
Hyperbaric oxygen therapy and stem cell mobilization refers to the observation that exposure to 100% oxygen at pressures above one atmosphere absolute (ATA) is associated with a measurable rise in circulating bone-marrow-derived stem and progenitor cells, particularly endothelial progenitor cells (EPCs). Across 21 published studies in the Canada Hyperbarics research database, the mechanism has been traced from foundational animal work in 2006 to a 2025 cohort study in umbilical cord blood transplantation, with the strongest clinical signal sitting in diabetic wound healing.
TL;DR: A 20-year body of evidence indicates that hyperbaric oxygen therapy (HBOT) is associated with mobilization of bone-marrow CD34+ endothelial progenitor cells into peripheral blood, mediated by an endothelial nitric oxide synthase (eNOS) and nitric oxide (NO) cascade. The clinical signal is strongest and most reproducible in diabetic wound healing and peripheral arterial occlusive disease. A 2019 head-and-neck irradiation cohort and a 2023 healthy-volunteer hyperbaric air study highlight that the effect is dose-dependent, population-dependent, and not exclusive to 100% oxygen. Most clinical evidence is observational, preclinical, or small single-centre work, so causal verbs should be reserved for the randomised data.
What is endothelial progenitor cell mobilization, and why does it matter for HBOT?
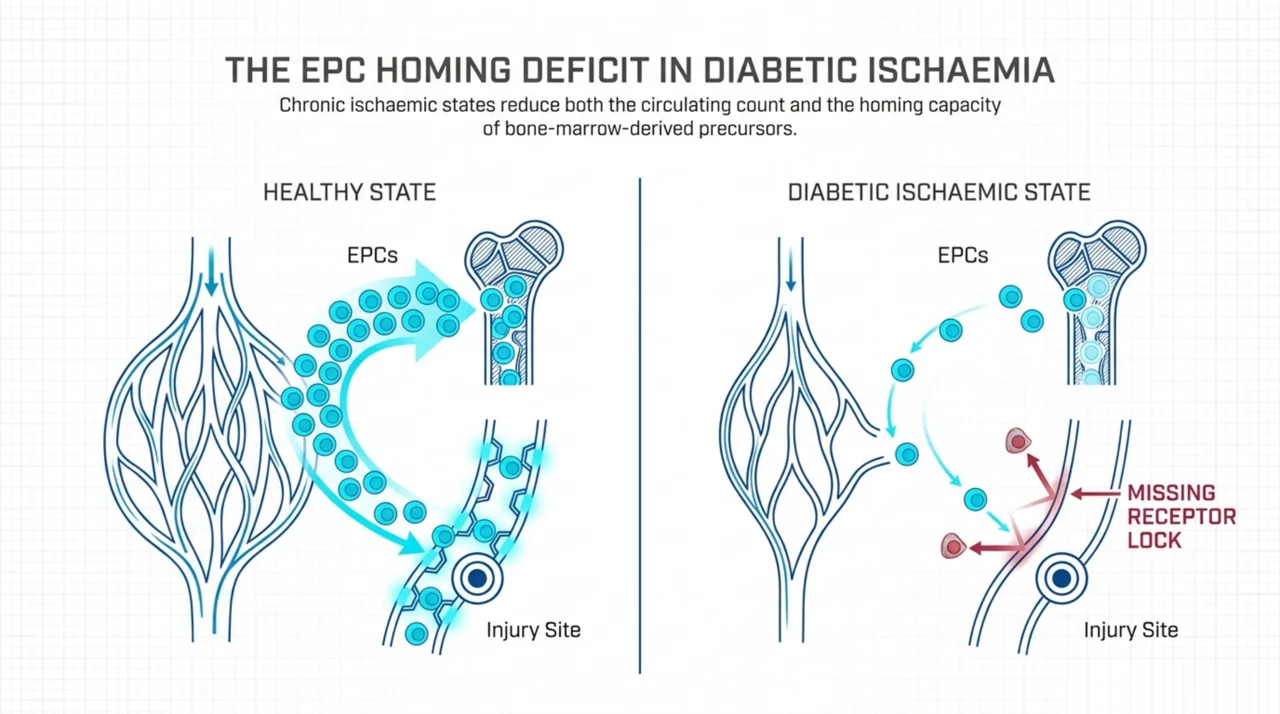
Endothelial progenitor cells (EPCs) are bone-marrow-derived precursors that home to sites of ischaemic or injured tissue and contribute to postnatal vasculogenesis. They are commonly identified by surface markers CD34+, CD133+, KDR+ (VEGFR-2), or various combinations of these. In healthy adults, EPCs circulate at low baseline frequencies. In diabetes, peripheral arterial disease, and chronic ischaemic states, both the circulating count and the homing capacity of EPCs are reduced, which is one of the proposed mechanisms behind delayed wound healing in those populations.
The interest in HBOT as an EPC-mobilizing intervention comes from a series of mechanistic studies showing that hyperoxia, induced by a clinically relevant HBOT protocol, was associated with increased mobilization of EPCs from bone marrow into peripheral blood, through an endothelial nitric oxide synthase and nitric oxide (eNOS-NO) cascade that the diabetic state otherwise impairs. The clinical hypothesis is that this mobilization, combined with HBOT-driven changes at the wound bed, contributes to angiogenesis and tissue repair.
How did the foundational 2006-2008 work establish the mechanism?
The earliest review of HBOT and bone-marrow-derived EPCs in diabetic wound healing came from a 2006 paper by Gallagher and colleagues (PubMed | Our Assessment). The authors reviewed evidence indicating that tissue-level hyperoxia achieved by therapeutic HBOT protocols was associated with increased mobilization of EPCs from the bone marrow into peripheral blood, and proposed this as a candidate mechanism for improving healing in chronic wounds affected by diabetes and peripheral arterial disease.
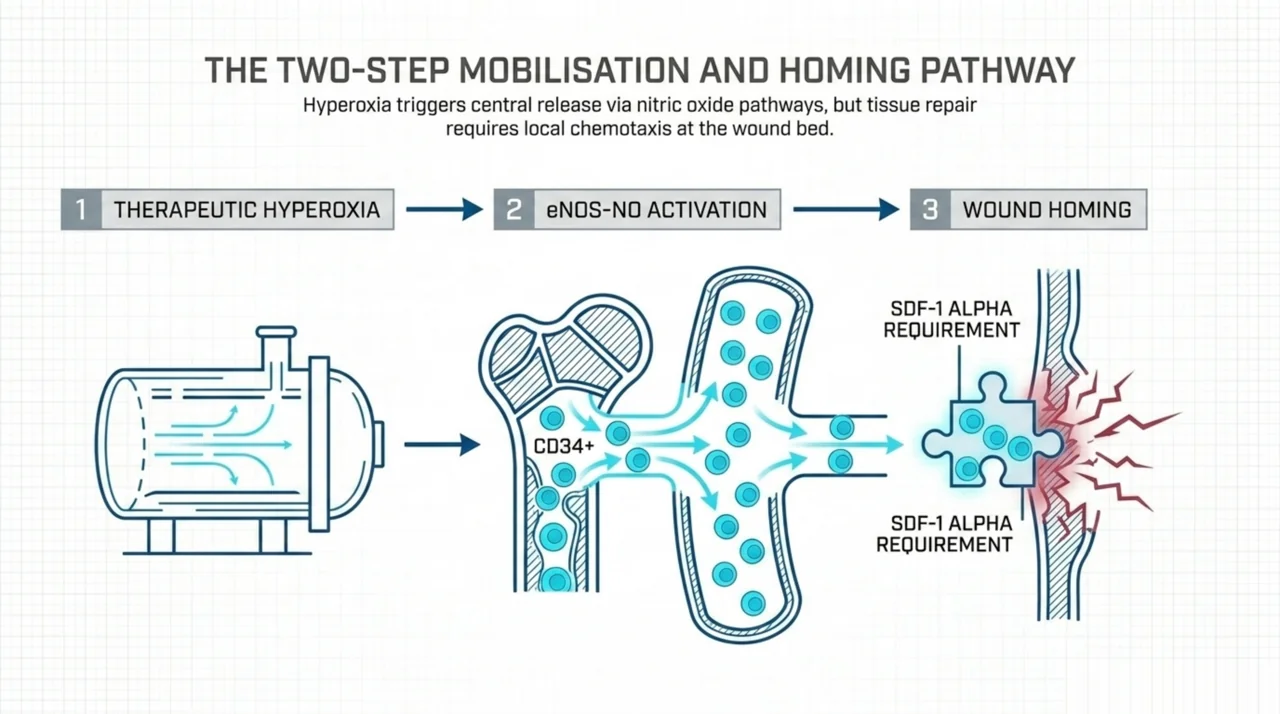
A 2008 paper by Liu and colleagues in Antioxidants and Redox Signaling (PubMed | Our Assessment) extended the mechanism into an explicit two-step model: hyperoxia under a clinically relevant HBOT protocol significantly enhanced EPC mobilization from bone marrow into peripheral blood through the eNOS-NO cascade, but increased circulating EPCs failed to reach wound tissues, in part because of downregulated stromal cell-derived factor-1 alpha (SDF-1 alpha) at the diabetic wound. Administration of exogenous SDF-1 alpha reversed the EPC homing impairment and, when combined with hyperoxia, was associated with synergistic enhancement of EPC mobilization, homing, neovascularization, and wound healing in animal models. This paper anchors the mobilization-versus-homing distinction that subsequent clinical studies have wrestled with.
Where is the strongest clinical signal: diabetic wound healing?
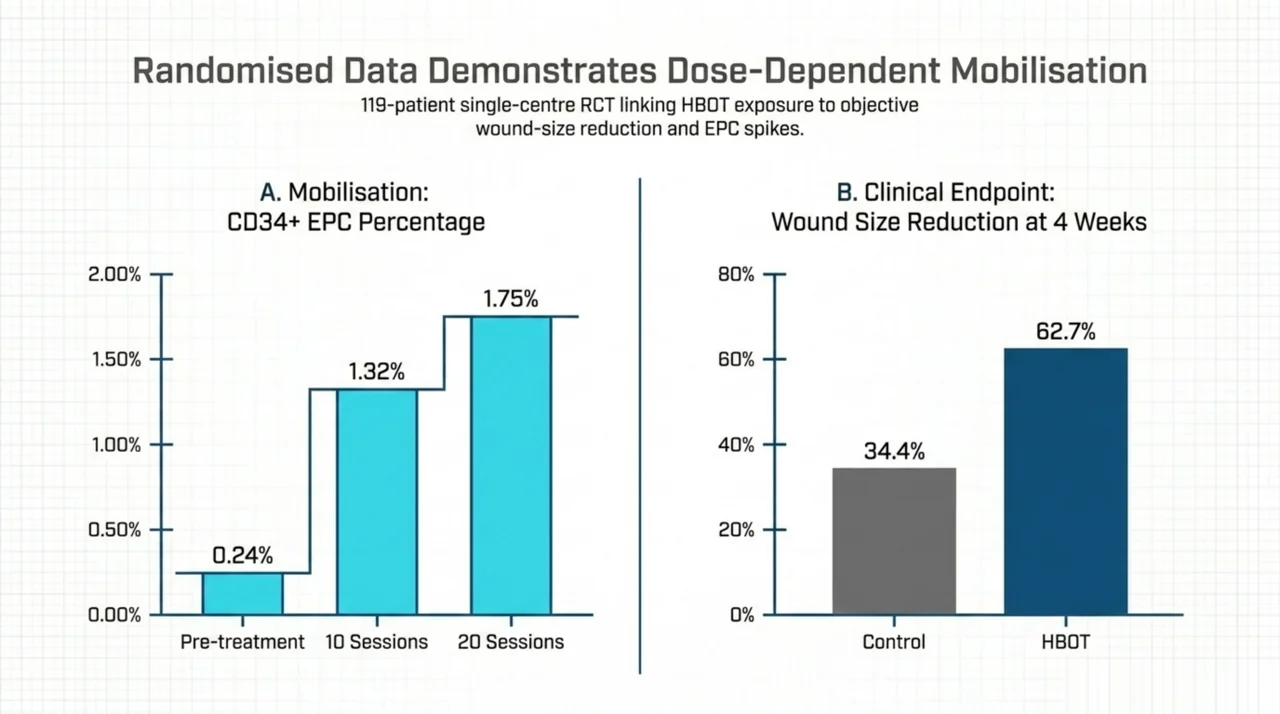
The most clinically translated signal sits in diabetic chronic wound healing. A 2011 single-centre randomised placebo-controlled trial by Ma and colleagues (PubMed | Our Assessment) enrolled 119 patients with chronic lower-extremity wounds lasting more than three months. Of these, 97 received HBOT (90 minute daily exposures, five days per week for four weeks) and 22 received hyperbaric air as the control arm. The peripheral CD34+ EPC average count rose from 0.24 plus or minus 0.03% pre-treatment to 1.32 plus or minus 0.05% after 10 HBOT sessions and 1.75 plus or minus 0.17% after 20 sessions, both significantly above pre-treatment values. Wound size decreased by 62.7 plus or minus 22.3% in the HBOT group at the 4-week endpoint, compared with 34.4 plus or minus 20.6% in the control group (p < 0.05). The CD34/CXCR4 and CD34/Sca-1+ dual-positive populations were similarly elevated. This is the strongest study in the pool linking HBOT exposure, EPC mobilization, and an objective wound-size endpoint within a single randomised design.
A 2022 rat study by Nasiry and colleagues (PubMed | Our Assessment) extended the Liu 2008 mobilization-versus-homing model by testing an SDF-1 alpha loaded amniotic membrane scaffold combined with HBOT in a diabetic rat ischaemic wound model. Wound closure, new dermis and epidermis volume, blood-vessel numerical density, collagen deposition, biomechanical properties, and VEGF, bFGF, and TGF-beta transcripts were all highest in the combined SDF-1 alpha scaffold plus HBOT group, supporting the hypothesis that mobilization gains are amplified when homing chemotaxis is restored at the wound bed. The clinical translation of this combined approach in humans remains to be tested.
A 2013 narrative review by Goldstein in Dermatologic Therapy (PubMed | Our Assessment) summarized this body of work for clinicians, noting that HBOT was associated with increased growth factors and local wound signaling while also promoting a central release of EPCs from the bone marrow via nitric oxide pathways, and cited accumulating clinical data supporting HBOT use to hasten chronic wound healing in appropriate patients.
What does the peripheral arterial disease evidence add?
Peripheral arterial occlusive disease (PAOD) is the second cluster where HBOT-EPC mobilization has been tested in humans. A 2018 prospective observational study by Lin and colleagues in Journal of Clinical Medicine (PubMed | Our Assessment) enrolled 57 consecutive PAOD patients receiving HBOT at 3 ATA for two hours. Circulating CD34+/CD133+/CD45dim EPCs, soluble angiogenesis factors, and skin perfusion pressure (an indicator of blood flow in ischaemic areas) were measured before and across five HBOT sessions. The authors reported that HBOT was associated with augmented circulating EPC levels, increased angiogenesis factors, and improved blood flow in the ischaemic area. Because the design was single-arm observational, the change cannot be attributed causally to HBOT alone.
A 2020 translational study by Chen and colleagues in International Journal of Molecular Sciences (PubMed | Our Assessment) took the next step by harvesting circulatory EPCs from PAOD patients who had received combined autologous CD34+ cell and HBO therapy, then testing whether these “rejuvenated” EPCs could salvage nude-mouse limbs against critical limb ischaemia. The result is mechanistic and supportive of a functional benefit to the mobilized EPC pool, but the design is preclinical and does not constitute a clinical efficacy trial.
For broader peripheral arterial disease context, see our companion 2026 PAOD evidence review for referring physicians, which synthesizes the Knezevic 2026 platelet-aggregation cohort alongside the EPC literature.
Is there a central nervous system signal?
A 2018 prospective study by Chen and colleagues in Journal of Translational Medicine (PubMed | Our Assessment) enrolled 25 acute non-cardioembolic stroke patients treated with HBOT and 25 disease controls. KDR+/CD34+ EPCs increased significantly after HBOT, while CD133+/CD34+ EPCs showed a non-significant upward tendency. High-sensitivity C-reactive protein decreased significantly post-HBOT. Importantly, changes in KDR+/CD34+ EPC numbers correlated positively with changes in clinical outcomes (Barthel Index, National Institutes of Health Stroke Scale, and modified Rankin Scale) in the HBOT group. The authors concluded that HBOT was associated with both improved short-term clinical outcomes and increased circulating EPCs, but the small sample and observational design constrain the strength of inference.
A 2024 narrative review by Barata and colleagues in Cureus (PubMed | Our Assessment) frames adult neurogenesis as a high-energy-demand process for which blood vessels and the “oxygen niche” supplying progenitor cells are critical. The authors argue that HBOT functions both as a neuroprotective intervention and a candidate neuroregenerative one across various brain-injury models, but the review remains hypothesis-generating rather than confirmatory for human cognitive outcomes.
A 2025 rat study by Ho and colleagues in International Journal of Medical Sciences (PubMed | Our Assessment) reported that HBOT was associated with prevention and reversal of whole-brain-radiotherapy-induced cognitive deficits, hippocampal microgliosis, neuronal-progenitor apoptosis, and lipid peroxidation in a controlled animal model. This is preclinical, but it places progenitor-cell protection within the radiation-injury indication, an area of established clinical use for HBOT.
Does the mobilization effect require 100% oxygen, or does pressure alone do part of the work?
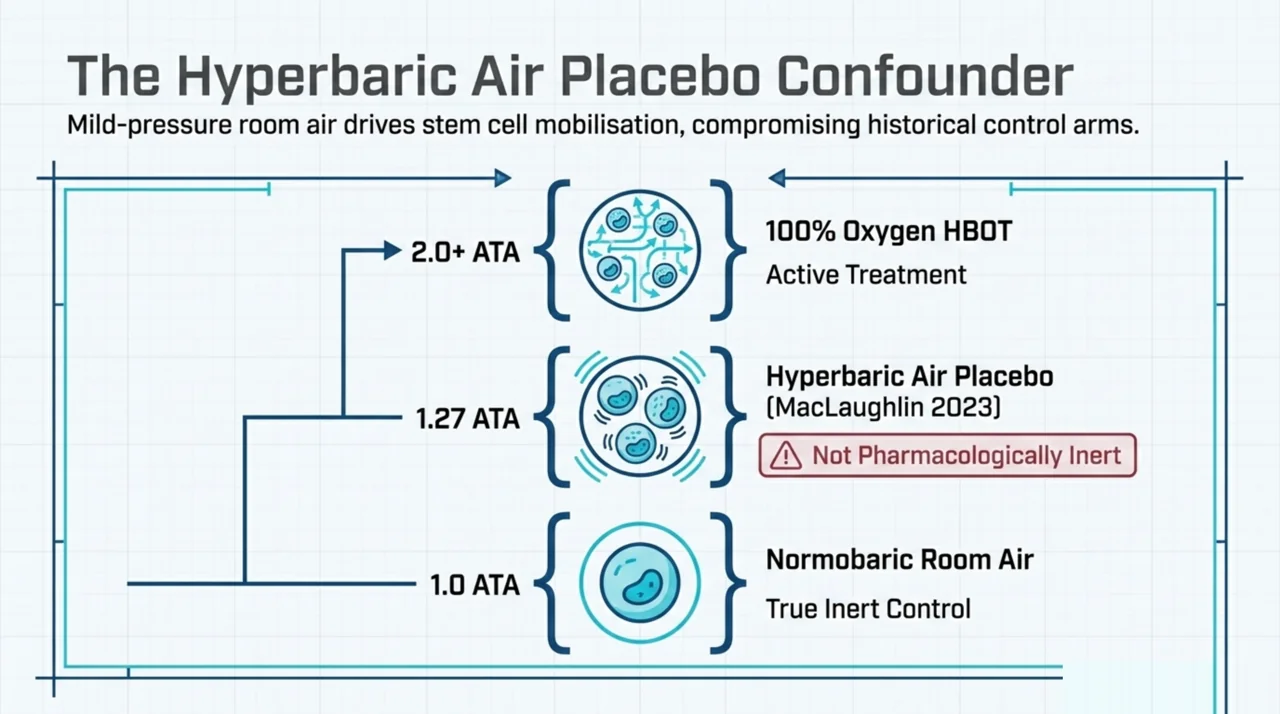
The dose-response question is sharpened by a 2023 study by MacLaughlin and colleagues in Frontiers in Neurology (PubMed | Our Assessment). The authors tested hyperbaric AIR (not 100% oxygen) at 1.27 ATA (4 psig / 965 mmHg) for 90 minutes daily over 10 exposures across two weeks in 10 healthy 34 to 35-year-old volunteers. Blood was sampled pre-first-exposure (each subject’s own control), after the first exposure, before the ninth, and three days after the final exposure. Stem and progenitor cells were gated by blinded flow cytometry. The historical framing is striking: before modern HBOT displaced air with 100% oxygen, hyperbaric air was used pharmaceutically as early as 1662, and the authors argue that the contribution of the 78% nitrogen fraction was never tested. The study reports that hyperbaric air mobilizes stem cells in humans, which the authors interpret as evidence for a hormetic dose curve in which mild-pressure room air also drives mobilization.
The Ma 2011 RCT discussed above used hyperbaric air as its placebo control. Read alongside MacLaughlin 2023, this suggests that the placebo arm in some prior trials may not have been pharmacologically inert with respect to EPC counts, which has methodological implications for any sham-controlled HBOT trial in which a stem-cell mobilization endpoint is being measured.
What does the umbilical cord blood transplantation work add?
A distinct clinical thread sits in haematopoietic engraftment after umbilical cord blood (UCB) transplantation. UCB transplants are limited by low stem and progenitor cell numbers and impaired homing, which cause delayed engraftment and higher rates of engraftment failure.
A 2013 murine study by Aljitawi and colleagues in Blood Cells, Molecules and Diseases (PubMed | Our Assessment) tested HBOT (2.5 ATA, 100% oxygen, 2 hours) in NSG mice four hours before transplant of expanded and gene-transduced human CD34+ UCB cells. HBOT-treated mice demonstrated significantly improved bone-marrow, peripheral-blood, and spleen retention and engraftment, with significantly higher bioluminescence values on in vivo imaging.
A 2016 paper in Blood by Aljitawi and colleagues (PubMed | Our Assessment) extended the work into a candidate mechanism: systemic reduction in erythropoietin (EPO) levels by HBOT in a preclinical mouse model and in a pilot clinical trial was associated with improved homing of transplanted UCB CD34+ cells to bone marrow. In the pilot human arm, HBOT before UCB transplantation was reported as well tolerated, with transient EPO reduction and encouraging engraftment kinetics, but the sample remained small and uncontrolled.
A 2025 paper by Abdelhakim and colleagues in Transfusion and Apheresis Science (PubMed | Our Assessment) reported a 15-subject HBOT-before-UCB cohort compared with historic institutional UCB recipients. In the first 100 days post-transplant, HBOT patients required fewer consecutive days of G-CSF support and achieved packed-red-blood-cell and platelet independence significantly faster than the historic group. This is the most recent clinical signal in the pool, and like the earlier Aljitawi work it is a small uncontrolled cohort with a historical comparator, so the result should be read as encouraging rather than definitive.
What are the negative and equivocal findings?
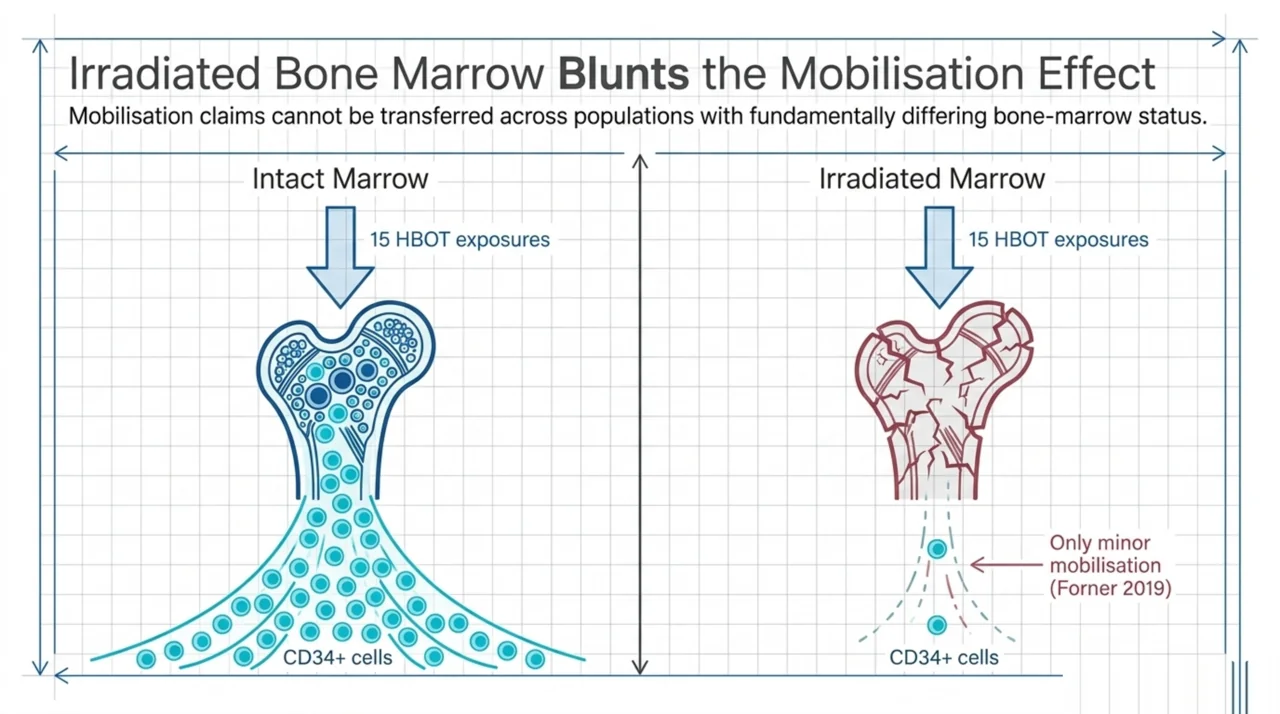
For balance, the most important negative dataset in the pool is a 2019 study by Forner and colleagues in Diving and Hyperbaric Medicine (PubMed | Our Assessment). Ten head-and-neck irradiated patients were enrolled (six completed the full 29 to 30 HBOT exposures). The authors measured CD34+CD45dim cell counts and aldehyde-dehydrogenase-positive stem/progenitor cells by flow cytometry. They reported a weak and insignificant tendency toward CD34+CD45dim mobilization after a single HBOT exposure, and an additive effect after 15 exposures that was statistically above zero but less than a doubling, with no significant effect on aldehyde-dehydrogenase-positive SPCs. The authors titled the paper “Only minor stem cell mobilization in head and neck irradiated patients,” which captures their conclusion. This dataset is a useful reminder that the mobilization signal observed in diabetic-wound and PAOD cohorts is not necessarily generalizable to irradiated populations in whom bone-marrow function may be compromised.
A 2019 review by Longobardi and colleagues in the same journal (PubMed | Our Assessment) summarized the case-series and case-report literature on HBOT for vasculitic, calcific uraemic, livedoid, and pyoderma-gangrenosum ulcers (63 participants across seven studies). The authors noted some evidence that HBOT may improve wound healing by increasing nitric oxide levels and EPC numbers, and they called for appropriately powered multi-centre randomised trials to establish efficacy. The methodological gap they describe in 2019 still characterizes most of the EPC-mobilization clinical literature: small samples, single-centre, observational or single-arm.
A 2017 review by Kanji and colleagues in Mediators of Inflammation (PubMed | Our Assessment) places HBOT-mediated EPC mobilization in the broader landscape of stem-cell therapeutics for cutaneous wound healing, and notes that the mechanisms by which mobilized progenitor cells contribute to healing have yet to be fully elucidated.
How do the findings sit by evidence design?
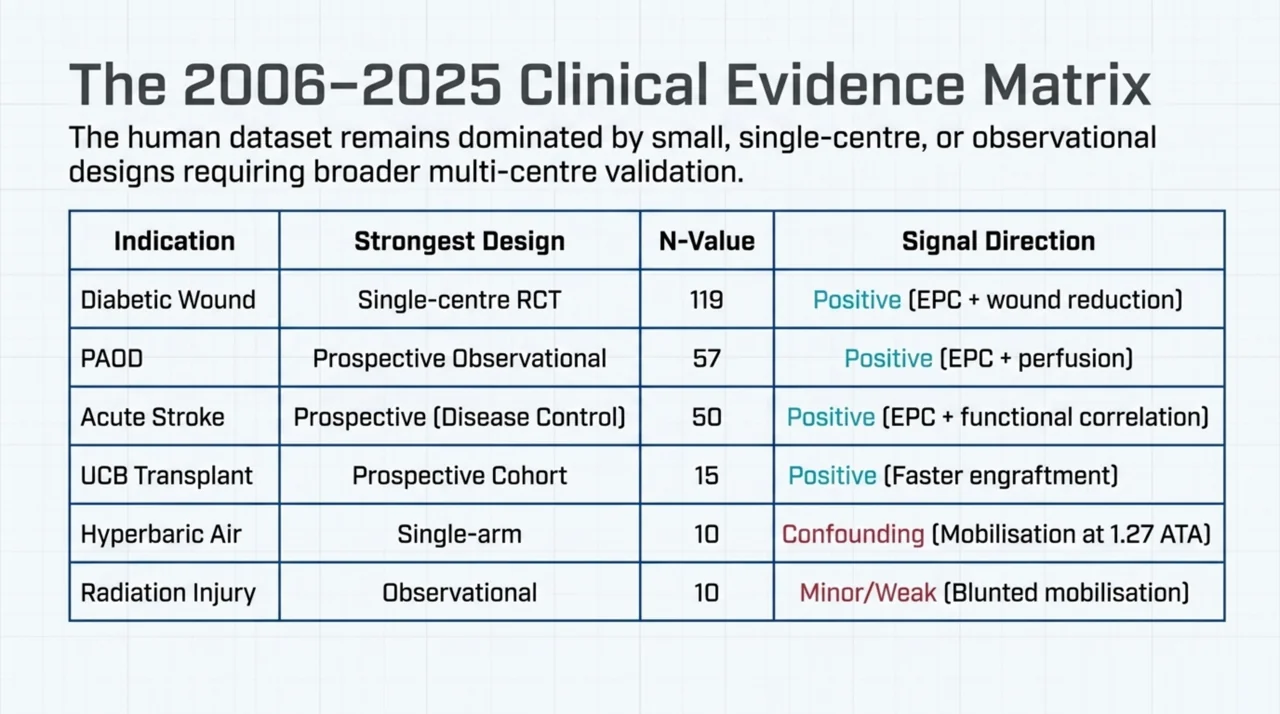
| Indication | Strongest design in pool | Direction of signal | Key reference |
|---|---|---|---|
| Diabetic chronic wound healing | Single-centre RCT (n=119) | EPC mobilization + wound-size reduction | Ma 2011 (PMID 22333107) |
| Peripheral arterial occlusive disease | Prospective observational (n=57) | EPC mobilization + perfusion improvement | Lin 2018 (PMID 30558177) |
| Acute non-cardioembolic stroke | Prospective with disease controls (n=25) | EPC mobilization + functional-score correlation | Chen 2018 (PMID 30208940) |
| Head and neck radiation injury | Observational (n=10 enrolled, 6 completed) | Only minor mobilization | Forner 2019 (PMID 31523792) |
| UCB transplant engraftment | Small prospective cohort vs historic controls (n=15) | Faster transfusion independence | Abdelhakim 2025 (PMID 40543291) |
| Healthy volunteers, hyperbaric air | Single-arm with each subject as own control (n=10) | Stem-cell mobilization with air at 1.27 ATA | MacLaughlin 2023 (PMID 37409020) |
What does this evidence base mean for Canadian researchers?
For Canadian investigators considering stem-cell mobilization as an HBOT mechanism endpoint, three observations follow from the pool.
- The mobilization signal is most reproducible in diabetic wound and PAOD cohorts. These remain the populations with the cleanest mechanistic rationale, the largest existing datasets, and a clinically meaningful endpoint that aligns with established HBOT indications. Future Canadian trials adding objective wound-area or perfusion endpoints alongside flow-cytometry EPC counts would extend, rather than replicate, the existing work.
- Sham control choice has measurable consequences. Hyperbaric air at low pressure (1.27 ATA) has been reported to mobilize stem cells in healthy volunteers, which calls into question whether hyperbaric-air “placebo” arms are pharmacologically inert for a mobilization endpoint. Designers of sham-controlled HBOT trials should report the partial pressure of oxygen in the sham arm explicitly and consider truly normobaric room-air comparators where feasible.
- Population matters: irradiated bone marrow behaves differently. The Forner 2019 dataset suggests that the EPC-mobilization response is reduced or absent in head-and-neck irradiation patients, even though HBOT is a well-established treatment for late radiation tissue injury through other mechanisms. Researchers should be cautious about transferring mobilization claims across populations with differing bone-marrow status.
For broader context on the Canadian HBOT research and care landscape, see the curated research database and the directory of hospitals and regulated facilities across the country. Recent Canadian-authored work indexed in our database includes the 2026 depression, PTSD and anxiety meta-analysis from the University of Toronto and Defence Research and Development Canada (see our summary).
Frequently asked questions
Is HBOT a stem-cell therapy?
No. HBOT is the delivery of 100% oxygen at greater than atmospheric pressure. It is not the administration of exogenous stem cells. The evidence reviewed here addresses HBOT’s association with mobilization of endogenous bone-marrow-derived stem and progenitor cells into peripheral circulation, which is a mechanism of action observation, not a therapy classification. Health Canada-recognised conditions for HBOT are defined by clinical condition (for example, decompression sickness, carbon monoxide poisoning, selected chronic wounds), not by cellular mechanism.
What surface markers identify the cells that HBOT mobilizes?
Across the studies reviewed, mobilization is most commonly quantified by flow cytometry as CD34+, CD133+, KDR+ (VEGFR-2), CD45dim, or combinations such as CD34+/CD133+/CD45dim, CD34/CXCR4, and CD34/Sca-1+. The Forner 2019 paper also assessed aldehyde dehydrogenase activity using the Aldefluor assay as a marker of stem-progenitor function.
What is the proposed mechanism?
The most cited mechanism is that tissue-level hyperoxia under a clinically relevant HBOT protocol activates an endothelial nitric oxide synthase and nitric oxide (eNOS-NO) cascade in bone marrow, which is associated with mobilization of EPCs into peripheral blood. The Liu 2008 paper additionally proposes that downregulated SDF-1 alpha at diabetic wound sites limits homing of mobilized EPCs to the wound bed, which is why exogenous SDF-1 alpha combined with hyperoxia was associated with synergistic effects in animal models.
How many HBOT sessions are needed to see a mobilization effect?
Reported protocols vary. The Ma 2011 RCT observed significant CD34+ EPC elevation after 10 sessions (1.32% versus 0.24% pre-treatment) with further elevation after 20 sessions (1.75%). The Lin 2018 PAOD study reported circulating EPC and perfusion changes across five HBOT sessions at 3 ATA for two hours. The MacLaughlin 2023 hyperbaric-air study observed effects in healthy volunteers across 10 exposures over two weeks. The Forner 2019 head-and-neck irradiation study observed only a sub-doubling effect after 15 exposures.
Is the mobilization claim a Health Canada-recognised condition?
No. Health Canada regulates hyperbaric chambers as medical devices and recognises specific clinical conditions for HBOT. “Stem-cell mobilization” is a mechanism of action observed in research, not a stand-alone treatment indication. Patients should not seek HBOT for stem-cell mobilization outside of a recognised indication or a properly approved clinical trial. See the regulatory overview and the indication-specific pages under conditions.
What are the main methodological gaps?
Most of the human evidence consists of single-centre, small, observational, or single-arm prospective studies. The one randomised trial in this pool (Ma 2011) is single-centre and uses hyperbaric air as a control, which the 2023 MacLaughlin data suggests may not be pharmacologically inert for a mobilization endpoint. Multi-centre, adequately powered randomised trials with mechanism-aligned endpoints and explicit sham-gas characterization remain the next major piece of work.
Where can I find the underlying studies?
Each study referenced in this article links to both PubMed and the Canada Hyperbarics structured assessment of that paper. The full research database, including filters by condition, year, and evidence type, is at canadahyperbarics.ca/research. For accredited HBOT delivery sites across Canada, see the directory of hospitals and regulated facilities.
The bottom line for researchers
Across 21 indexed studies spanning two decades, HBOT exposure is consistently associated with measurable mobilization of bone-marrow-derived endothelial progenitor cells into peripheral circulation, with the strongest clinical signal in diabetic wound healing and PAOD. The mechanism (an eNOS-NO cascade with SDF-1 alpha-mediated wound homing) is supported by animal data. The most important caveats are that human evidence is still dominated by small observational and single-arm studies, the mobilization signal is reduced in irradiated populations, and hyperbaric-air controls used in earlier trials may themselves mobilize cells. Canada Hyperbarics will continue to track new mobilization-endpoint trials as they index in PubMed and add them to the research database.
This content is for informational purposes only and does not constitute medical advice. Treatment decisions should be made in consultation with a qualified physician familiar with the patient’s medical history. HBOT is regulated in Canada by Health Canada under the Medical Devices Regulations; clinical use should occur within recognised conditions or properly approved research protocols.