
TL;DR: A hyperbaric wound-care program is built around three equipment pillars: a Health Canada-licensed pressure chamber, an oxygen delivery system, and patient-assessment and monitoring tools. Choose the chamber type to match your wound caseload, build to recognised construction and safety standards, and plan for accreditation before you treat your first patient. This guide walks Canadian clinic owners through each decision step by step.
Hyperbaric oxygen therapy (HBOT) is a medical treatment in which a patient breathes 100% oxygen inside a pressurised chamber, raising the amount of oxygen dissolved in the blood and delivered to oxygen-starved tissue. For wound care, that extra oxygen is the whole point. A 2026 review of problem wounds (Huang et al., PubMed | Our Assessment) traced the field back to foundational work showing that wound healing depends on tissue oxygenation. Your equipment exists to deliver that oxygen safely and repeatably.
Adding a wound-care service line is one of the most common reasons a Canadian clinic invests in hyperbaric equipment. Chronic and non-healing wounds are a large and growing burden, and the evidence base for hyperbaric oxygen therapy as an adjunct continues to mature. But the equipment decision is where many new operators get stuck. This guide from Canada Hyperbarics explains what equipment a wound-care program needs, which standards apply in Canada, and how to plan the purchase in a sensible order.
Why does the clinical evidence matter before you buy wound-care equipment?
Equipment is a major capital commitment, so the business case should rest on the evidence for the wounds you plan to treat. The clinical literature is encouraging but nuanced, and matching your equipment to realistic indications protects both your patients and your investment.
Diabetic and other chronic wounds are difficult precisely because the underlying biology works against healing. A 2026 review of diabetic wound healing (Jreije et al., PubMed | Our Assessment) described how sustained high blood sugar drives persistent inflammation, impaired blood-vessel growth, and refractory ulcers, and concluded that no single treatment fully addresses the problem. That is a useful reality check: HBOT is positioned as one part of a multimodal wound program, not a standalone cure.
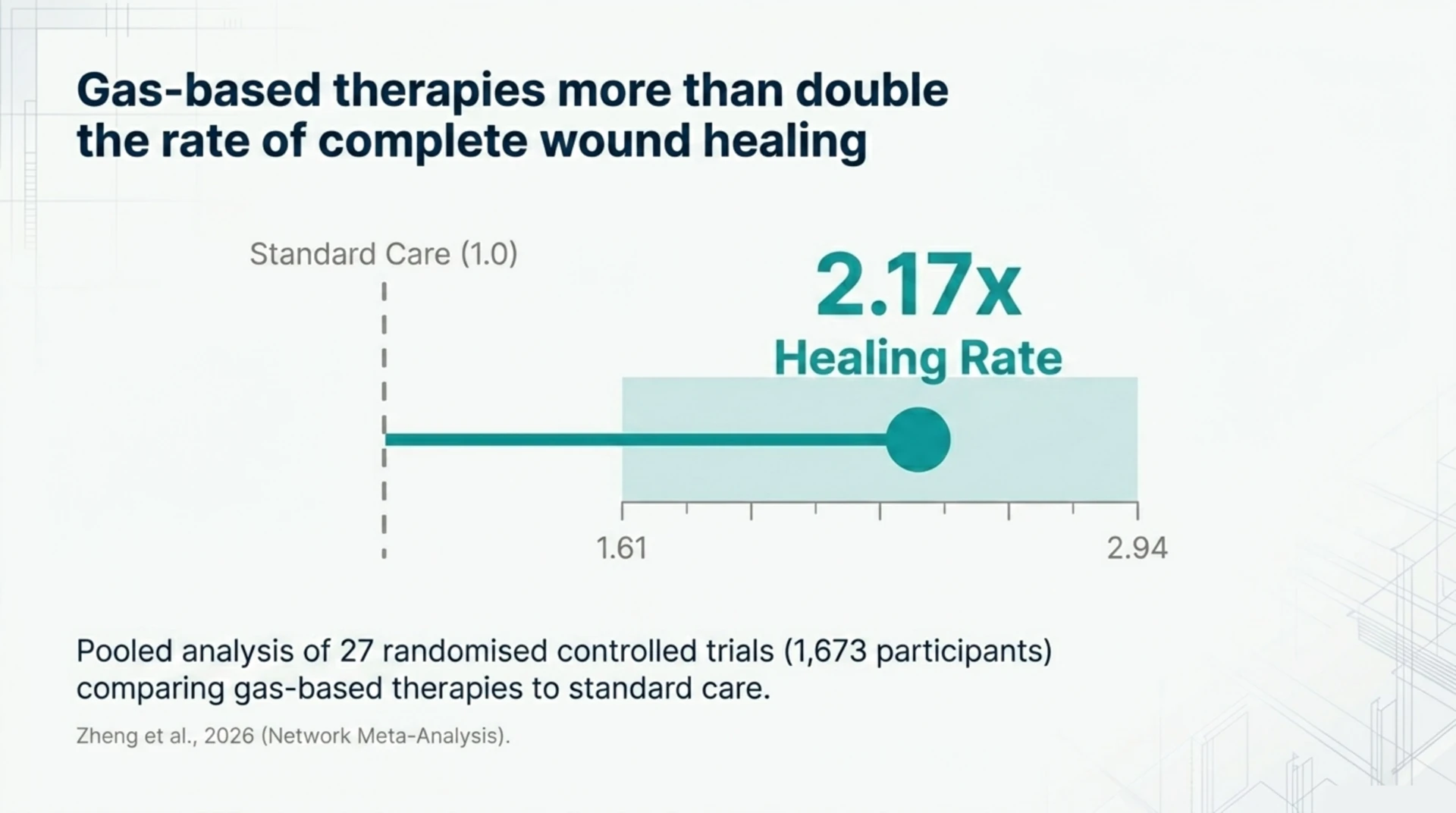
On effectiveness, a 2026 systematic review and network meta-analysis of 27 randomised controlled trials (1,673 participants) (Zheng et al., PubMed | Our Assessment) found that gas-based therapies, a group that includes HBOT, were associated with more than double the rate of complete wound healing compared with standard care in pooled analysis (risk ratio 2.17, 95% confidence interval 1.61 to 2.94). The authors cautioned that the studies varied widely and that the network ranking was less clear-cut, so the result is best read as supportive rather than definitive.
For surgical and reconstructive wounds, a 2026 structured review of surgical wound healing and tissue salvage (González Flores et al., PubMed | Our Assessment) reported that HBOT works through enhanced plasma-dissolved oxygen delivery, angiogenesis, fibroblast proliferation, and collagen synthesis, and that the evidence supports its use in chronic ischaemic wounds such as diabetic foot ulcers, venous leg ulcers, burns, and radiation-injured tissue. A 2026 systematic review and meta-analysis of skin flap and graft indications (Carter et al., PubMed | Our Assessment), covering 24 studies and 2,246 patients (including 13 randomised controlled trials), issued a strong GRADE recommendation to use HBOT to help heal flaps and grafts in soft-tissue and trauma wounds.
The takeaway for an owner: the strongest, most established wound indications are also the ones publicly funded in Canada, and those should anchor your equipment specification and your referral relationships. You can review the recognised indications and the Canadian regulatory picture on our HBOT regulatory framework page.
What hyperbaric equipment does a wound-care program actually need?
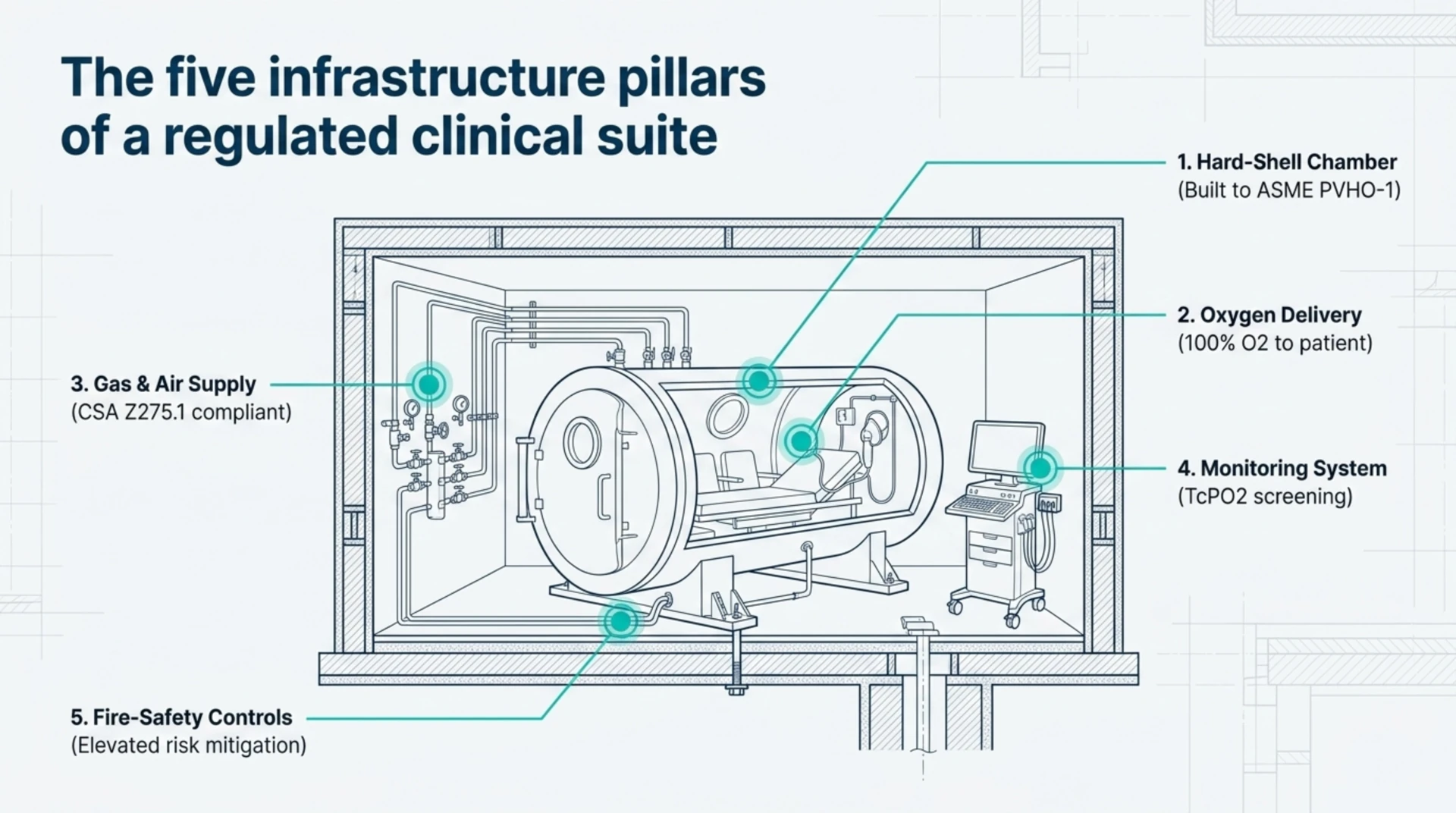
A clinical wound-care program is more than a chamber. The table below summarises the core equipment components, what each one does, and the main Canadian standard or consideration attached to it.
| Equipment component | What it does | Key standard or consideration |
|---|---|---|
| Hard-shell hyperbaric chamber | Delivers pressurised oxygen treatment | Must be a Health Canada-licensed medical device; built to ASME PVHO-1 |
| Oxygen delivery system | Supplies 100% oxygen to the patient (hood, mask, or chamber fill) | Sized to chamber type; monoplace fills the chamber, multiplace uses hoods or masks |
| Compressed gas and air supply | Pressurises the chamber and supports patient breathing | Clean, dry medical-grade supply; refer to CSA Z275.1 facility requirements |
| Patient assessment and monitoring | Screens and tracks patients (vitals, tissue oxygen) | Transcutaneous oximetry (TcPO2) supports physician patient selection |
| Fire-safety and grounding systems | Controls the elevated fire risk of an oxygen-rich environment | Integral to CSA Z275.1 hyperbaric facility design |
How do you choose hyperbaric wound-care equipment step by step?
Work through these steps in order. Each one narrows the next decision, which keeps you from over-buying or specifying a chamber that does not suit your patients.
- Define your patient population first. Decide which wounds you intend to treat (for example diabetic foot ulcers, compromised grafts and flaps, or radiation tissue injury). The indication mix drives session length, patient throughput, and whether you need single-patient or multi-patient capacity.
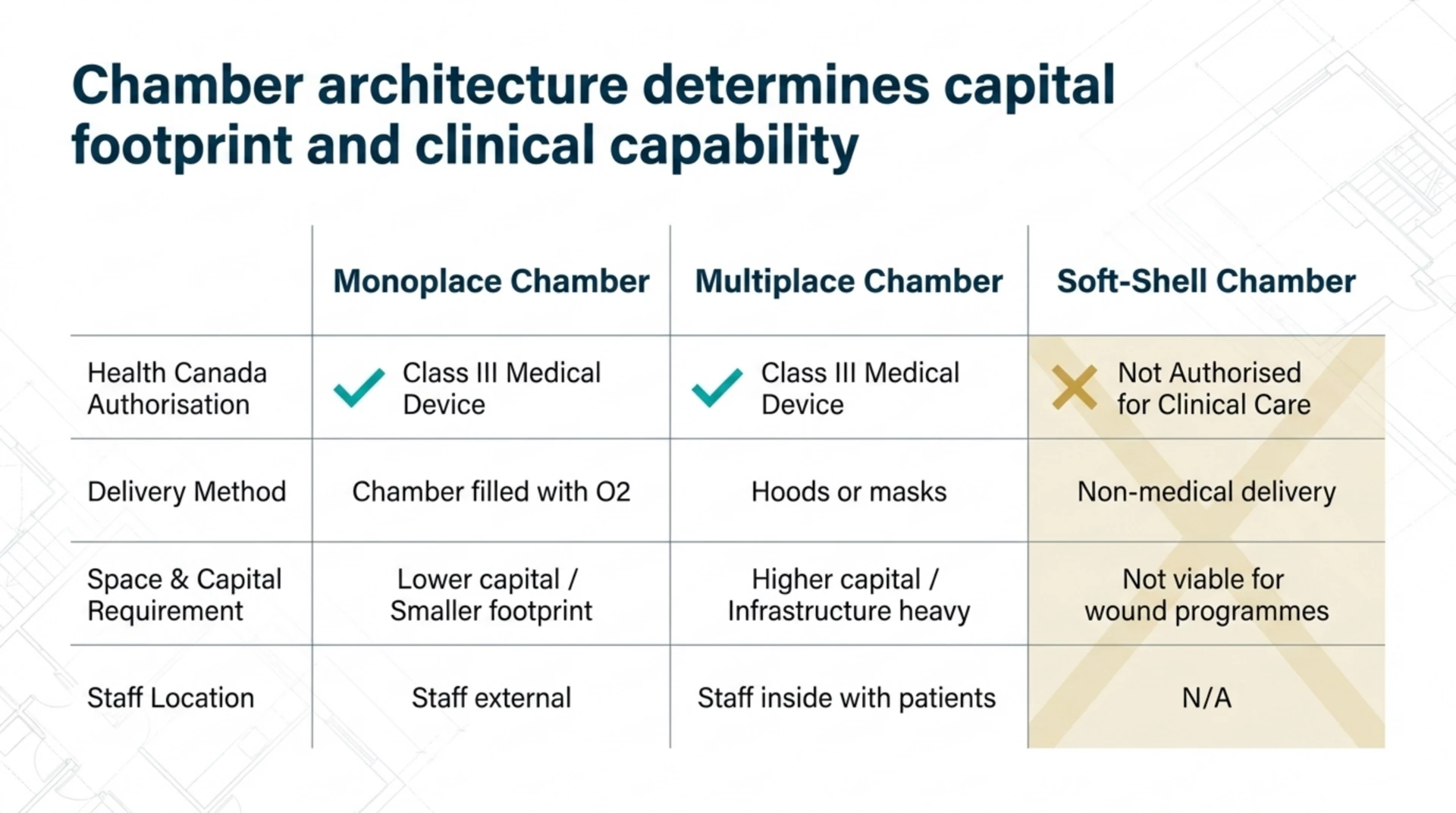
- Select a Health Canada-licensed chamber. In Canada, hyperbaric chambers are regulated as Class III medical devices, and only hard-shelled chambers from licensed manufacturers are authorised for medical treatment. Confirm the licence before you sign anything. Soft-shelled chambers are not licensed for clinical care.
- Decide between a monoplace and a multiplace chamber. A monoplace chamber treats one patient at a time and is filled with oxygen; it has a smaller footprint and lower capital cost. A multiplace chamber treats several patients at once with masks or hoods and allows a staff member inside, but it costs more and needs more space and infrastructure. Match the choice to your projected daily volume.
- Specify the oxygen and gas supply. Size your medical oxygen and compressed-air supply to the chamber type and your treatment schedule. Plan storage, redundancy, and delivery logistics early, because gas supply is an ongoing operating cost, not a one-time purchase.
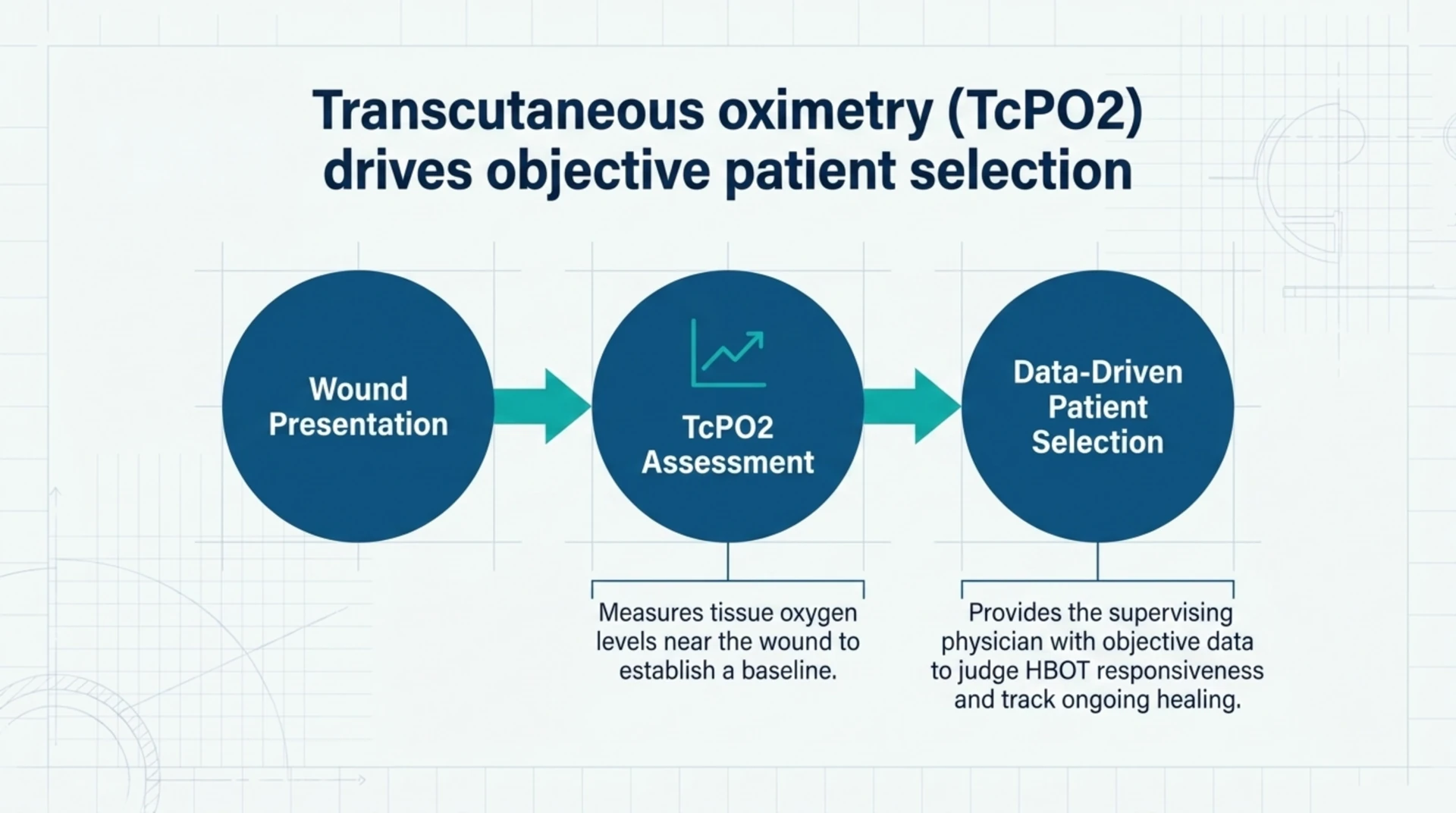
- Add patient-assessment and monitoring equipment. Many wound-care programs use transcutaneous oximetry (TcPO2) to measure the oxygen level in the tissue around a wound, which helps the supervising physician judge whether a patient is likely to benefit from HBOT and track healing over time. Plan for vital-sign monitoring suited to the chamber environment as well.
- Build to construction and safety standards. Confirm the chamber is built to ASME PVHO-1 and that your facility is designed and operated to CSA Z275.1, which sets minimum requirements for the operation, design, construction, maintenance, and testing of hyperbaric facilities in Canada.
- Plan for accreditation and documentation. Decide early whether you will pursue UHMS hyperbaric facility accreditation, because its requirements touch facility design, equipment, staffing, and training. Building toward those requirements from day one is far cheaper than retrofitting later.
Which standards and regulations apply to hyperbaric chambers in Canada?
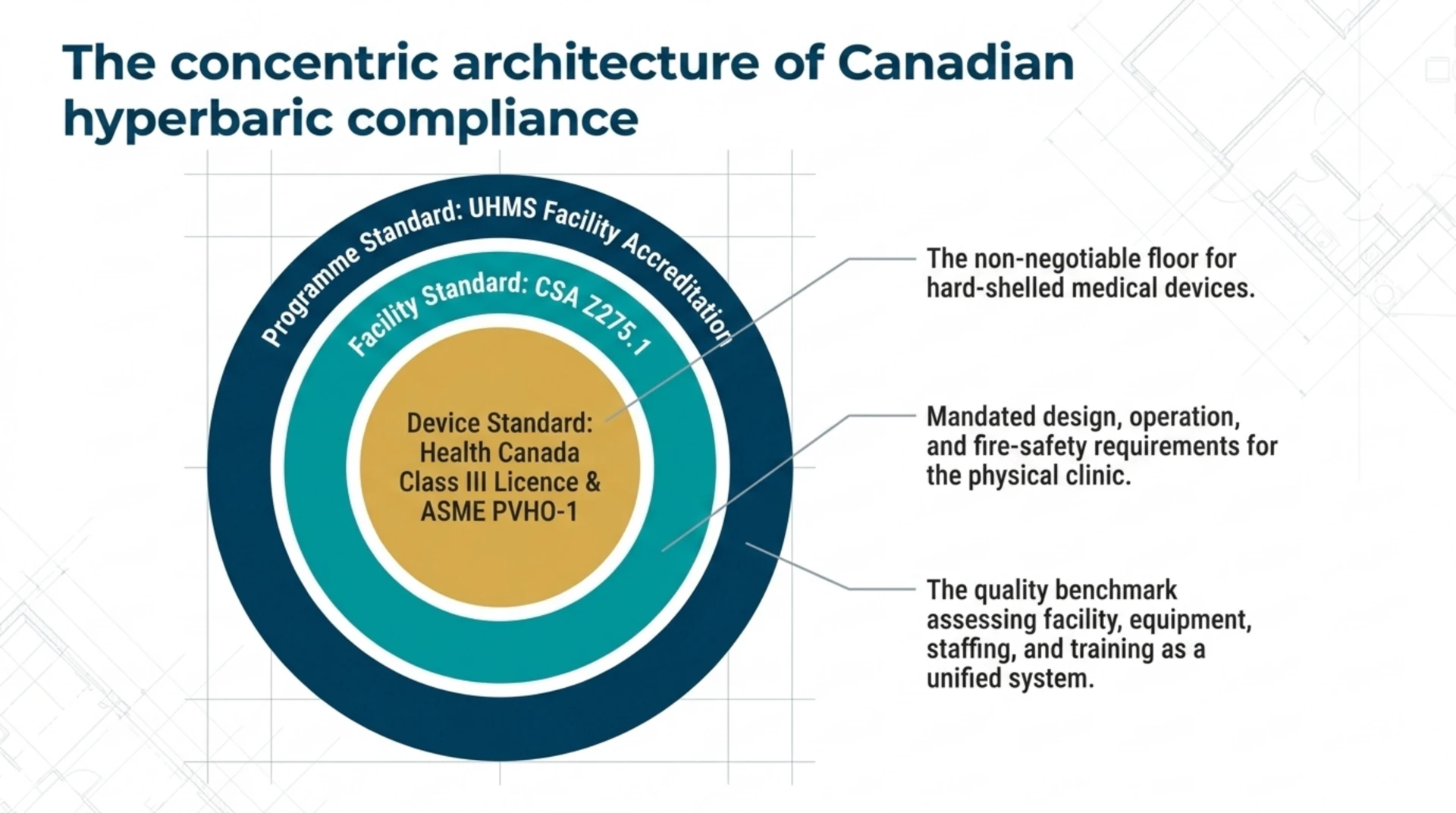
Three reference points matter most for equipment. The first is device licensing: Health Canada regulates hyperbaric chambers as Class III medical devices and has licensed only hard-shelled chambers from a small number of manufacturers. The second is construction: chambers are built to the ASME PVHO-1 Safety Standard for Pressure Vessels for Human Occupancy. The third is facility operation: CSA Z275.1 sets the Canadian requirements for hyperbaric facility design, operation, maintenance, and testing.
Treat these as the non-negotiable floor. A chamber that is not a licensed device, or a facility that does not meet CSA Z275.1, is not a viable clinical wound-care program regardless of how attractive the equipment price looks.
Should a wound-care clinic pursue UHMS accreditation?
For most clinical operators, the answer is yes, and the equipment plan should reflect it. UHMS hyperbaric facility accreditation evaluates the adequacy of your facility, equipment, staff, and training, and it is widely regarded as the benchmark for safe, credible hyperbaric care. Note the correct language: the UHMS recognises indications and accredits facilities; it does not approve or regulate. Designing your equipment and protocols to accreditation-level requirements from the outset signals quality to referring physicians and to patients comparing the hospitals and regulated facilities listed in the Canadian HBOT facility directory.
Frequently asked questions about hyperbaric wound-care equipment
What hyperbaric chamber is best for a wound-care clinic?
There is no single best chamber; the right choice depends on your patient volume and space. Monoplace chambers suit lower-volume clinics and have a smaller footprint and lower capital cost. Multiplace chambers suit higher volumes and allow a clinician inside with the patient, but they need more space, infrastructure, and capital. Both must be Health Canada-licensed, hard-shelled medical devices.
Do I need a Health Canada licence for a hyperbaric chamber?
Yes. Hyperbaric chambers are Class III medical devices in Canada, and clinical treatment must use a chamber from a licensed manufacturer. Health Canada has licensed hard-shelled chambers only; soft-shelled chambers are not authorised for clinical care and should not be used in a wound-care program.
How much does hyperbaric wound-care equipment cost?
Costs vary widely and depend on chamber type, oxygen and gas supply, monitoring equipment, facility construction to CSA Z275.1, and ongoing maintenance and staffing. A monoplace setup carries a lower capital cost than a multiplace installation, but the gas supply, servicing, and accreditation are recurring operating costs that must be budgeted alongside the purchase. Build a multi-year operating model rather than focusing on the chamber sticker price alone.
What monitoring equipment supports HBOT patient selection?
Transcutaneous oximetry (TcPO2) is commonly used to measure tissue oxygen levels near a wound. It gives the supervising physician objective information to help decide whether a patient is likely to respond to HBOT and to monitor progress. It is an assessment tool, not a treatment device, but it is a sensible part of a wound-care equipment plan.
Are soft-shell hyperbaric chambers suitable for clinical wound care?
No. Health Canada has not licensed soft-shelled hyperbaric chambers for medical use, and they should not form the basis of a clinical wound-care program. Clinical care relies on hard-shelled chambers from licensed manufacturers, built and operated to recognised pressure-vessel and facility standards.
What wounds is hyperbaric oxygen therapy used for?
The most established wound indications include diabetic foot ulcers, compromised skin grafts and flaps, and radiation-injured tissue, alongside other chronic non-healing wounds. You can read more about non-healing wounds on our non-healing wounds condition page. Specifying your equipment around these recognised indications keeps your program on solid clinical and regulatory ground.
Does the equipment plan change if I want UHMS accreditation?
Yes. UHMS accreditation assesses facility, equipment, staffing, and training together, so it is far easier to specify equipment and design your space to those requirements from the start than to retrofit a running clinic. If accreditation is on your roadmap, factor its requirements into every equipment decision above.
Putting your hyperbaric wound-care equipment plan together
Start from the patients you intend to serve, anchor your indications to the recognised evidence, and then specify a Health Canada-licensed chamber, an appropriately sized oxygen and gas supply, sound monitoring, and a facility built to CSA Z275.1 and ASME PVHO-1, with UHMS accreditation as your quality target. That order keeps the clinical case in front of the capital decision, which is exactly where it belongs. Canada Hyperbarics maintains a directory of hospitals and regulated facilities so owners and patients can see how established programs present themselves.
Ready to see how Canadian programs are set up? Explore the directory of hospitals and regulated facilities to benchmark your wound-care program.
This content is for informational purposes only and does not constitute medical advice. It is not regulatory, legal, or business advice. Clinic owners should confirm current Health Canada licensing requirements, applicable CSA and ASME standards, and accreditation criteria with the issuing bodies before making equipment or operational decisions.