Reading time: about 8 minutes
TL;DR: Hyperbaric oxygen therapy (HBOT) is an emerging adjunct in burn care, not a first-line treatment. A 2026 systematic review of 13 studies (566 patients) found that several studies reported fewer surgeries and shorter hospital stays with HBOT, alongside trends toward improved healing, but heterogeneous designs prevented a meta-analysis. The clearest signal from the wider literature is that lower chamber pressures (below 3 ATA) are associated with better outcomes. Well-designed randomised controlled trials in burn centres remain the key research gap.
Hyperbaric oxygen therapy is a treatment in which a patient breathes 100% oxygen inside a pressurised chamber at pressures greater than one atmosphere absolute (ATA). In burn care, it is studied as an adjunct to standard wound management, with the aim of improving tissue oxygenation, reducing oedema, and supporting healing. The current evidence for hyperbaric oxygen therapy for burns is best described as promising but inconsistent: the most recent systematic review concluded that HBOT shows promise as a burn-care adjunct while cautioning that study designs and treatment protocols vary too widely for firm conclusions.
What does the current evidence say about hyperbaric oxygen therapy for burns?
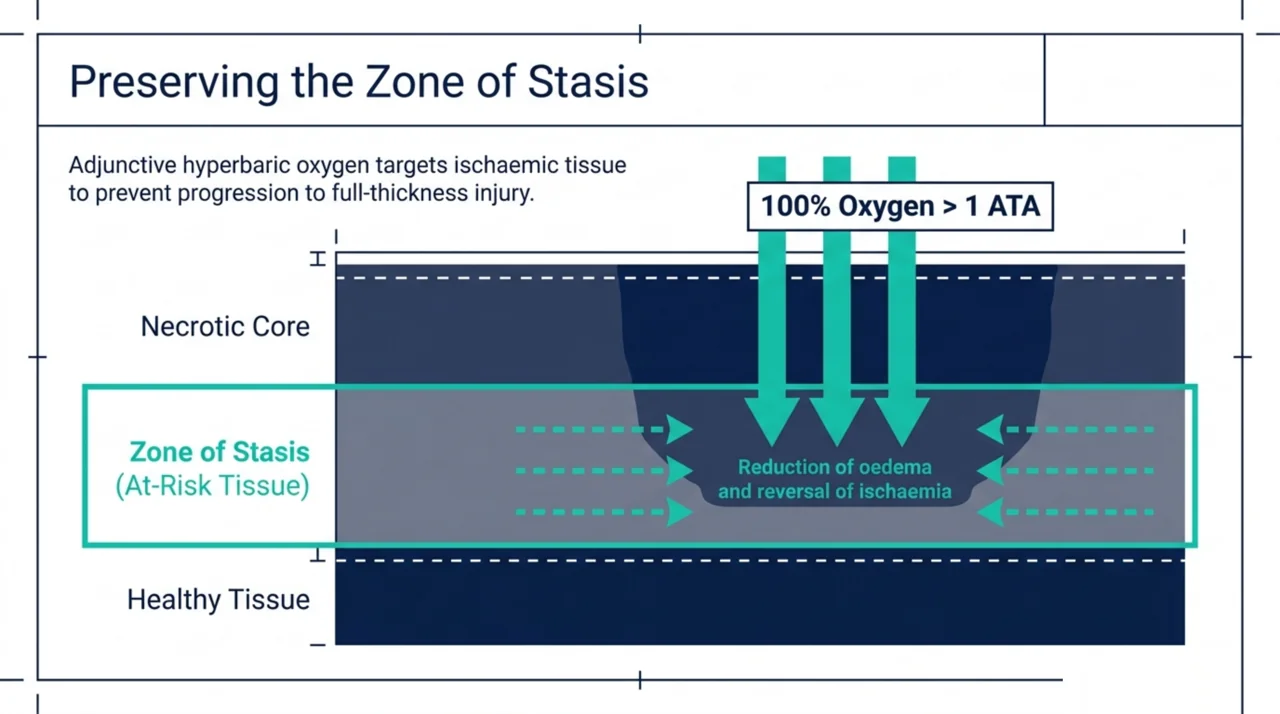
The short answer is that the signal is positive but the evidence base is thin and heterogeneous. Across more than five decades of experimental and clinical work, hyperbaric oxygen has been linked to reduced dermal ischaemia, less oedema, and better preservation of the burn “zone of stasis” – the at-risk tissue surrounding a burn that can either recover or progress to full-thickness injury. Yet these mechanistic rationales have not translated into a strong, consistent clinical evidence base. For researchers, the honest framing is that HBOT in burns is an active investigational question rather than a settled standard of care.
What did the 2026 systematic review of HBOT in burn care find?
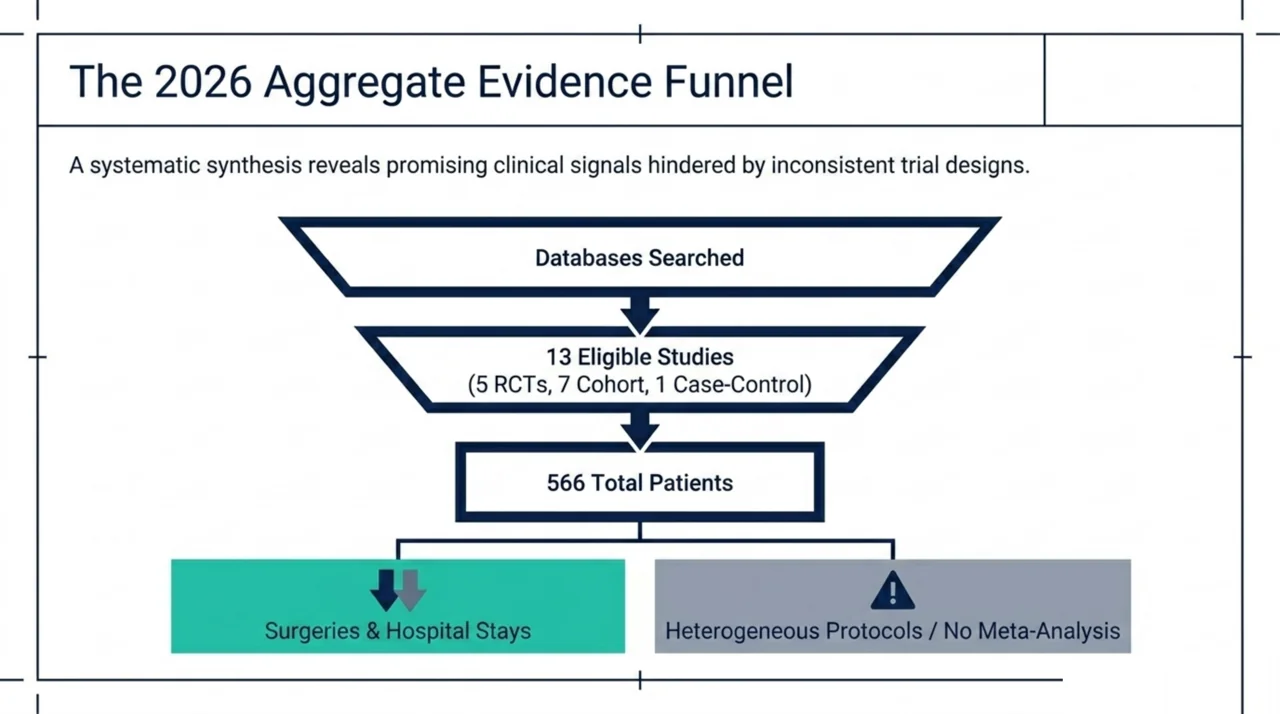
In a 2026 systematic review published in the Journal of Burn Care & Research, Molina-Vega and colleagues applied PRISMA methodology to the question (Molina-Vega et al., PubMed | Our Assessment). The reviewers searched PubMed, the Cochrane Library, and Embase in September 2025 and identified 13 eligible studies: 5 randomised controlled trials, 7 cohort studies, and 1 case-control study, together evaluating 566 burn patients. Several studies reported a reduced need for surgery and shorter hospital stays with HBOT, and the authors noted trends toward improved healing and lower infection risk. Mortality benefits, by contrast, were inconsistent. Because burn severity, HBOT protocols, and reported outcomes varied substantially, the reviewers judged the data too heterogeneous for a meta-analysis and concluded that HBOT shows promise as an adjunct in burn care rather than an established treatment.
Why does hyperbaric pressure dose matter in burn treatment?
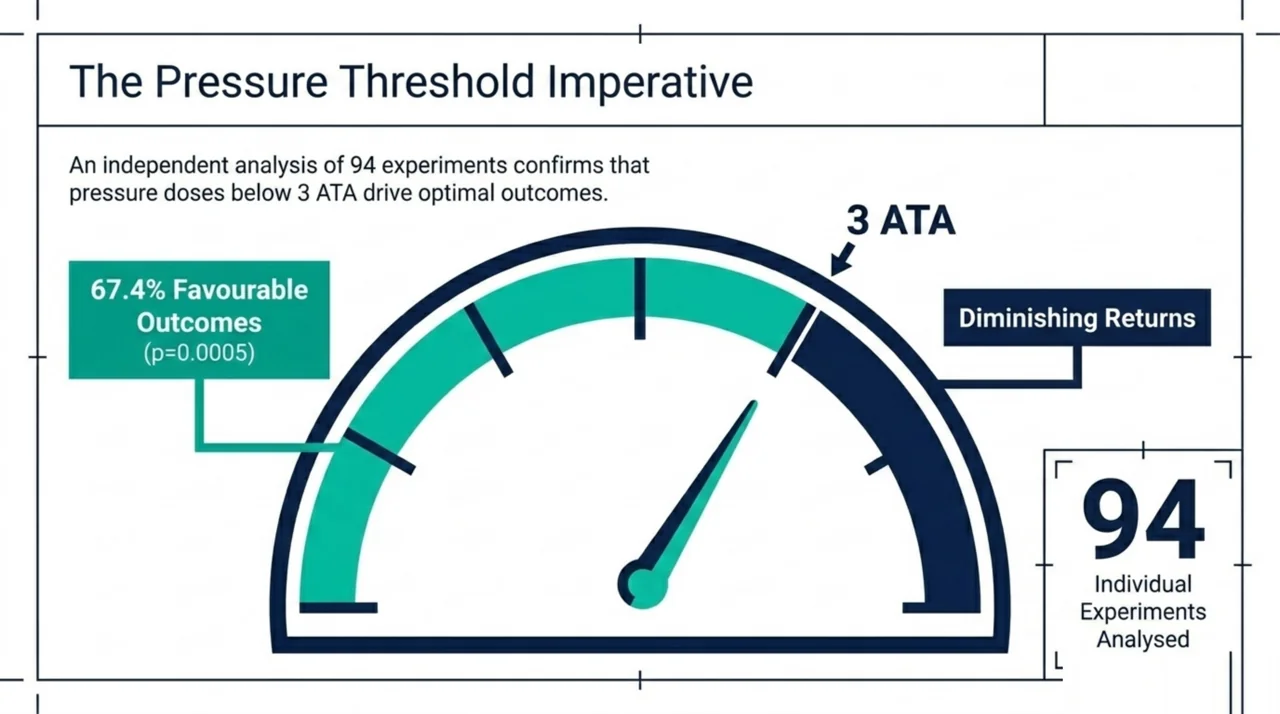
A 2024 review in Undersea and Hyperbaric Medicine looked specifically at why burn results have been so mixed (Smolle et al., PubMed | Our Assessment). Drawing on original work dating back to 1965, the authors assembled 47 publications – 32 animal trials, 4 trials in human volunteers, and 11 clinical studies – containing 94 individual experiments. Of these, 64 (67.4%) showed a positive outcome, 16 (17.9%) were ambiguous, and 14 (14.7%) were negative. The single factor that independently influenced results was pressure: sessions delivered below 3 ATA were significantly associated with better outcomes (p=0.0005). The authors stressed the need for well-designed clinical studies in burn centres equipped with hyperbaric facilities to establish dedicated treatment protocols. For trial designers, this is a concrete, testable hypothesis: pressure dose, not simply the decision to use HBOT, may be the variable that matters most.
What do clinical studies of HBOT in burn patients show?
Two recent clinical studies illustrate the kind of outcomes researchers are tracking. A 2023 prospective observational study of deep second-degree burns enrolled 38 patients and compared conventional treatment alone with conventional treatment plus HBOT, performed by a single experienced surgeon to minimise confounding (Ozdemir et al., PubMed | Our Assessment). Mean burned total body surface area was about 9% (range 5% to 20%). Patients who received HBOT had a lower need for surgery and grafting (p=0.003 and p=0.03), and their wounds epithelialised in a shorter time (p<0.001). Because this was an observational design rather than a randomised trial, the results point to an association rather than proof of cause.
A 2025 case series from the Vietnam National Institute of Maritime Medicine followed 82 thermal burn patients treated with hyperbaric oxygen between 2018 and 2022 (Pham et al., PubMed | Our Assessment). Most injuries were caused by boiling water (74.4%), and 80.5% of patients had burns covering less than 10% of total body surface area. In this uncontrolled series, the mean length of stay was 8.9 days, which the authors reported as significantly lower than expected. As a single-arm series with no comparison group, it adds descriptive support rather than confirmatory evidence.
Can HBOT help burns complicated by drug-resistant infection?
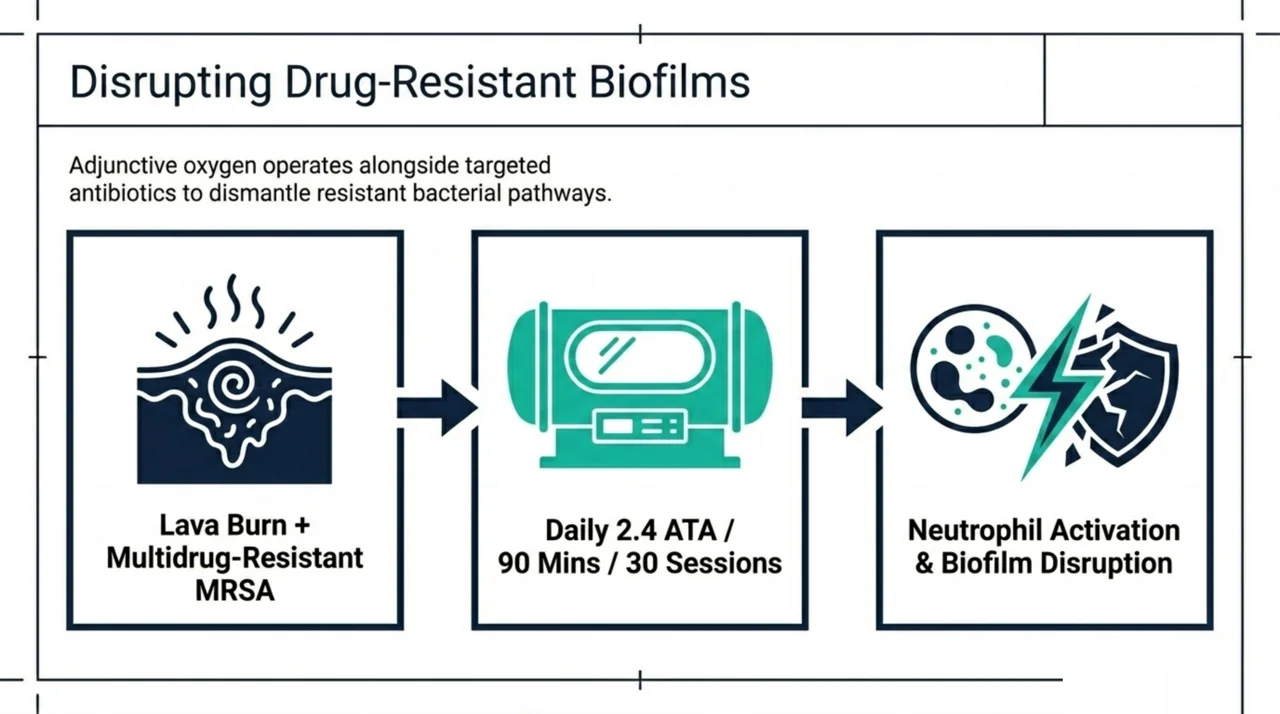
Burn wounds are highly vulnerable to infection, and one 2026 case report explored HBOT in exactly that setting (Oley et al., PubMed | Our Assessment). A 43-year-old man with lava-related burns over 15% of his body developed persistent multidrug-resistant infection, including MRSA. Alongside targeted antibiotics and repeated debridement, he received HBOT at 2.4 ATA for 90 minutes daily over 30 sessions, beginning on day 17. The authors describe progressive clearance of the resistant organisms and propose that HBOT contributed through increased tissue oxygenation, granulation, neutrophil activation, and disruption of bacterial biofilms. As a single case, it cannot establish efficacy, but it points to an infection-control mechanism that warrants formal testing.
How do the key burn studies compare?
| Study (Year) | Design | Patients | Key reported outcome |
|---|---|---|---|
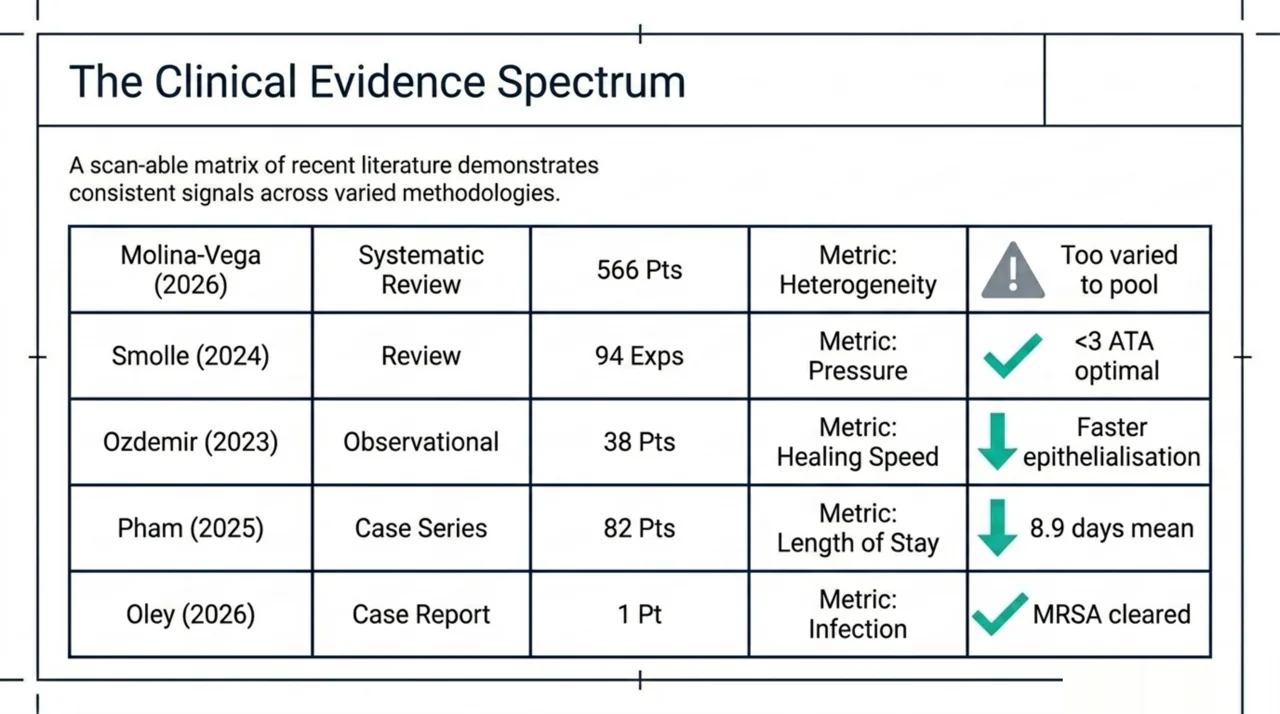
| Molina-Vega et al. (2026) | Systematic review (13 studies) | 566 | Fewer surgeries and shorter stays in several studies; too heterogeneous to pool |
| Smolle et al. (2024) | Review (47 publications, mostly animal) | 94 experiments | Pressure below 3 ATA associated with better outcomes (p=0.0005) |
| Ozdemir et al. (2023) | Prospective observational | 38 | Lower need for surgery and grafting; faster epithelialisation (p<0.001) |
| Pham et al. (2025) | Case series | 82 | Mean length of stay 8.9 days, lower than expected |
| Oley et al. (2026) | Case report | 1 | Clearance of MRSA and resistant organisms with adjunctive HBOT |
What are the research gaps and what should future studies measure?
For researchers, the consistent message across these papers is methodological. The 2026 systematic review could not pool its data because protocols and outcome measures were too varied, and the 2024 review found that pressure dose, rather than the decision to use HBOT alone, was the variable that independently predicted results. Future trials would benefit from standardised pressure and session protocols, clear stratification by burn depth and total body surface area, and a shared set of core outcomes such as time to healing, surgeries avoided, infection rates, length of stay, and scar quality. Burn centres with on-site hyperbaric capacity are the natural setting for the randomised controlled trials the field still lacks, and these are summarised alongside hundreds of other indications in the Canada Hyperbarics research library.
How does this apply in the Canadian context?
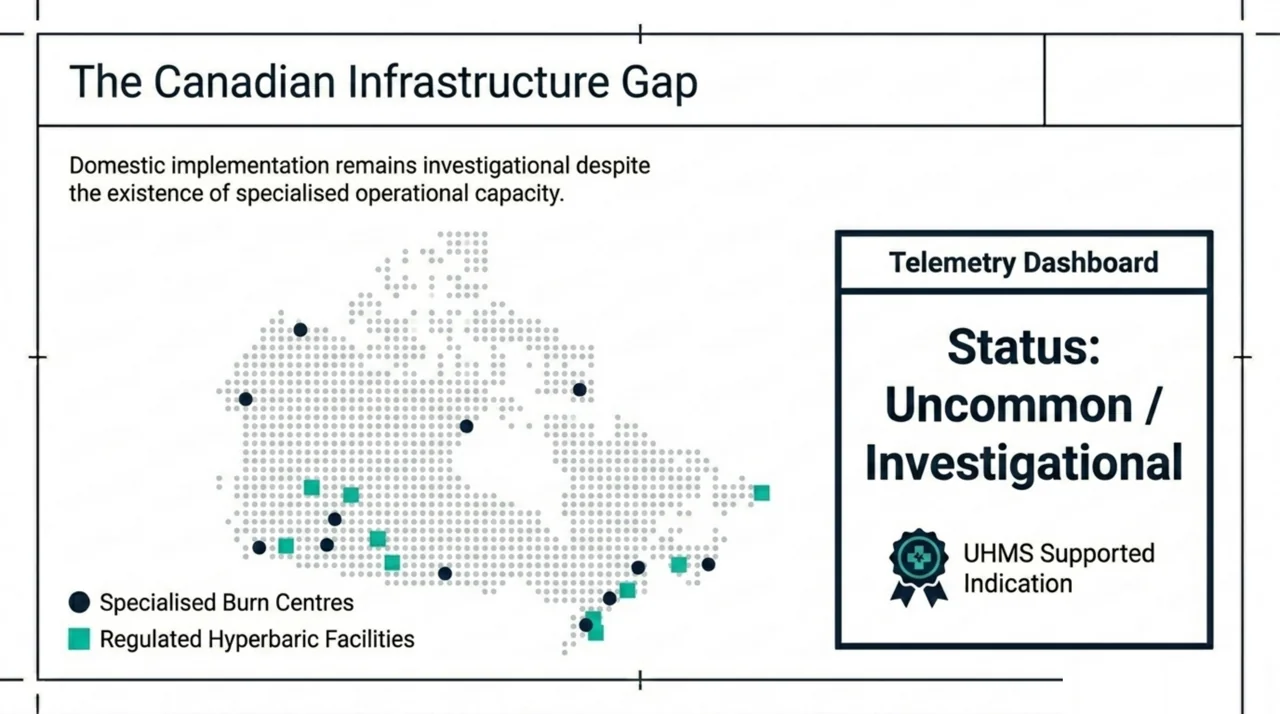
In Canada, severe burns are managed at specialised burn centres, and hyperbaric oxygen therapy is delivered at a limited number of hospitals and regulated facilities, most of which focus on wound care, diving injuries, and other established indications. Thermal burns are recognised among the conditions supported by the Undersea and Hyperbaric Medical Society (UHMS clinical practice guidelines), but Canadian use of HBOT as a burn adjunct remains uncommon and largely investigational. Canada Hyperbarics maintains an independent overview of the evidence and of where hyperbaric capacity actually exists, including a dedicated summary of the evidence for acute thermal burns.
Frequently asked questions about HBOT for burns
Is hyperbaric oxygen therapy an approved treatment for burns?
Thermal burns are listed among the indications supported by the Undersea and Hyperbaric Medical Society, where HBOT is used as an adjunct to standard burn care rather than a stand-alone treatment. In practice, its use in burns is far less common than for established indications such as carbon monoxide poisoning or non-healing wounds, and the supporting evidence is still developing.
Does HBOT improve healing in burn patients?
The 2026 systematic review found that several studies reported fewer surgeries and shorter hospital stays with HBOT, along with trends toward improved healing. However, study designs and protocols varied so widely that the reviewers could not combine the results statistically, so these findings should be read as promising rather than definitive.
What pressure is used for hyperbaric oxygen therapy in burns?
Most clinical burn protocols use pressures in the range of roughly 2.0 to 2.5 ATA. Notably, a 2024 review found that experiments using pressures below 3 ATA were significantly associated with better outcomes, which has made pressure dose a focus for future research.
Can HBOT reduce infections in burn wounds?
Laboratory rationale and individual case reports suggest HBOT may help by raising tissue oxygen levels, supporting white-blood-cell activity, and disrupting bacterial biofilms. A 2026 case report described clearance of drug-resistant organisms in a burn patient receiving HBOT, but single cases cannot prove that HBOT prevents or clears infection on its own.
How strong is the overall evidence for HBOT in burn care?
The evidence is best described as low-to-moderate certainty. The largest synthesis to date pooled only 566 patients across 13 small and varied studies, with just 5 randomised controlled trials among them. The field needs larger, standardised trials before HBOT can be considered an evidence-based standard for burns.
Is hyperbaric oxygen therapy for burns available in Canada?
Hyperbaric oxygen therapy is available at a limited number of hospitals and regulated facilities across Canada, though most programmes prioritise established indications over burns. You can review where capacity exists using the Canada Hyperbarics directory of hospitals and regulated facilities, and explore related questions in our frequently asked questions.
The bottom line for researchers
Hyperbaric oxygen therapy for burns sits at an interesting research frontier. The mechanistic case is plausible, early clinical signals point toward fewer surgeries and shorter stays, and the pressure-dose finding gives trial designers a clear hypothesis to test. What is missing is the high-quality, standardised, adequately powered randomised evidence that would move HBOT from “promising adjunct” to “evidence-based component” of burn care. Until those trials are done, claims should stay carefully calibrated to the observational and small-trial data that currently exist.
This content is for informational purposes only and does not constitute medical advice. Hyperbaric oxygen therapy for burns is an adjunctive and largely investigational use, and treatment decisions should be made by qualified burn and hyperbaric specialists. To see where hyperbaric oxygen therapy is offered across the country, explore the Canada Hyperbarics directory of hospitals and regulated facilities.