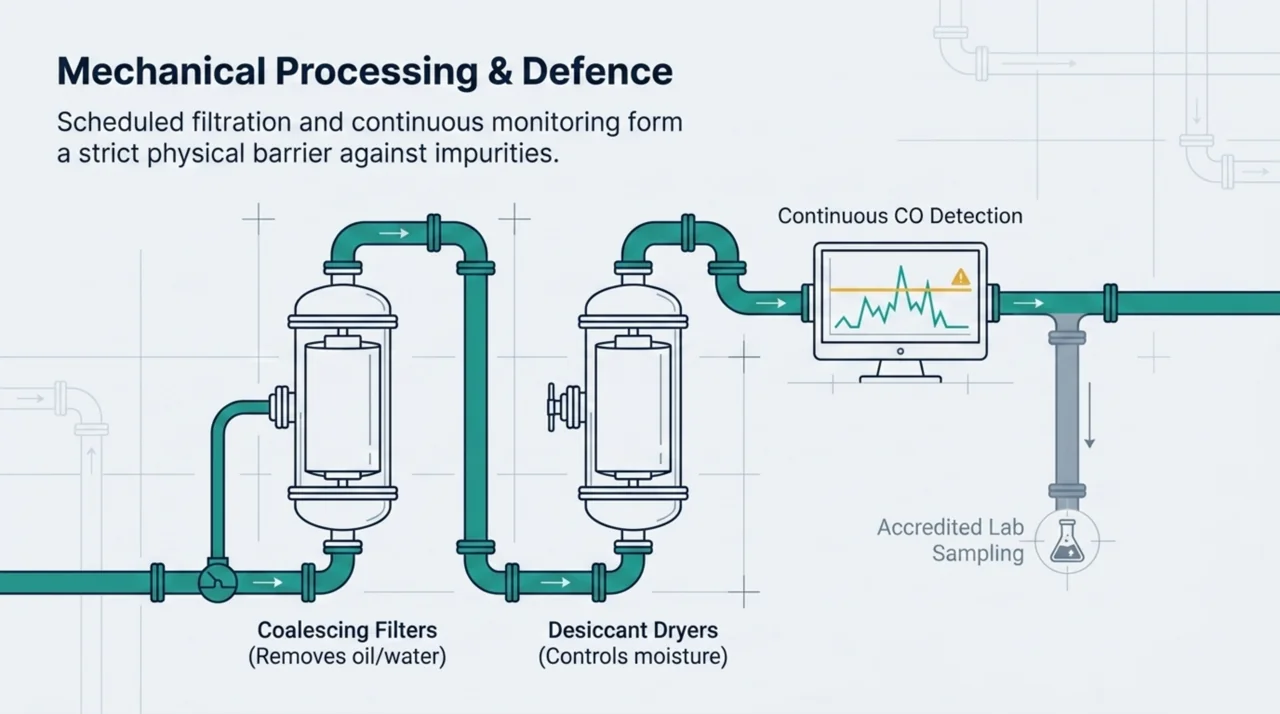
- Install continuous carbon monoxide monitoring on the air supply, with an alarm that interrupts or alerts before contaminated air can reach a patient.
- Maintain the filtration and drying train. Coalescing filters remove oil and water, and desiccant dryers control moisture. Change cartridges on the schedule the manufacturer and standard specify, not just when they look spent.
- Schedule periodic laboratory air sampling. Send samples to an accredited lab to confirm carbon monoxide, carbon dioxide, oil, water vapour, and odour all meet the CSA Z180.1 limits.
- Log every result and every maintenance action. A documented trail is both a safety tool and an accreditation and Health Canada compliance requirement.
- Train staff to respond to an out-of-range result. Everyone on shift should know how to take the air system offline and switch to a verified backup supply.
Treat the air system the way you treat the chamber: as a piece of life-support equipment with a maintenance schedule, a logbook, and a defined failure response. Many clinics fold this into a broader preventive-maintenance plan that also covers valves, gauges, and the chamber pressure boundary.
How does pressure change gas delivery inside the chamber?
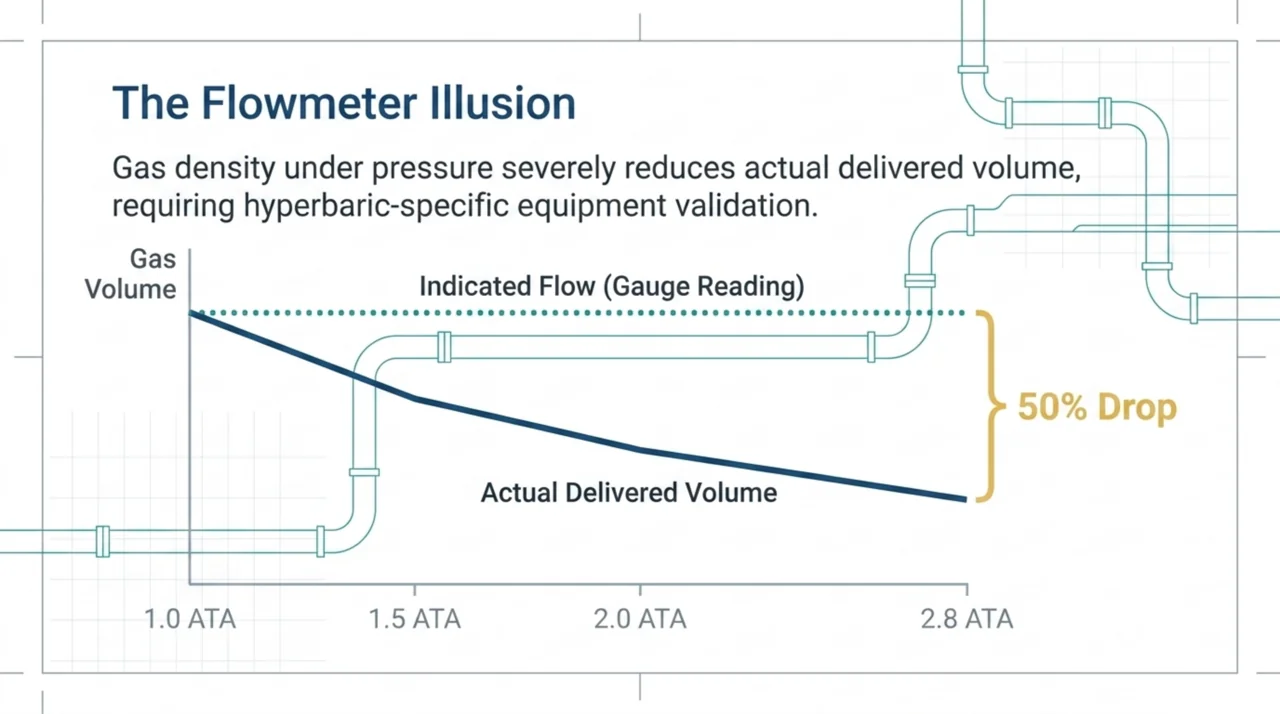
Clean air at the inlet is necessary but not sufficient. Pressure also changes how gases behave once the chamber door closes, and that can catch an operator off guard. A 2026 technical report (Aufgang and colleagues, PubMed | Our Assessment) measured oxygen flowmeters under hyperbaric conditions and found a striking gap between what the gauge showed and what was actually delivered. While the indicated reading on the flowmeter barely moved, the actual volume of oxygen delivered fell by about 50 percent as chamber pressure rose from 1 to 2.8 atmospheres absolute. A low-flow meter showed reductions of roughly 40 to 43 percent across the same pressure range.
For a clinic owner, the lesson is that equipment must be validated under the conditions it actually operates in, not just on the bench at surface pressure. A flowmeter, regulator, or oxygen-delivery device that reads correctly in the office may behave very differently at treatment depth. Built-in breathing systems, masks, and any add-on oxygen equipment should be checked against the manufacturer’s hyperbaric specifications, and staff should understand that a gauge reading is an indication, not a guarantee of delivered flow.
What gas-safety risks should clinic owners plan for?
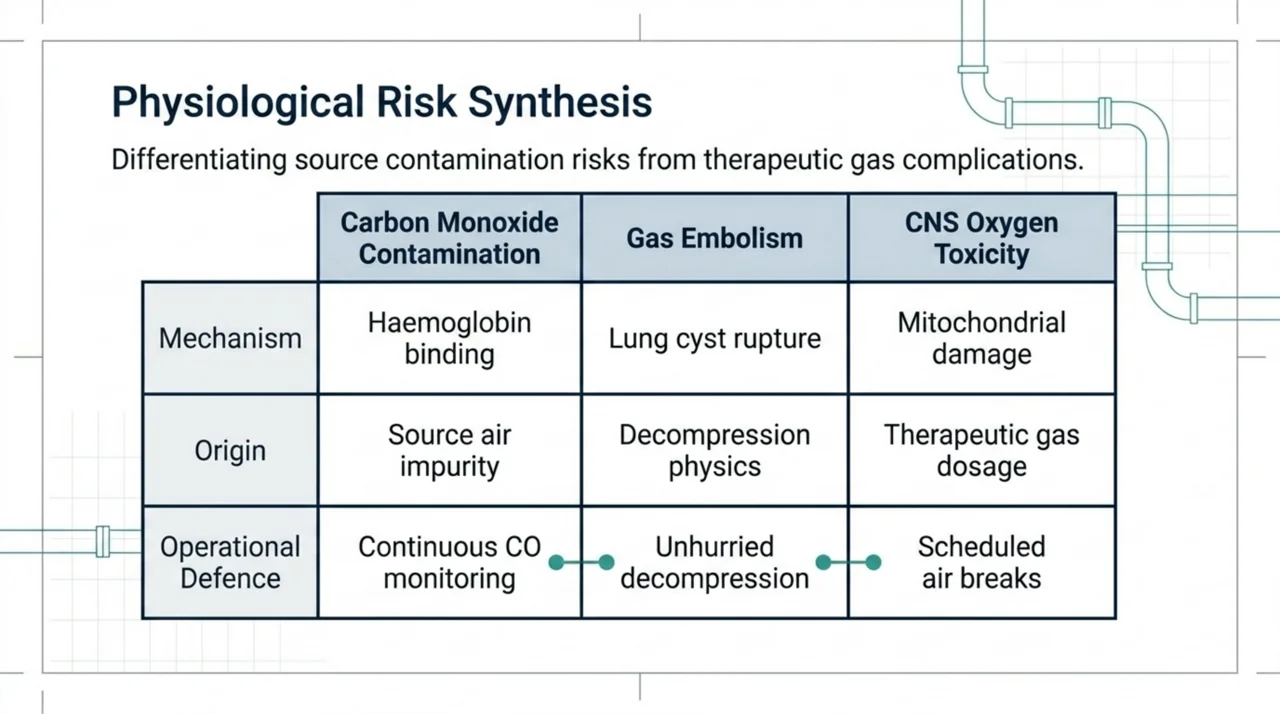
Beyond contamination, two gas-related risks deserve a place in every clinic’s safety plan: gas embolism and oxygen toxicity. Both are uncommon, but both are serious, and a written protocol is the best defence.
Gas embolism inside the chamber is rare but real. A 2026 case report (Ramchandani and colleagues, PubMed | Our Assessment) described a 73-year-old man who developed sudden neurological deficits during decompression on his first hyperbaric session for a chronic leg wound. Imaging later revealed lung cysts and a probable transient connection that allowed gas to enter an artery during decompression. The authors stressed the importance of vigilance during decompression and careful patient assessment. For operators, this reinforces the value of controlled, unhurried decompression and of screening for lung conditions that raise the risk.
Oxygen itself, the therapeutic gas, must also be controlled. Central nervous system oxygen toxicity, which can cause seizures, is a recognised complication of breathing oxygen at high pressure. In a 2026 laboratory study using rats and cultured neurons (Ding and colleagues, PubMed | Our Assessment), exposure to oxygen at a very high pressure of 6 atmospheres absolute caused mitochondrial damage associated with this toxicity. Clinical treatment pressures are far lower than that experimental level, but the finding reinforces why oxygen exposure times, scheduled air breaks, and partial-pressure limits are written into hyperbaric safety protocols in the first place.
How should a clinic build an air-quality and gas-safety program?
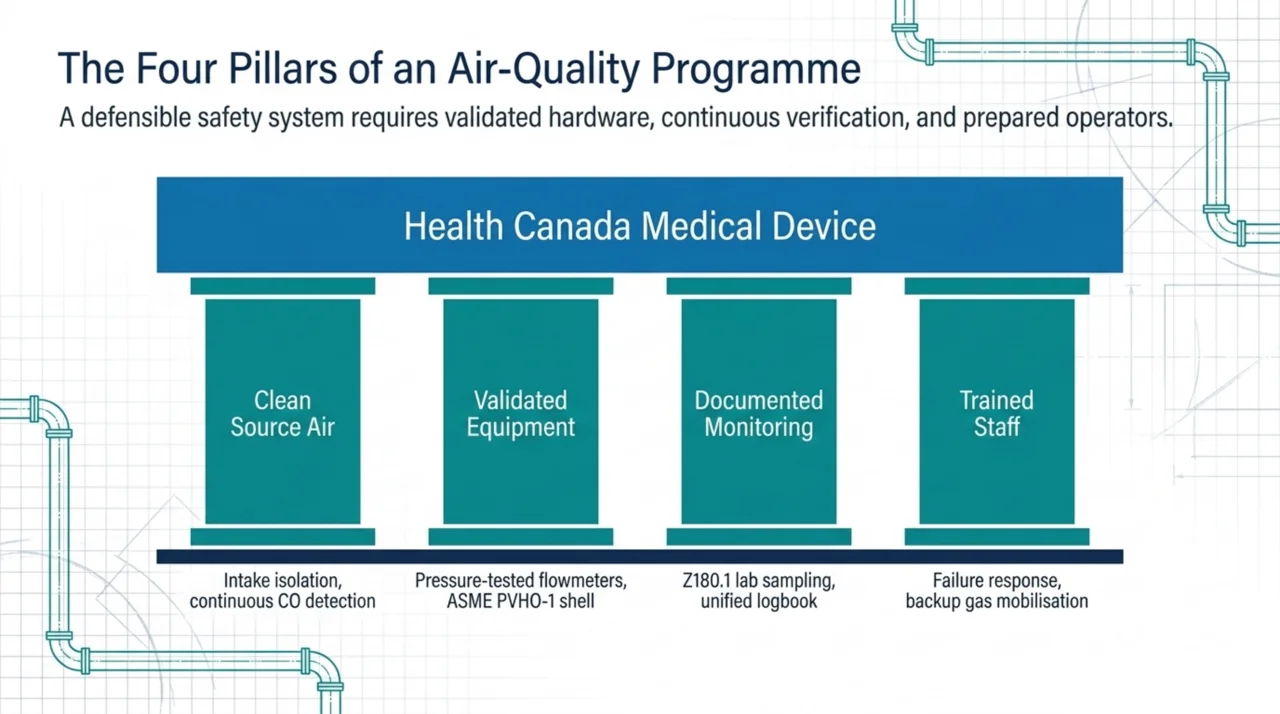
Pulling it together, a defensible program rests on four pillars: clean source air, validated equipment, documented monitoring, and trained staff. The steps below give clinic owners a starting framework that maps onto the Canadian standards and Health Canada expectations.
- Write air quality into your standard operating procedures. Reference CSA Z180.1 for purity limits and CSA Z275.1 for chamber operation, and name who is responsible for each check.
- Verify the chamber and piping pedigree. Confirm the vessel meets ASME PVHO-1 and that the device carries the appropriate Health Canada licence.
- Build a contaminant-monitoring schedule. Continuous carbon monoxide detection, scheduled filter and desiccant changes, and periodic accredited-lab air sampling.
- Validate gas-delivery equipment under pressure, not just at the surface, and record the results.
- Maintain a single, auditable logbook for air tests, maintenance, and any out-of-range events, ready for an accreditation survey or Health Canada review.
- Drill the failure response. Every team member should know how to isolate the air system and switch to a verified backup if a monitor alarms.
None of this is about chasing a perfect score on a form. It is about making sure that the gas a patient breathes under pressure is exactly what you intend it to be. Patients and referrers can compare accredited hospitals and regulated facilities through the Canada Hyperbarics directory of hospitals and regulated facilities, and a strong air-quality program is part of what sets a credible clinic apart.
Frequently asked questions about hyperbaric chamber air quality
What contaminants are tested for in hyperbaric breathing air?
The main contaminants are carbon monoxide, carbon dioxide, condensed oil and hydrocarbons, water vapour, and odour. Each has a defined limit in CSA Z180.1, the Canadian standard for compressed breathing air. Carbon monoxide receives the most attention because it is colourless, odourless, and dangerous even in small amounts under pressure.
How often should a clinic test its compressed breathing air?
Carbon monoxide should be monitored continuously while the system is in use. Laboratory air sampling for the full panel of contaminants is done on a periodic schedule, and filters and dryers are serviced on the interval set by the manufacturer and the applicable standard. The exact frequency should be written into your standard operating procedures and confirmed against the current edition of CSA Z180.1.
Does a hyperbaric chamber need a Health Canada licence?
A medical hyperbaric chamber is a medical device in Canada. Moderate-to-high risk devices require a medical device licence from Health Canada, which involves safety information and ongoing post-market reporting. You can read the current requirements on the Health Canada medical device licensing page linked above.
Why does oxygen flow read differently under pressure?
Flowmeters are calibrated at surface pressure, and the increased density of gas inside a pressurised chamber changes the actual volume delivered. A 2026 technical report found the real delivered flow dropped by about half at 2.8 atmospheres absolute even though the gauge reading barely changed. This is why oxygen-delivery equipment must be validated under hyperbaric conditions.
What is the difference between air quality and oxygen toxicity?
Air quality is about keeping contaminants such as carbon monoxide out of the breathing supply. Oxygen toxicity is a separate risk that comes from the therapeutic oxygen itself when exposure time and pressure are not controlled. Both are managed through protocols, but they are different problems with different controls.
Where can I find the official Canadian standards?
CSA Z180.1 and CSA Z275.1 are published by CSA Group, ASME PVHO-1 is published by ASME, and medical device rules are administered by Health Canada. Each is linked in this article. Always work from the current edition, as contaminant limits and requirements are updated over time.
Key takeaways for Canadian clinic owners
Breathing air quality is a safety system, not paperwork. Carbon monoxide is the contaminant of greatest concern, and its harm can be delayed, so continuous monitoring is essential. Pressure changes how gases behave inside the chamber, which means equipment must be validated under hyperbaric conditions. The Canadian and international standards (CSA Z180.1, CSA Z275.1, ASME PVHO-1) and Health Canada licensing give you a clear framework, and accreditation programs add a recognised external check. Build the four pillars (clean source air, validated equipment, documented monitoring, trained staff) and you have a program that protects patients and stands up to scrutiny. To see how accredited hospitals and regulated facilities present their standards, explore the Canada Hyperbarics facilities directory or review the broader research library behind hyperbaric safety.
This content is for informational purposes only and does not constitute medical advice. It is intended to support clinic owners and operators in understanding safety standards, not to replace the current published editions of the standards cited, professional engineering advice, or Health Canada guidance. Always work from the official, current editions of any standard and consult qualified professionals when designing or operating a hyperbaric facility.