Reading time: about 9 minutes. Hyperbaric oxygen therapy (HBOT) is a medical treatment in which a patient breathes 100% oxygen inside a pressurised chamber. This content is for informational purposes only and does not constitute medical advice.
TL;DR: Avascular necrosis (AVN) of the femoral head became the newest UHMS-recognised indication for hyperbaric oxygen therapy (HBOT) in 2024. A 2025 systematic review and several 2024-2026 cohort studies report encouraging improvements in pain and hip function, but the evidence base is dominated by small, single-centre, and uncontrolled studies. In the one pooled comparison, the difference between HBOT and non-HBOT groups did not reach statistical significance. Adequately powered randomised controlled trials remain the central research gap. Canada Hyperbarics tracks this literature as it develops.
Avascular necrosis (AVN) is bone death, also called osteonecrosis, that occurs when the blood supply to a section of bone is interrupted. In the femoral head it is a progressive and often disabling condition that frequently ends in structural collapse and total hip replacement. Hyperbaric oxygen therapy (HBOT) has emerged as an adjunctive, hip-preserving option, and in 2024 the Undersea and Hyperbaric Medical Society added AVN to its Indications list as the 15th recognised indication. This evidence review summarises the 2024-2026 literature on HBOT for femoral head osteonecrosis for a research audience, with attention to study design and the gap between encouraging signals and confirmatory trials.
What is avascular necrosis, and why does it matter for hyperbaric medicine?
Osteonecrosis of the femoral head (ONFH) results from disrupted perfusion, ischaemia, and the death of bone and marrow tissue. It commonly affects younger and working-age adults, which makes joint preservation a priority because early hip replacement is undesirable in this group. A 2025 systematic review of hip joint-preserving strategies noted that the prevalence of ONFH is rising and that the patient population is becoming younger, so early-stage interventions that delay or avoid arthroplasty carry significant clinical and socioeconomic value (Qi et al., 2025, PubMed | Our Assessment).
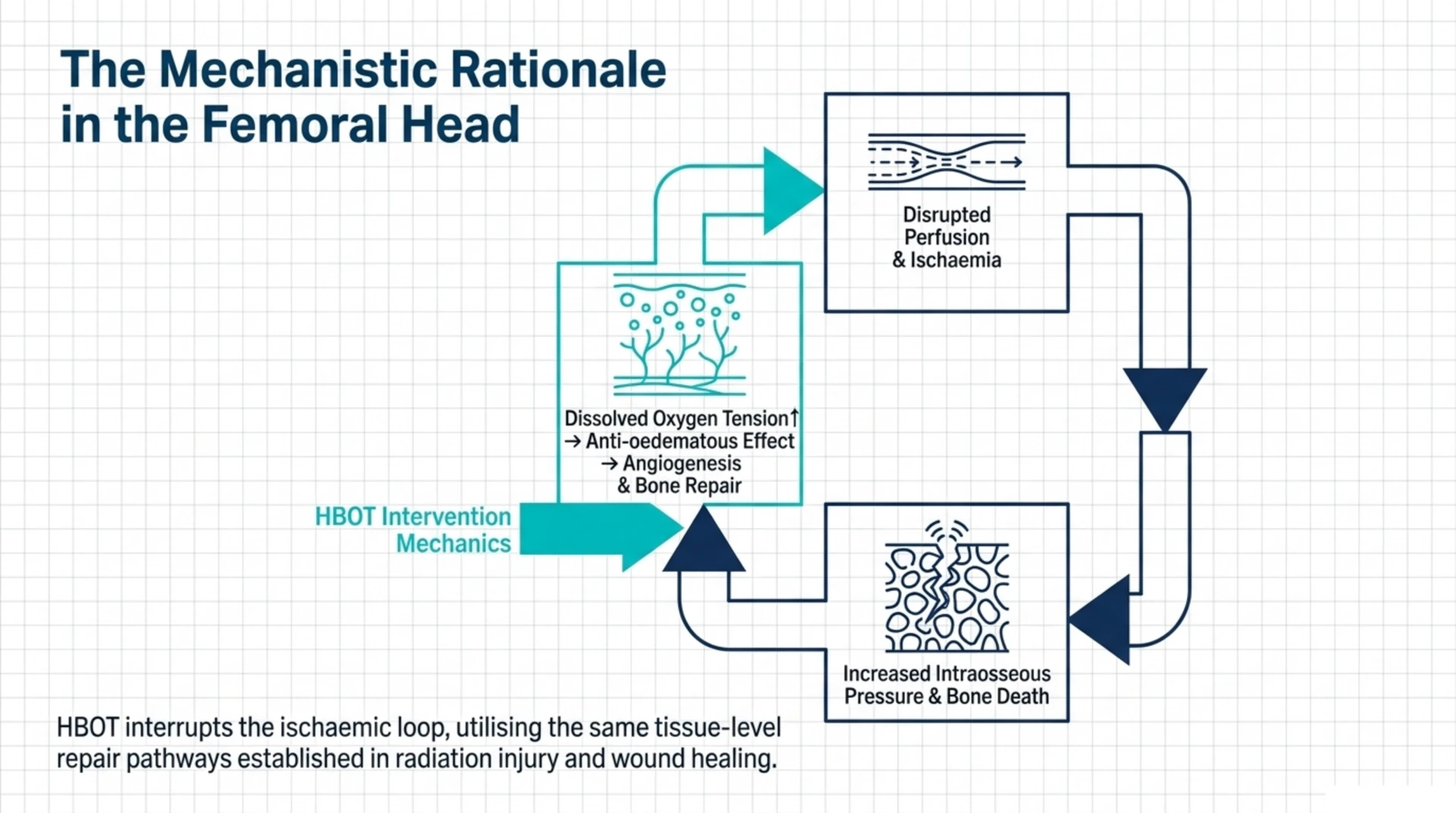
The mechanistic rationale for HBOT in AVN is straightforward. The therapy raises dissolved oxygen tension in ischaemic tissue, has an anti-oedematous effect that can lower intraosseous pressure, and is associated with angiogenesis and bone repair. These are the same tissue-level effects that underpin HBOT’s established wound-healing and radiation-injury roles, which is part of why hyperbaric researchers have long studied osteonecrosis. Canada Hyperbarics maintains a searchable bank of these studies in its research library.
Is avascular necrosis a recognised indication for hyperbaric oxygen therapy?
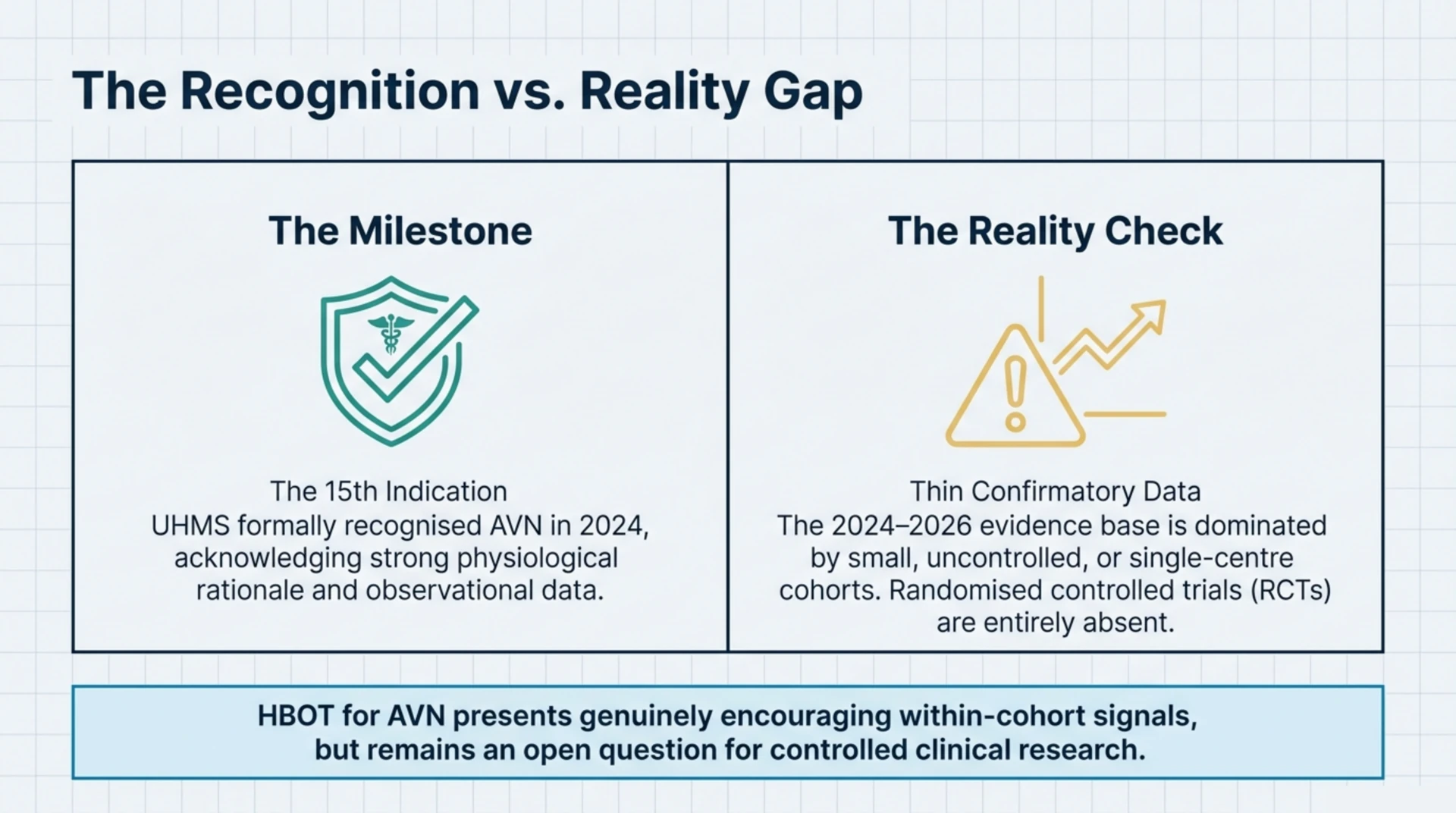
Yes, but with an important Canadian caveat. The Undersea and Hyperbaric Medical Society (UHMS) Indications list added avascular necrosis (aseptic osteonecrosis) in its 15th-edition manual in 2024, making it the 15th and newest UHMS-recognised indication (UHMS announcement, 2024). It is important not to conflate this with Canadian regulatory status. Health Canada recognises 14 conditions for hyperbaric chamber licensing, and AVN is not among them. The UHMS list and the Health Canada list are separate frameworks that only partially overlap, so in Canada AVN remains outside the publicly funded indication set even though it is now UHMS-recognised.
For researchers, this recency is the headline. A condition added to the recognised list in 2024 has, by definition, a thinner randomised evidence base than long-standing indications, which is exactly what the 2024-2026 literature shows.
What does the 2025 meta-analysis show about HBOT for femoral head necrosis?
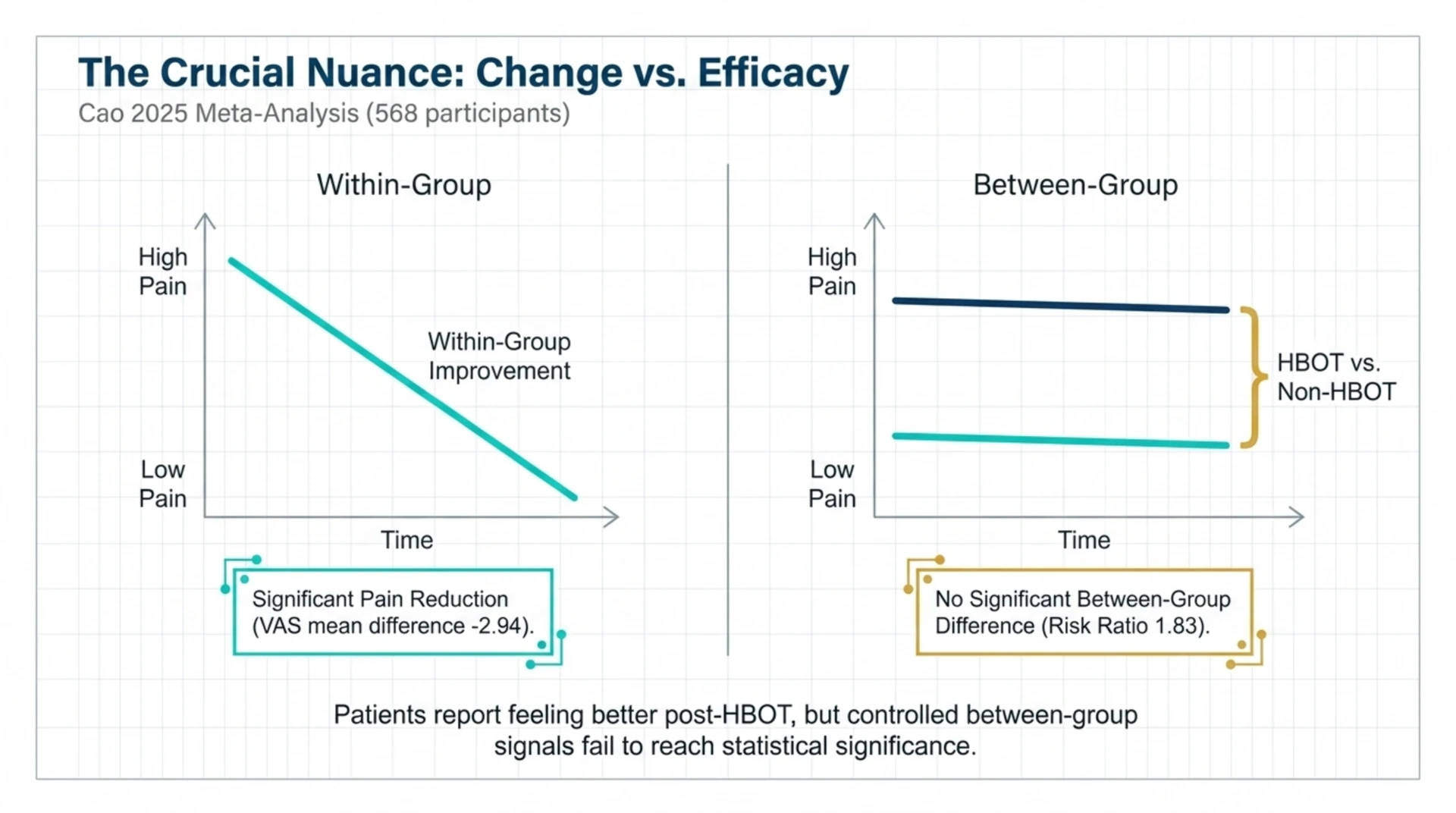
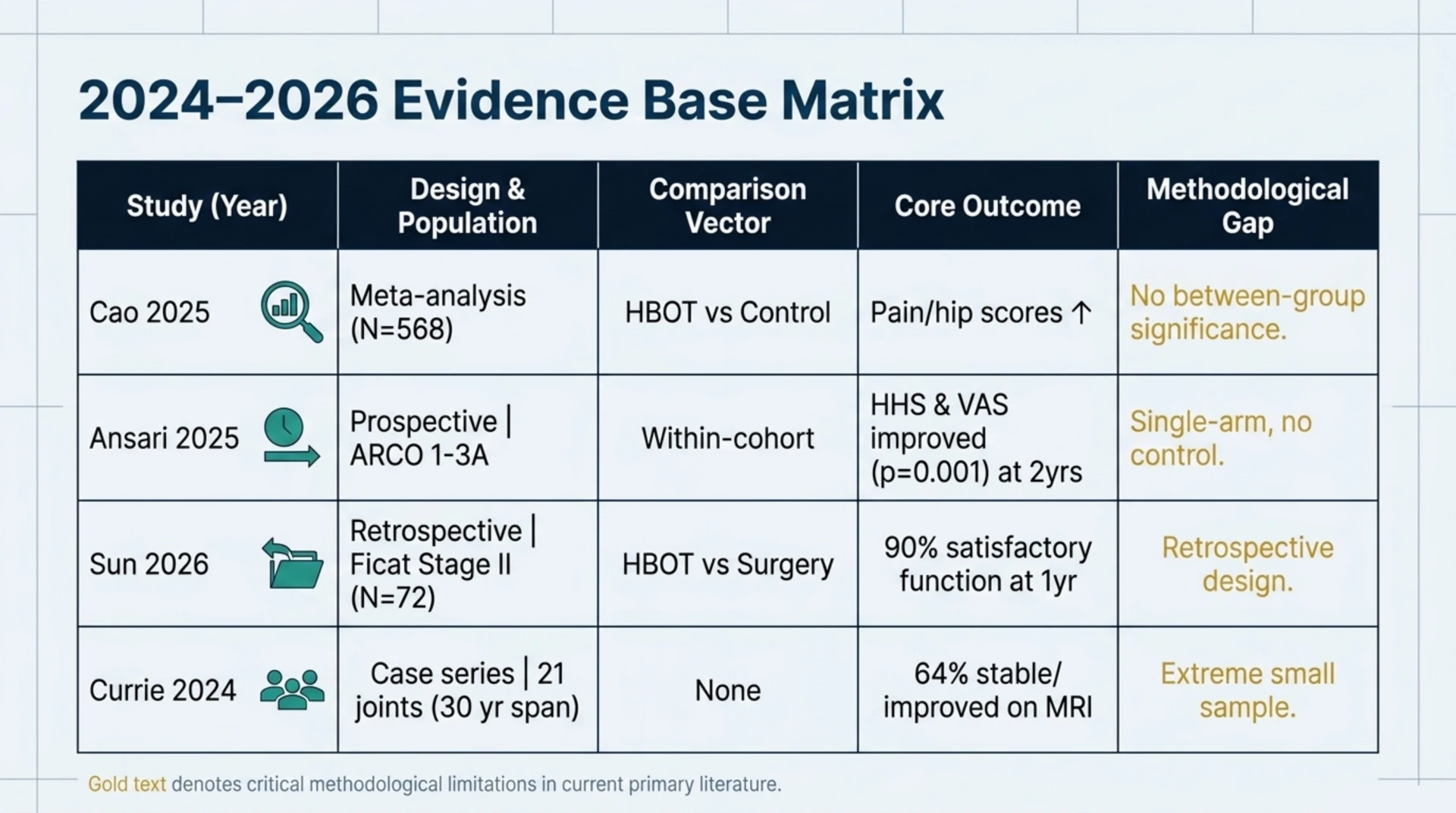
The most comprehensive synthesis to date is a 2025 systematic review and meta-analysis of HBOT for ONFH that pooled 10 studies and 568 participants (Cao et al., 2025, PubMed | Our Assessment). The pooled before-and-after analyses found statistically significant improvements after HBOT, including a reduction in pain on the visual analogue scale (mean difference -2.94, 95% CI -4.27 to -1.60) and improvements in physical and mental quality-of-life scores and in modified Harris Hip Score.
The key nuance is the comparison against controls. When the review compared HBOT groups with non-HBOT groups, the differences in quality-of-life summary scores and in the proportion of patients who improved were not statistically significant (for example, improved-patient events showed a risk ratio of 1.83, 95% CI 0.37 to 9.09). In other words, patients tended to be better off after HBOT than before it, but the controlled between-group signal was not significant in this pooled analysis. That distinction between within-group change and between-group effect is the single most important methodological point in this field, and it should temper any causal reading of the before-and-after data.
What do the most recent cohort and comparison studies report?
Three 2024-2026 studies add primary observational data. A 2025 prospective observational study enrolled patients with early-stage ONFH (ARCO stages 1 to 3A, non-traumatic), each treated with 5 HBOT sessions per week for a total of 35 sessions (Ansari et al., 2025, PubMed | Our Assessment). At two-year follow-up the cohort showed significant improvement in Harris Hip Score and visual analogue pain score (both p = 0.001) alongside radiological measures. The authors describe HBOT as effective, safe, and non-invasive for early ONFH, but they explicitly state that its role in the early-collapse stage needs further validation by higher-level, large-scale randomised controlled trials. Because this was a single-arm study with no control group, the improvements are best read as within-cohort change rather than proof of a treatment effect.
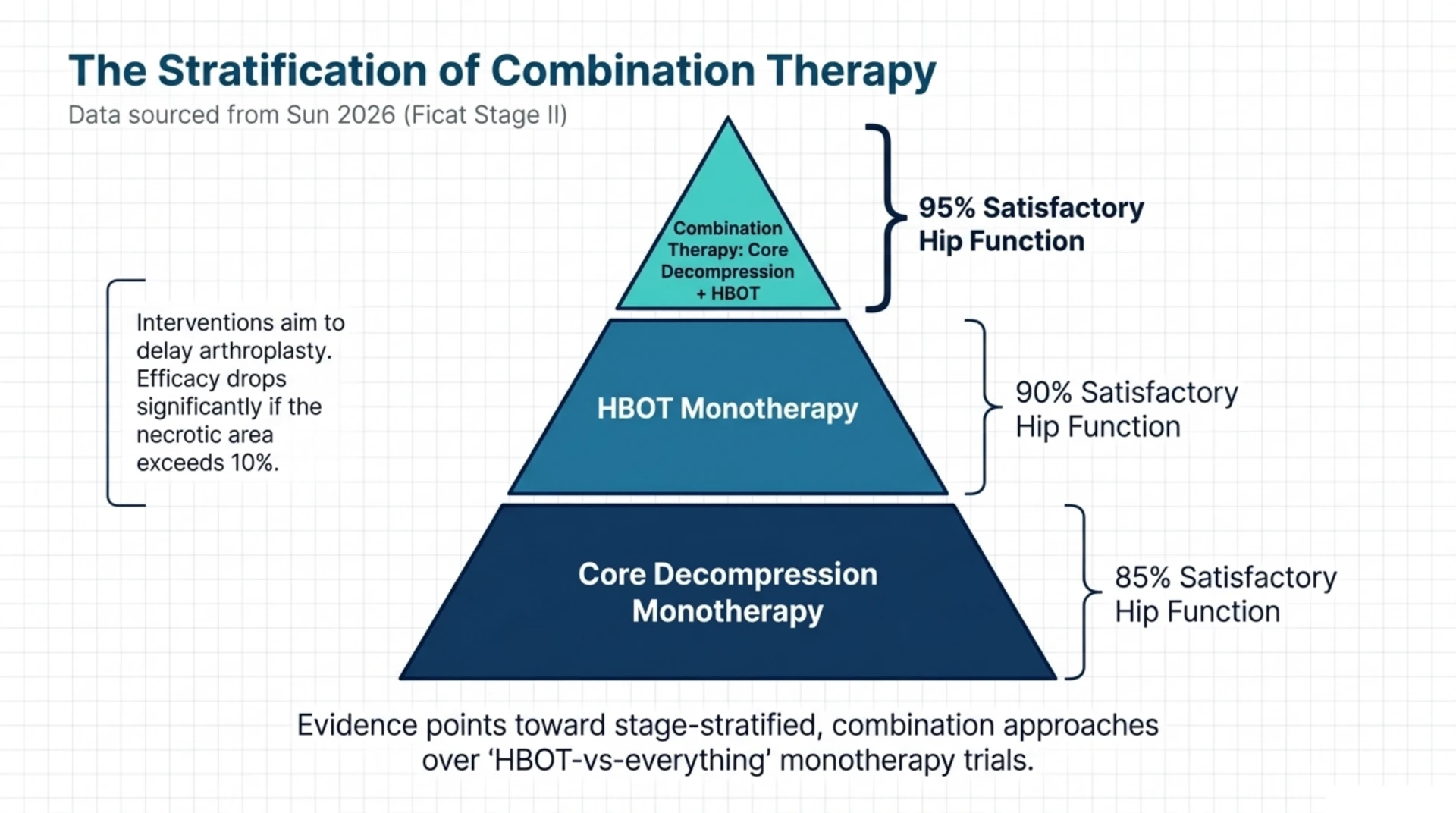
A 2026 retrospective study compared HBOT, core decompression, and the two combined in 72 patients with Ficat stage II non-traumatic osteonecrosis, divided evenly into three groups of 24 (Sun et al., 2026, PubMed | Our Assessment). After one year of follow-up, satisfactory improvement in hip-joint function was recorded in 90% of the HBOT group, 85% of the core-decompression group, and 95% of the combination group. The authors concluded that HBOT showed efficacy similar to core decompression and that the combination performed best, while acknowledging the retrospective design.
The longest real-world record comes from a 2024 retrospective chart review of a single Australian centre over roughly 30 years, covering 21 joints in 14 patients (14 femoral heads and 7 femoral condyles) (Currie et al., 2024, PubMed | Our Assessment). In the femoral-head group, 9 of 14 joints (64%) had stable or improved MRI appearance after treatment, 71% reported good subjective outcomes, and 3 joints still required surgical intervention. The most common adverse event was mild aural barotrauma in 3 patients. The very small sample size limits any firm inference, but the safety profile was consistent with HBOT’s broader record.
How do these AVN studies compare at a glance?
| Study (year, design) | Population | Comparison | Key reported outcome |
|---|---|---|---|
| Cao 2025 (systematic review / meta-analysis) | 10 studies, 568 participants | Within-group and HBOT vs non-HBOT | Significant before-after gains in pain and hip scores; no significant between-group difference |
| Ansari 2025 (prospective, single-arm) | Early ONFH (ARCO 1-3A), non-traumatic | None (within-cohort) | Harris Hip Score and VAS both improved at 2 years (p = 0.001); RCTs called for |
| Sun 2026 (retrospective) | 72 patients, Ficat stage II | HBOT vs core decompression vs both | Satisfactory hip function in 90% / 85% / 95% at 1 year |
| Currie 2024 (retrospective series, ~30 yr) | 14 patients, 21 joints | None (case series) | 64% of femoral-head joints stable/improved on MRI; mild barotrauma main adverse event |
How does HBOT fit among other hip-preserving strategies?
HBOT is one of several non-operative options, and it should be understood in that context rather than as a standalone cure. The 2025 review of hip-preserving strategies grouped HBOT with protective weight-bearing, pulsed electromagnetic fields, extracorporeal shockwave, bisphosphonates, anticoagulants, and other conservative measures (Qi et al., 2025, PubMed | Our Assessment). The authors observed that non-operative treatments aim to slow disease progression and delay joint replacement, but that they usually cannot effectively prevent progression except when the necrotic area is small (under 10%). That framing is consistent with the Sun comparison, where combining HBOT with core decompression performed best, and it points researchers toward stage-stratified and combination-therapy questions rather than HBOT-versus-everything comparisons.
Why is research interest in avascular necrosis growing?
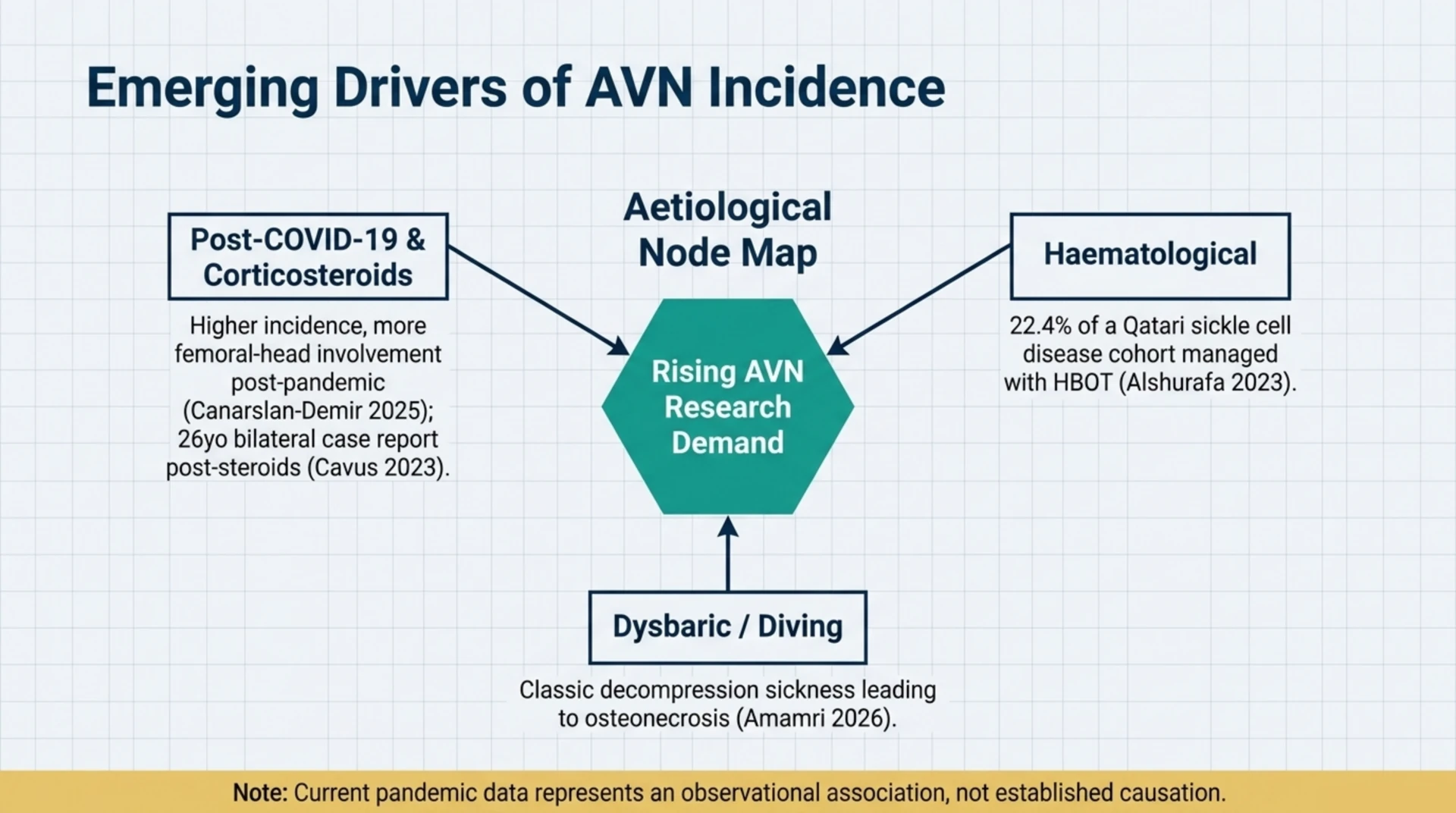
Several converging aetiologies are pushing AVN up the research agenda. A 2025 retrospective cohort study compared patients diagnosed with AVN before and after the COVID-19 pandemic and reported a significant increase in cases afterward, with a higher incidence of femoral-head involvement and more advanced stages among patients with a history of COVID-19 (Canarslan-Demir et al., 2025, PubMed | Our Assessment). The authors suggested that COVID-19 and high-dose steroid use may be associated with increased AVN risk, while calling for further study of the link. Because this is an observational cohort, the relationship is an association rather than established causation.
Corticosteroid exposure is a recurring theme. A 2023 case report described bilateral femoral and humeral head AVN in a 26-year-old man after a one-month course of oral corticosteroids, managed with a multimodal regimen that included HBOT, antiplatelet therapy, rehabilitation, and bilateral core decompression, with a favourable three-year outcome (Cavus et al., 2023, PubMed | Our Assessment). Because several treatments were given together, the case cannot isolate the contribution of HBOT, which is typical of the case-report tier of this evidence.
Haematological and diving aetiologies round out the picture. A 2023 cross-sectional study of 49 adults with sickle cell disease and AVN in Qatar found that most had multiple-joint and bilateral hip involvement, and that 11 patients (22.4%) were managed with hyperbaric oxygen, which the authors recorded as giving a good response within a descriptive series (Alshurafa et al., 2023, PubMed | Our Assessment). Separately, a 2026 case series of divers in Algeria documented dysbaric osteonecrosis following decompression sickness, a reminder that osteonecrosis is also a recognised diving-medicine concern (Amamri et al., 2026, PubMed | Our Assessment).
What are the research gaps and limitations?
The limitations are consistent across the literature. Sample sizes are small, many studies are retrospective or single-arm, staging systems differ (Ficat, ARCO, JIC), and HBOT protocols vary in pressure, session count, and co-interventions. The meta-analysis that did include controlled comparisons found no significant between-group effect, and the strongest prospective study explicitly called for randomised trials. For researchers planning new work, the highest-value designs would be adequately powered, stage-stratified randomised controlled trials with standardised HBOT protocols, MRI-based primary endpoints, and pre-specified comparisons against or alongside core decompression. Until those exist, HBOT for AVN is best described as a recognised but still-emerging indication with promising but unconfirmed efficacy.
Frequently asked questions
Is HBOT proven to cure avascular necrosis of the hip?
No. Current evidence comes mostly from small, observational, or uncontrolled studies. They report encouraging improvements in pain and hip function, but the one pooled between-group meta-analysis did not show a statistically significant advantage, and researchers consistently call for randomised controlled trials before efficacy can be considered proven.
When was avascular necrosis recognised as a hyperbaric indication?
The UHMS added avascular necrosis (aseptic osteonecrosis) to its Indications list in the 15th-edition manual in 2024, making it the 15th and newest UHMS-recognised indication. It is not one of Health Canada’s 14 conditions for chamber licensing.
Which stage of femoral head necrosis is studied most for HBOT?
Early, pre-collapse disease. The 2025 prospective study enrolled ARCO stage 1 to 3A patients, and the 2026 comparison focused on Ficat stage II. Reviews suggest non-operative options, including HBOT, are most relevant when the necrotic area is small, while advanced collapse usually moves toward surgical management.
How is HBOT delivered for osteonecrosis in these studies?
Protocols vary, but daily sessions over several weeks are typical. The 2025 prospective study used 5 sessions per week for a total of 35 sessions. Pressure, total session count, and whether HBOT is combined with surgery differ between studies, which is one reason results are hard to pool.
Could COVID-19 be increasing avascular necrosis cases?
An observational cohort reported more AVN cases after the pandemic, with more femoral-head involvement and more advanced stages in patients with prior COVID-19, and suggested that the infection and high-dose steroid use may be associated with increased risk. This is an association that needs further research, not established causation.
Where can clinicians and researchers access HBOT in Canada?
Hyperbaric oxygen therapy is delivered at hospitals and regulated facilities across the country. You can browse the directory of Canadian programmes on the Canada Hyperbarics facilities page, and review what public plans do and do not fund on the coverage guide.
The bottom line for researchers
Avascular necrosis is the newest UHMS-recognised indication for hyperbaric oxygen therapy, and the 2024-2026 literature offers genuinely encouraging within-cohort signals on pain and hip function. The evidence remains early: small, heterogeneous, and short on randomised controlled comparisons, with the one pooled between-group analysis falling short of significance. That combination of recognition plus thin confirmatory data makes AVN one of the more interesting open questions in clinical hyperbaric research. Canada Hyperbarics will continue to summarise new studies as they are published in its research library.
Medical disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Hyperbaric oxygen therapy for avascular necrosis is an emerging area of research. Always consult a qualified healthcare professional about your individual circumstances. Canada Hyperbarics is an independent informational resource and is not affiliated with any specific clinic.