
TL;DR: For Canadian clinic owners planning where to focus capacity, staff training, and referral development, the strongest 2026 hyperbaric oxygen therapy (HBOT) evidence sits with established indications: delayed radiation tissue injury, necrotizing soft-tissue infection, carbon monoxide poisoning, and chronic wound care. Emerging areas such as surgical flap salvage and athletic recovery show promise but rest on lower-certainty, non-randomised data. This Canada Hyperbarics briefing maps HBOT service lines by evidence strength so operators can invest where clinical demand and defensible science overlap.
Hyperbaric oxygen therapy (HBOT) is a medical treatment in which a patient breathes 100% oxygen inside a pressurised chamber, raising dissolved oxygen in the blood to support healing in oxygen-starved tissue. A hyperbaric service line is the defined clinical programme a clinic builds around a specific condition or referral pathway, including the staff competency, chamber time, and marketing behind it. In 2026, the smartest question a Canadian operator can ask is not “does HBOT work?” but “which HBOT service lines have the strongest current evidence, and where is that evidence still forming?” The answer shapes capital planning, accreditation priorities, and how you position your clinic to referring physicians.
This briefing reads the newest peer-reviewed research through an operator lens. It is not clinical guidance for treating patients; it is market and evidence intelligence for the people deciding which service lines to build. Every study cited below links to both the primary source on PubMed and our own plain-language assessment in the Canada Hyperbarics research database.
Why should evidence strength drive your service-line decisions?
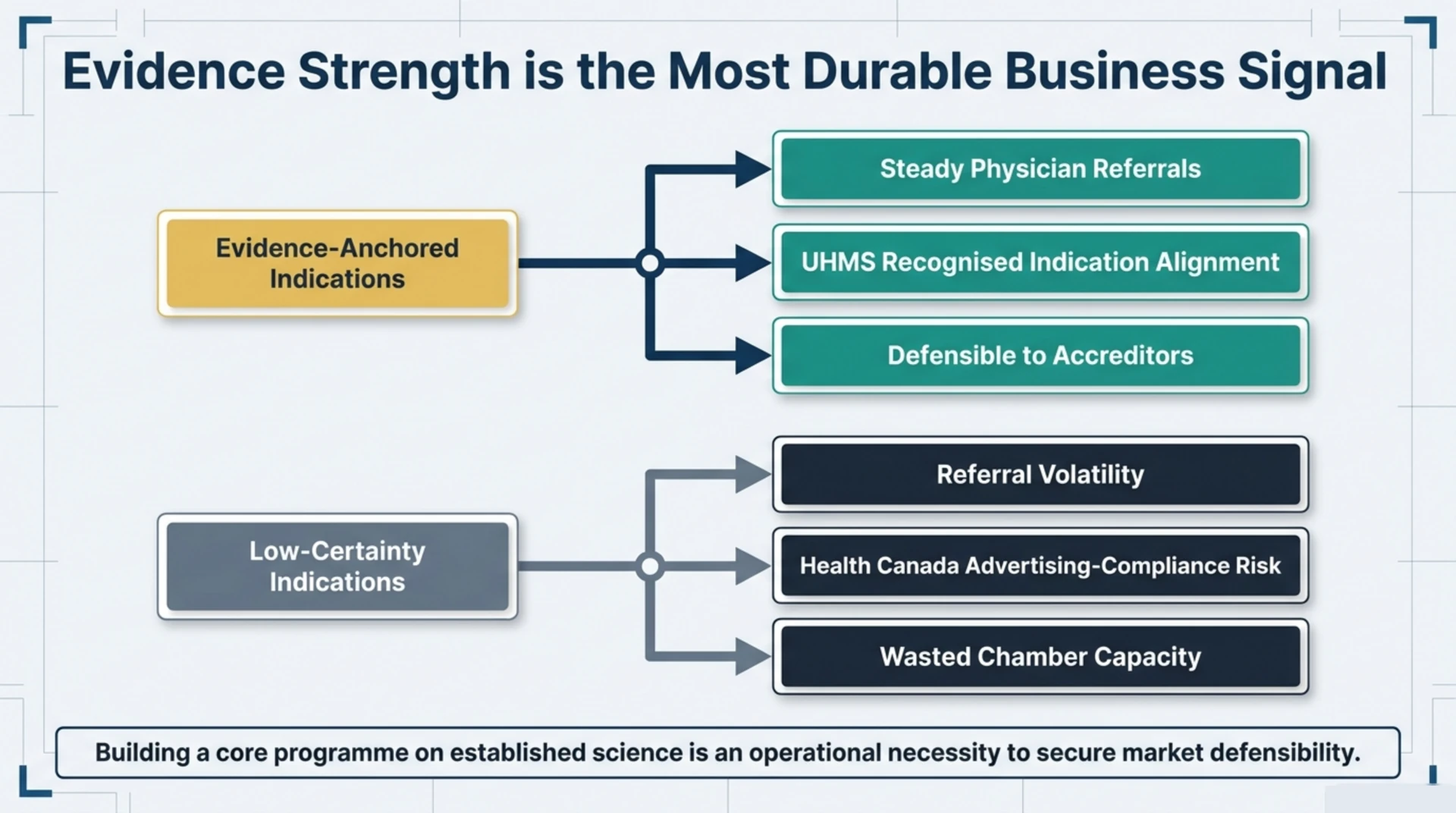
Evidence strength is the single most durable signal a clinic owner can plan around. Indications backed by systematic reviews and consistent outcomes attract steadier physician referrals, align with the conditions on the UHMS list of recognised indications, and are far easier to defend to accreditors and payers. Weakly evidenced indications, by contrast, expose a clinic to referral volatility, advertising-compliance risk under Health Canada rules, and wasted chamber capacity. Building your core programme on established science is a business decision as much as a clinical one.
Which HBOT service lines have the strongest evidence in 2026?
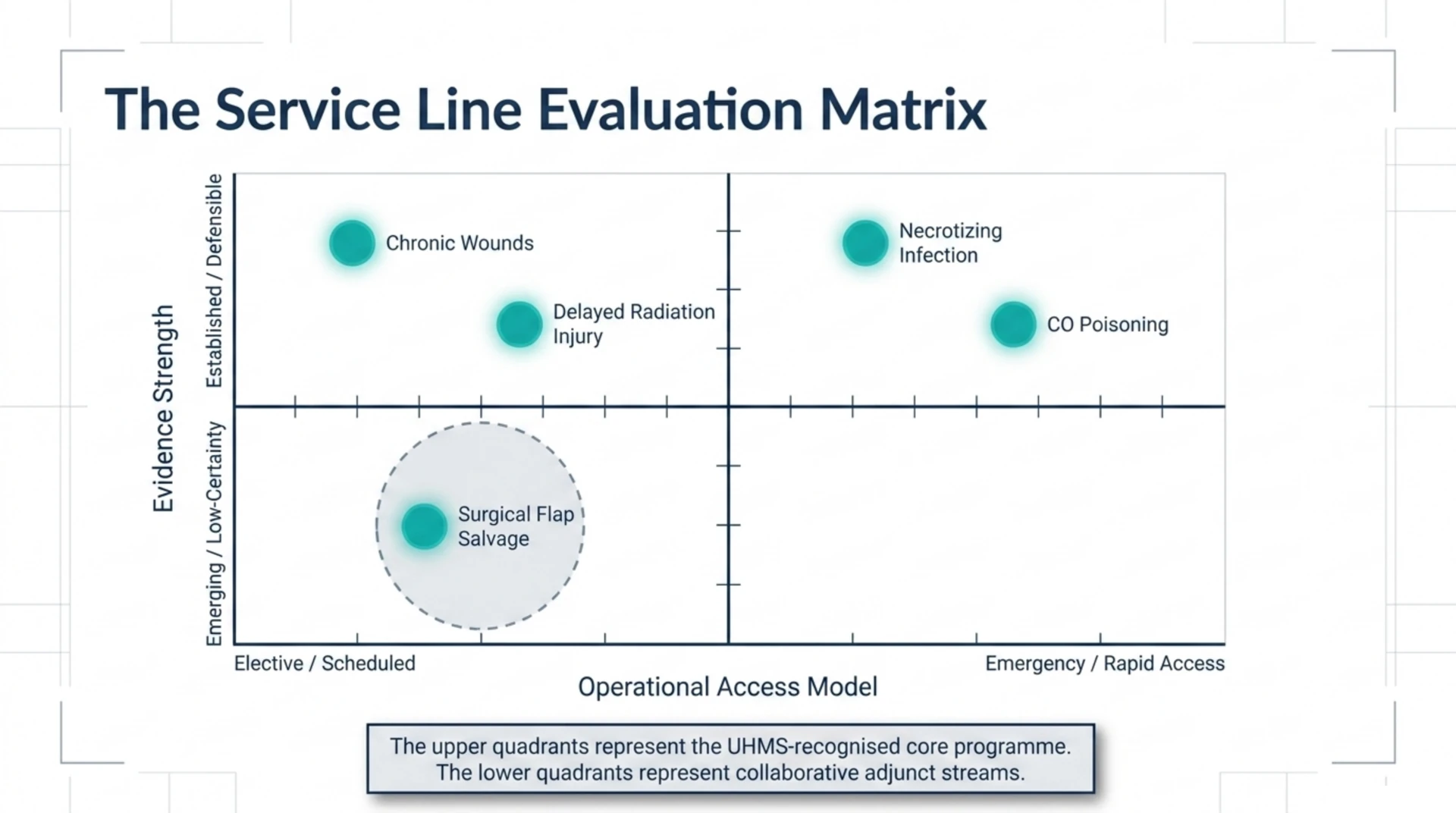
Four service lines stand out as evidence-anchored in 2026: radiation tissue injury, necrotizing soft-tissue infection, carbon monoxide poisoning, and chronic wound care. These map closely to the recognised indication list, which makes them the safest foundation for a Canadian clinic.
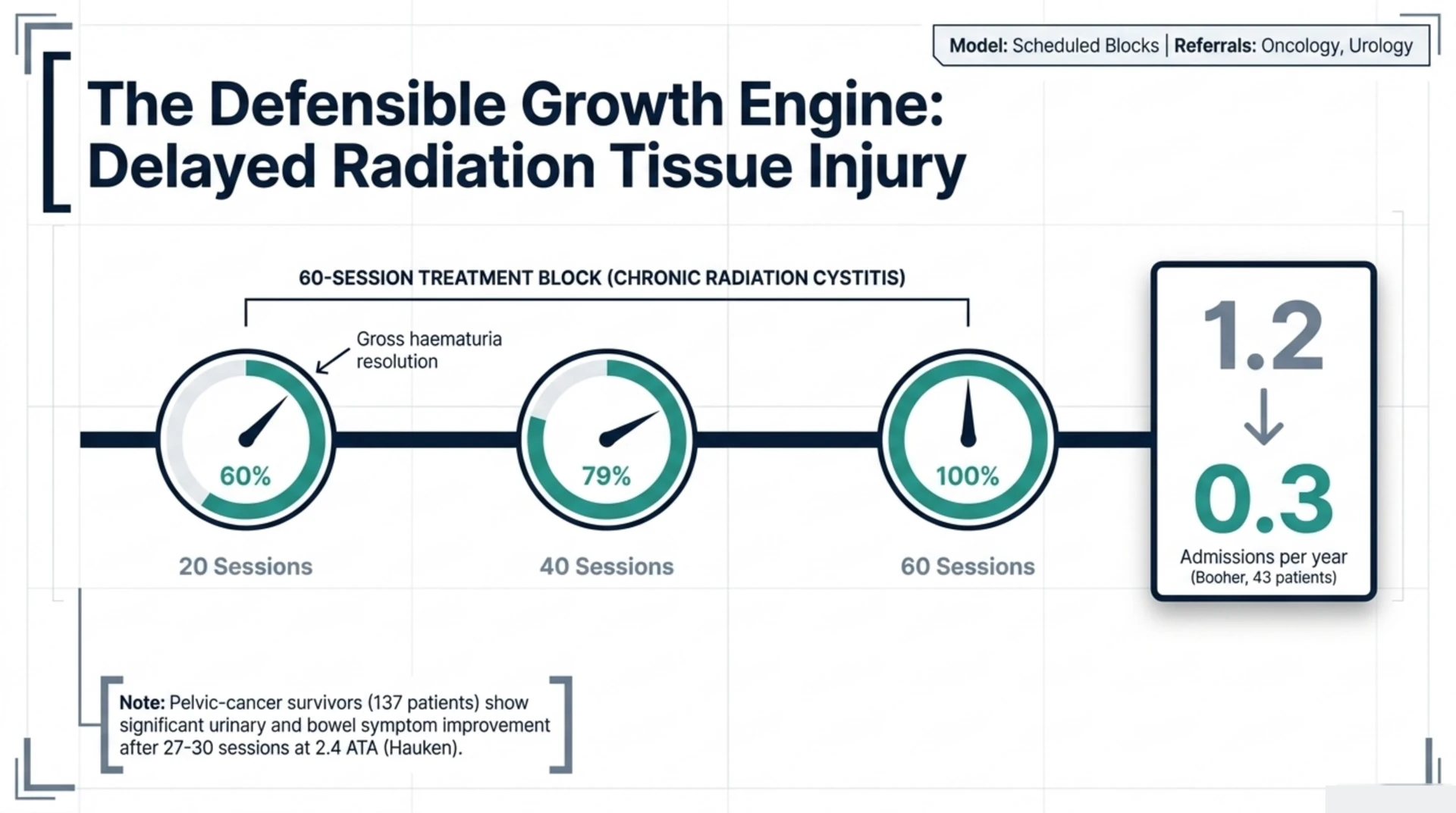
Delayed radiation injury is arguably the most defensible growth service line. One 2026 longitudinal study of 137 pelvic-cancer survivors (27 to 30 sessions at 2.4 atmospheres absolute) reported significant improvement in urinary and bowel symptoms after HBOT, though sexual-health scores did not change significantly (Hauken and colleagues, PubMed | Our Assessment). In chronic radiation cystitis, a 2026 review of prospectively collected data from 43 patients found HBOT was associated with resolution of gross haematuria in 60% of patients by 20 treatments, 79% by 40, and 100% by 60, with haematuria-related admissions falling from 1.2 per year before treatment to 0.3 after (Booher and colleagues, PubMed | Our Assessment). Both are observational, so the results describe association rather than proof, but radiation injury referrals tend to be steady and clinically appropriate.
Necrotizing soft-tissue infection carries a strong adjunctive-mortality signal. A 2026 meta-analysis of 14 studies (793 patients) found that adjunctive HBOT was associated with lower mortality in Fournier’s gangrene: 9.55% in the HBOT cohort versus 27.45% in the conventional-therapy cohort (relative risk 0.33; 95% confidence interval 0.23 to 0.48) (Huang and colleagues, PubMed | Our Assessment). Because it pools observational data, this is an association, not a randomised proof of causation. Necrotizing infection is an emergency indication, so this service line depends on strong hospital and surgical referral relationships rather than elective marketing.
Carbon monoxide poisoning remains a core emergency indication. A 2026 retrospective cohort of 272 carbon-monoxide-poisoning patients found that the 103 patients selected for HBOT presented more severely, with lower Glasgow Coma Scale scores, higher cardiac biomarkers, and more frequent ischaemic ECG findings, reflecting how clinicians triage the sickest patients to hyperbaric treatment (Yuceer, PubMed | Our Assessment). For operators, the operational lesson is capacity: emergency indications need rapid-access protocols, not appointment books.
Chronic and diabetic wound care is the volume backbone of most Canadian programmes. A 2026 review of diabetic wound healing positioned HBOT among the evidence-examined interventions for refractory ulcers while stressing that no single modality resolves the multifactorial biology of diabetic wounds, which argues for a multimodal wound-care programme rather than HBOT alone (Jreije and colleagues, PubMed | Our Assessment). Wound care pairs naturally with the equipment and staffing most clinics already run, which is why it anchors so many service lines.
How do the leading service lines compare at a glance?
| Service line | 2026 evidence strength | Typical referral source | Operator model |
|---|---|---|---|
| Delayed radiation injury | Established (observational, consistent) | Oncology, urology | Elective, scheduled blocks |
| Necrotizing infection | Adjunctive mortality signal (pooled observational) | Surgery, hospital | Emergency, rapid access |
| Carbon monoxide poisoning | Established emergency indication | Emergency departments | Emergency, on-call |
| Chronic and diabetic wounds | Established, best used multimodally | Wound clinics, endocrinology | High-volume, scheduled |
| Surgical flap salvage | Emerging, low certainty | Plastic and reconstructive surgery | Adjunct, case-by-case |
Where is demand growing but the evidence still emerging?
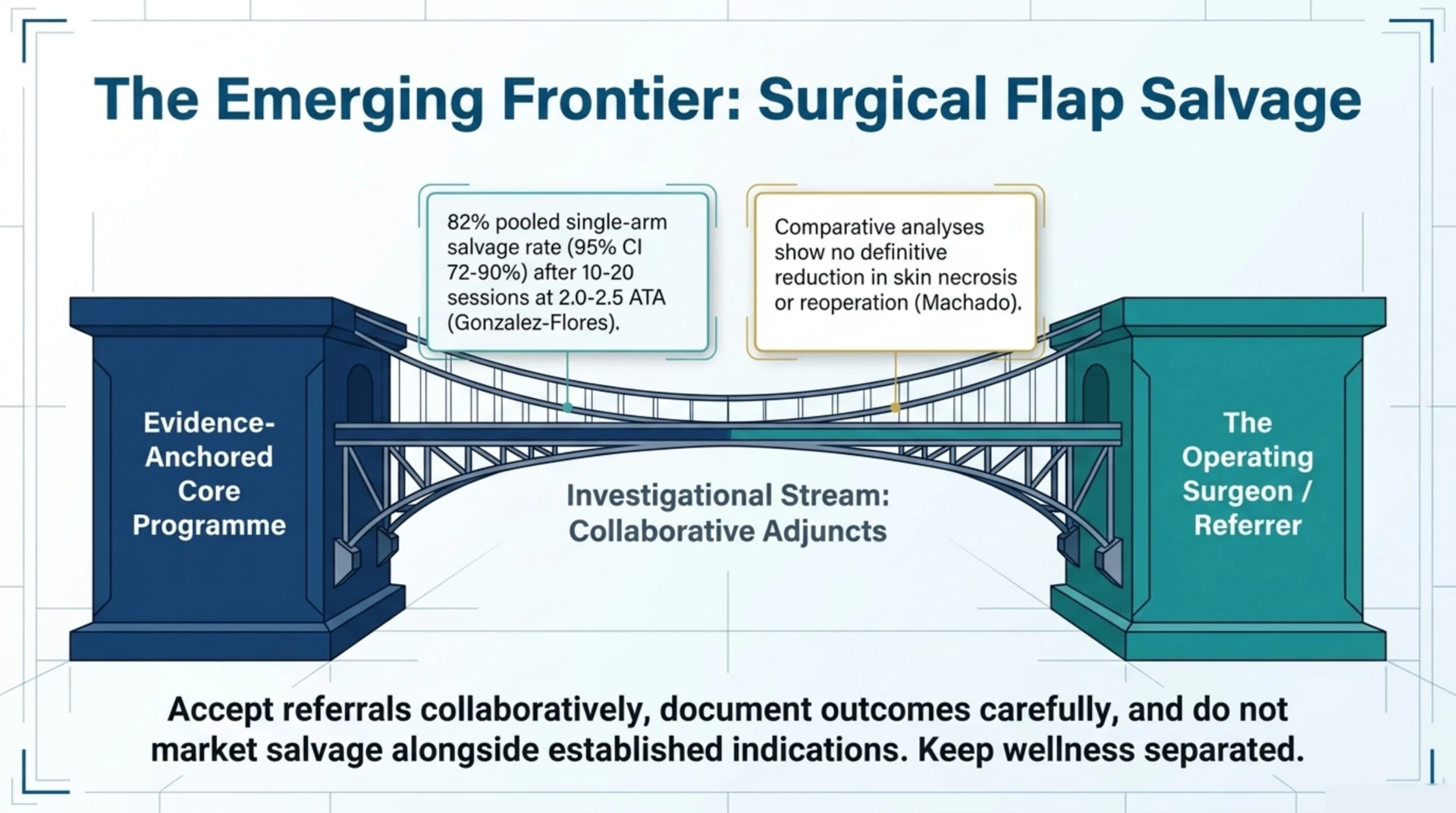
Two areas are generating referral interest ahead of definitive evidence, and operators should treat them as adjunct offerings rather than core service lines. Surgical flap and reconstruction salvage is the clearest example. A 2026 systematic review of five observational studies (409 patients, 75 receiving HBOT) reported pooled single-arm flap salvage of 82% (95% confidence interval 72% to 90%) after 10 to 20 sessions at 2.0 to 2.5 atmospheres absolute (Gonzalez-Flores and colleagues, PubMed | Our Assessment). Those salvage rates look encouraging, but a separate 2026 review found HBOT did not significantly reduce skin necrosis or reoperation in comparative analyses, underscoring that the controlled evidence is not yet settled (Machado and colleagues, PubMed | Our Assessment).
The practical takeaway is to accept flap-salvage referrals collaboratively with the operating surgeon, document outcomes carefully, and avoid marketing salvage as an established indication. Investigational and wellness uses, including athletic recovery, should stay clearly separated from your evidence-anchored medical service lines to protect advertising compliance and referrer trust.
How should Canadian clinic owners turn this evidence into a plan?
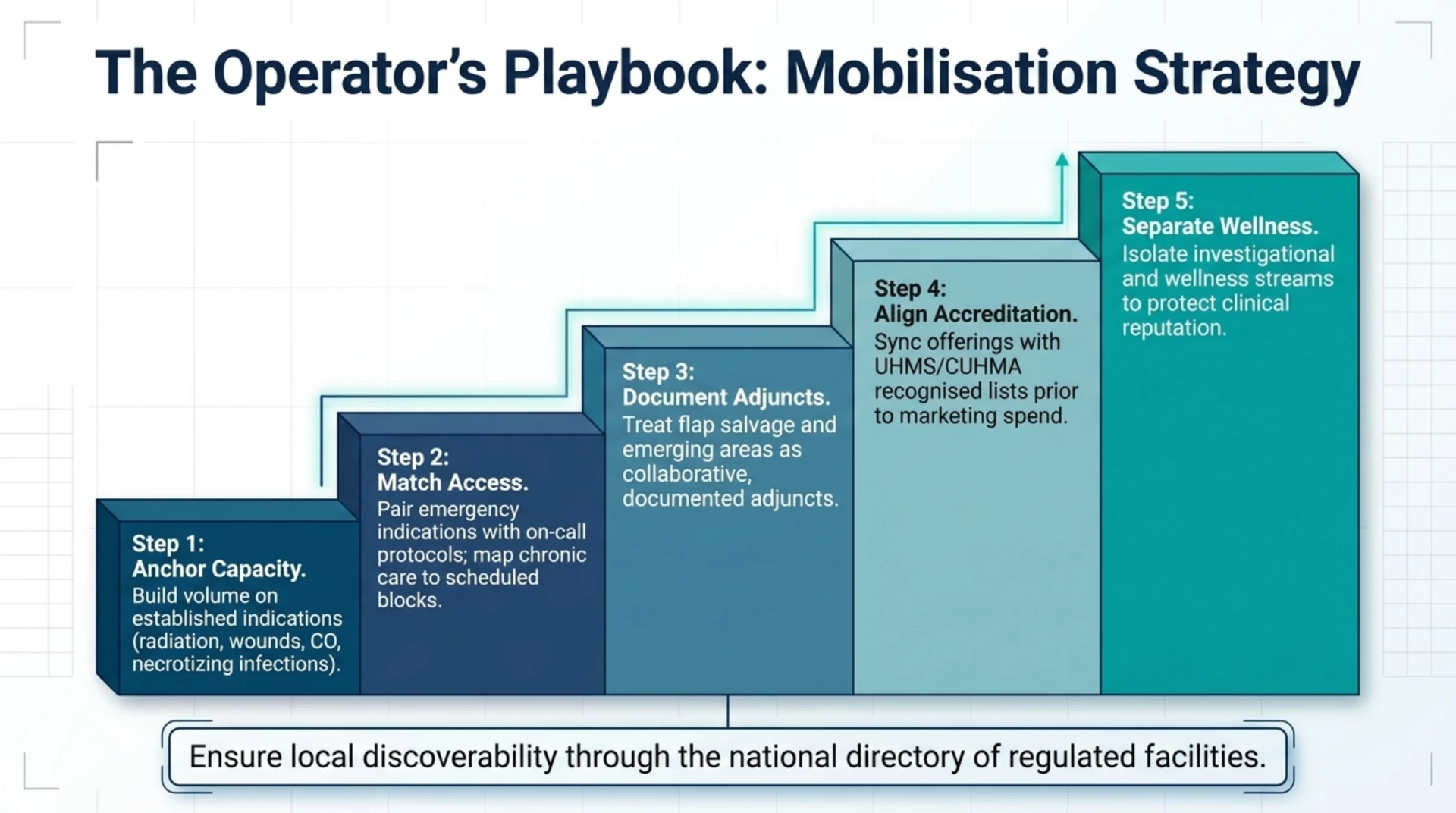
Translate evidence strength into concrete operating decisions with a short, ordered checklist:
- Anchor your core capacity on established indications – radiation injury, necrotizing infection, carbon monoxide, and chronic wounds – because they draw the steadiest, most defensible referrals.
- Match your access model to the indication: emergency lines need rapid-access and on-call protocols, while radiation and wound care fill scheduled blocks.
- Treat emerging areas such as flap salvage as documented, collaborative adjuncts, not headline offerings.
- Align your service lines with the recognised indication list and your accreditation goals before you invest in marketing.
- Keep investigational and wellness services in a separate, clearly labelled stream.
Referral demand also follows access. Patients and physicians increasingly search for local options, so make sure your programme is discoverable through the national directory of hospitals and regulated facilities and that your condition pages reflect only the indications your evidence supports.
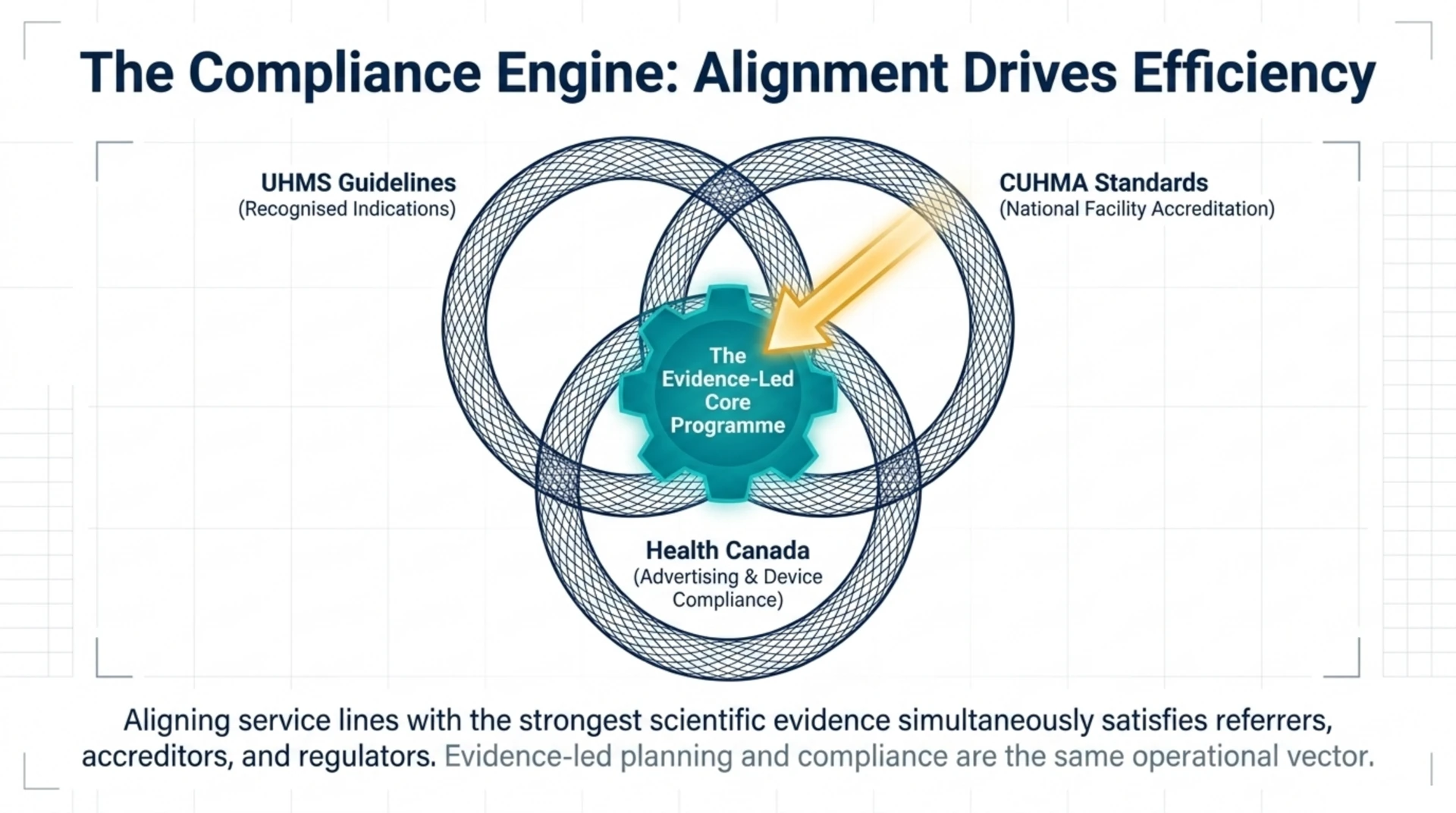
How do accreditation and national standards shape these choices?
Service-line planning does not happen in a vacuum. National coordination through the Canadian Undersea and Hyperbaric Medical Association (CUHMA) and the recognised indication framework maintained by the UHMS give operators a shared reference for which conditions belong in a credible programme. Aligning your strongest service lines with those references streamlines accreditation, supports clean documentation, and keeps your advertising within Health Canada guidance. In short, the conditions with the best evidence are also the ones the standards bodies already recognise, which is why evidence-led planning and compliance tend to point the same way.
Frequently asked questions
What is a hyperbaric service line?
A hyperbaric service line is a clinical programme built around a specific condition or referral pathway, including the staff training, chamber capacity, documentation, and outreach that support it. Most clinics run several service lines at once, such as wound care alongside radiation-injury treatment.
Which HBOT indications have the strongest evidence in 2026?
In 2026, delayed radiation tissue injury, necrotizing soft-tissue infection, carbon monoxide poisoning, and chronic or diabetic wound care carry the most consistent peer-reviewed support. These conditions also appear on the UHMS list of recognised indications, which makes them the most defensible foundation for a clinic.
Is hyperbaric oxygen therapy proven for surgical flap salvage?
Not definitively. Single-arm data show encouraging flap-salvage rates, but comparative studies have not consistently shown that HBOT reduces necrosis or reoperation, so the evidence remains low-certainty. Operators should offer it as a documented, collaborative adjunct rather than an established indication.
How does evidence strength affect referrals and compliance?
Well-evidenced indications attract steadier physician referrals and are easier to defend to accreditors and payers. Marketing weakly evidenced uses can create advertising-compliance risk under Health Canada rules, so aligning service lines with recognised indications protects both revenue and reputation.
Where can Canadian clinics confirm recognised indications?
The UHMS maintains the list of recognised hyperbaric indications, and CUHMA provides Canadian coordination, education, and facility listings. Reviewing both alongside current research helps operators keep their service lines credible and current.
How many HBOT service lines should a new clinic run?
There is no fixed number, but most Canadian clinics start with one or two established, high-referral service lines such as wound care and radiation injury, then add capacity as referral relationships mature. Building depth in evidence-anchored indications usually beats spreading thin across many.
Ready to see where treatment is delivered across the country? Explore the Canada Hyperbarics directory of hospitals and regulated facilities to understand the current Canadian landscape and where referral demand is concentrated.
This content is for informational purposes only and does not constitute medical advice. It is intended as evidence and industry intelligence for clinic owners and operators, not as clinical guidance for treating patients. Always consult qualified medical professionals and current regulatory guidance before making clinical or operational decisions.