
TL;DR: Diabetic foot ulcers are the single most-studied wound indication for hyperbaric oxygen therapy (HBOT), yet the evidence remains genuinely contested. A 2026 network meta-analysis of 27 randomised controlled trials found gas-based therapies, including HBOT, were associated with more than double the rate of complete wound healing versus standard care (risk ratio 2.17), but high statistical heterogeneity and a paradoxical ranking that placed standard care first mean the certainty of that evidence is low. For researchers, the open questions are no longer “does oxygen help wounds heal” but “which patients, at which pressures, measured how.” This Canada Hyperbarics review maps the 2026 literature and the gaps worth funding.
A diabetic foot ulcer is a full-thickness wound below the ankle in a person with diabetes mellitus, arising from the combined effects of peripheral neuropathy, impaired tissue perfusion, and disordered wound healing. It is one of the most consequential complications of diabetes, and it is also the indication that has driven more hyperbaric oxygen therapy research than any other wound type. For the research community, that makes the diabetic foot ulcer both a proving ground and a cautionary tale: decades of trials have produced a large but heterogeneous body of evidence, and the field is still arguing about effect size, patient selection, and outcome definitions.
This review summarises what the 2026 literature, indexed in the Canada Hyperbarics research database, tells us about HBOT for diabetic foot ulcers, where the evidence is strongest, where it is weakest, and which methodological questions deserve the next generation of Canadian studies. Throughout, claim strength is matched to study design: pooled randomised data are described differently from single-arm pilots and narrative reviews.
Why are diabetic foot ulcers so hard to heal?
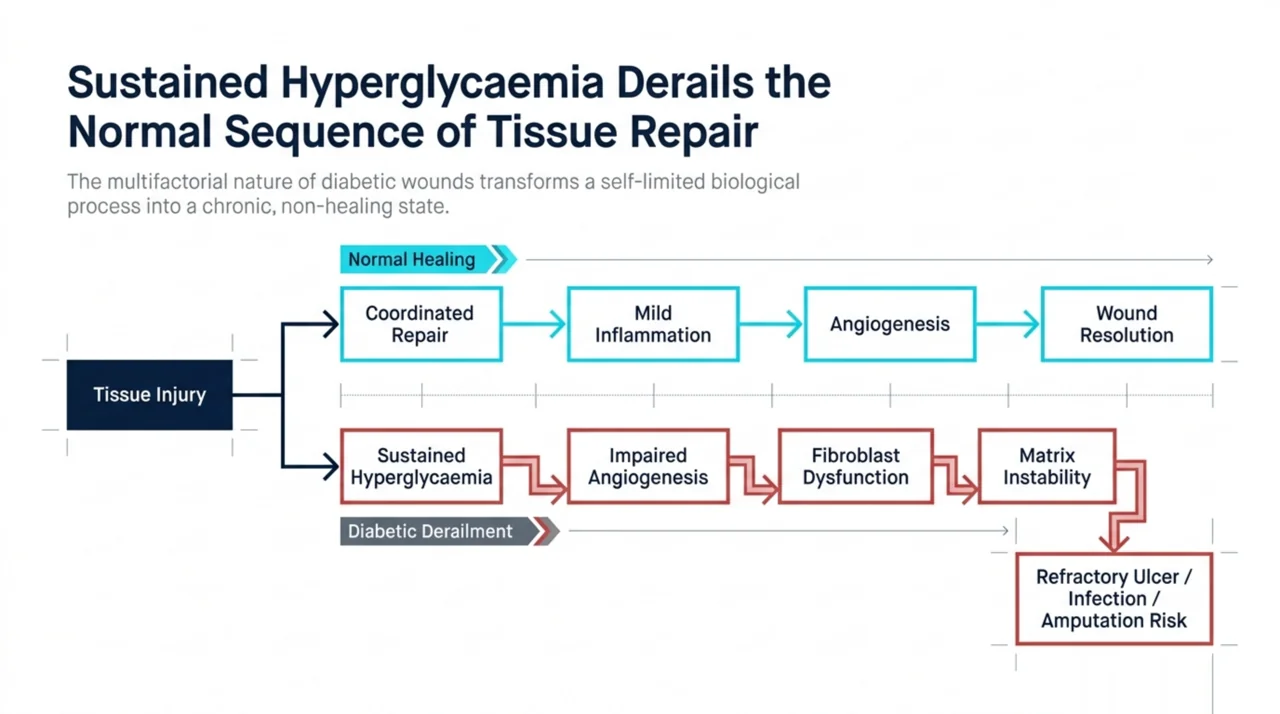
The biological rationale for oxygen-based therapy starts with how diabetes derails the normal repair sequence. A 2026 mechanistic review in the International Wound Journal (Jreije et al., PubMed | Our Assessment) describes how sustained hyperglycaemia transforms a coordinated, self-limited repair process into a chronic, non-healing state. The authors catalogue persistent inflammation, impaired angiogenesis, fibroblast dysfunction, and extracellular matrix instability as the core derailments, and they link these to the downstream burden clinicians recognise: refractory ulcers, infection, hospitalisation, amputation, and premature death.
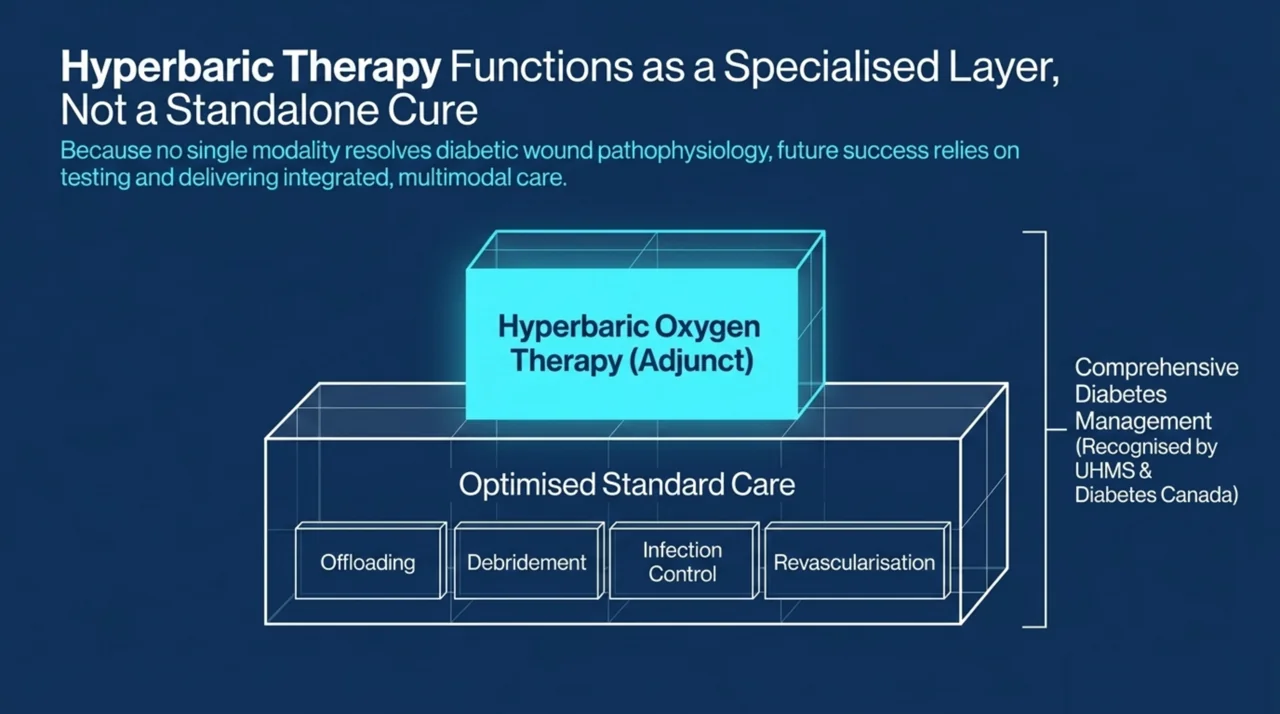
That same review reaches a conclusion researchers should sit with: no single modality fully addresses the multifactorial nature of diabetic wounds. Hyperbaric oxygen therapy is examined alongside negative-pressure wound therapy, advanced dressings, biologic grafts, and regenerative strategies, and the authors frame the most promising path forward as multimodal rather than any one intervention winning outright. This matters for trial design, because studies that test HBOT as a stand-alone therapy may be asking the wrong question.
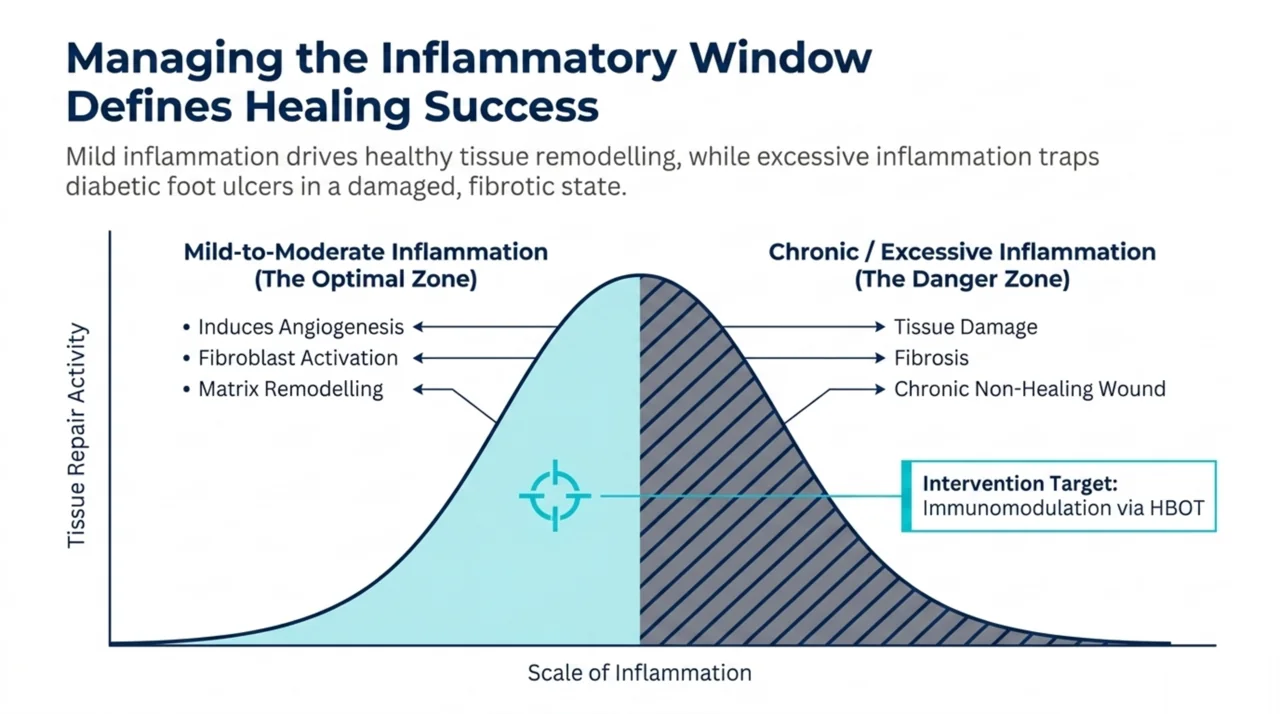
A complementary 2026 overview of inflammation and wound healing in Biomarker Research (Zhang et al., PubMed | Our Assessment) sharpens the inflammation story. The authors describe how mild-to-moderate inflammation induces angiogenesis, fibroblast activation, and matrix remodelling, whereas chronic or excessive inflammation drives tissue damage, fibrosis, and the chronic non-healing wound. The review lists hyperbaric oxygen among the novel interventions examined against this inflammatory backdrop, which is one reason the inflammation pathway is frequently cited as a mechanistic rationale for oxygen-based wound therapies.
What is the mechanistic basis for hyperbaric oxygen in wound repair?
Hyperbaric oxygen therapy is the inhalation of 100% oxygen at pressures above one atmosphere absolute, which sharply raises the amount of oxygen dissolved in plasma and available to hypoxic tissue. The link between tissue oxygenation and wound healing is not a recent claim. A 2026 historical review in Undersea and Hyperbaric Medicine (Huang et al., PubMed | Our Assessment) traces the modern foundation to 1964, when Dr T.K. Hunt was asked by the United States National Science Foundation to investigate divers who reported that their wounds healed better while living in an underwater habitat than on dry land. Hunt’s subsequent work established the scientific rationale that wound healing depends on tissue oxygenation.
A 2026 structured narrative review in Cureus (Gonzalez Flores et al., PubMed | Our Assessment), covering literature from January 2000 to February 2026, lists the physiological mechanisms invoked for HBOT: enhanced plasma-dissolved oxygen delivery, stimulation of angiogenesis, fibroblast proliferation, collagen synthesis, and immunomodulation. The authors report that clinical evidence supports HBOT in chronic ischaemic wounds, explicitly including diabetic foot ulcers, with improved wound closure rates and reduced infection risk reported across the synthesised studies. As a narrative review rather than a pooled analysis, it describes the direction of the evidence rather than quantifying a single effect size.
How strong is the randomised evidence for HBOT in diabetic foot ulcers?
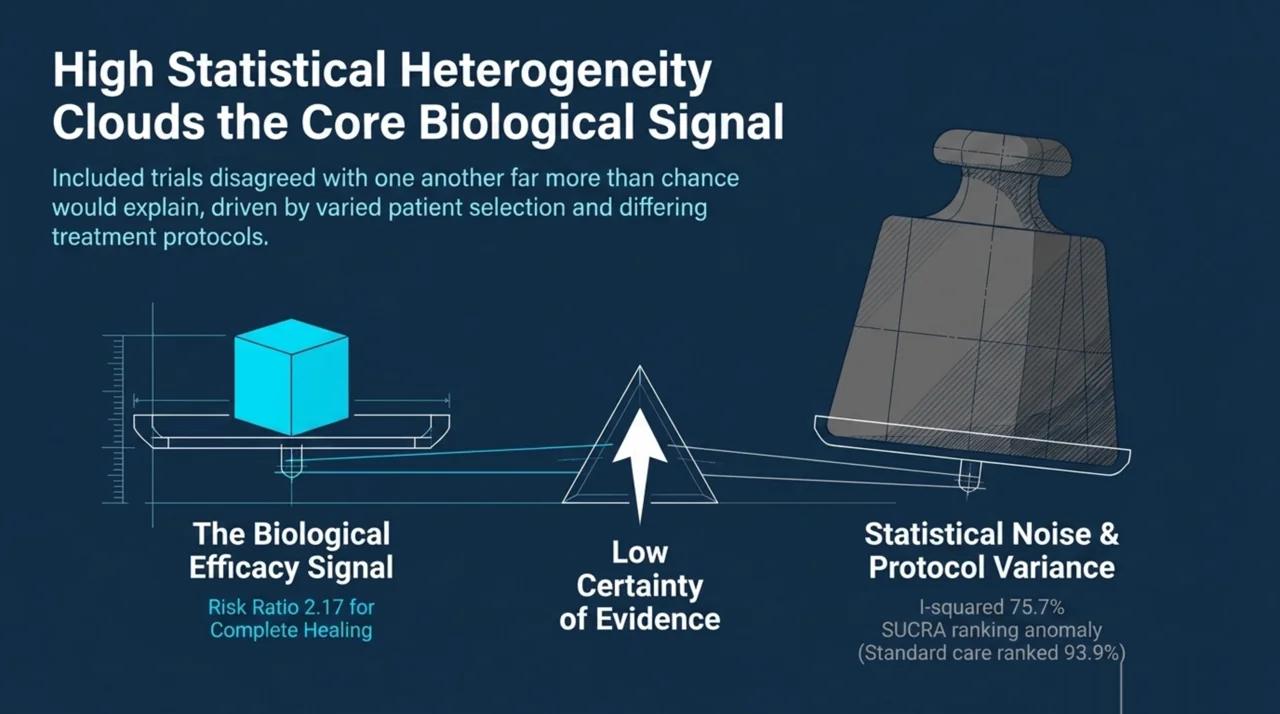
The most rigorous 2026 synthesis is a systematic review and network meta-analysis in the Journal of Clinical Medicine (Zheng et al., PubMed | Our Assessment), which compared gas-based therapies for chronic wounds. Following PRISMA 2020, the authors included 27 randomised controlled trials comprising 1,673 participants, with complete wound healing as the primary endpoint. In pairwise pooling, gas-based therapies significantly increased complete healing versus standard care, with a random-effects risk ratio of 2.17 (95% confidence interval 1.61 to 2.94). The analysis pooled gas therapies as a class rather than isolating hyperbaric oxygen, so the figure should be read as a class-level effect.
That headline figure deserves caution rather than celebration. The same analysis reported substantial statistical heterogeneity (I-squared of 75.7%), meaning the trials disagreed with one another more than chance would explain. More striking, when the authors ran the network meta-analysis and ranked treatments by SUCRA, standard care landed highest at 93.9%, a counterintuitive result the authors attributed to the structure of the evidence network and between-study differences rather than to standard care being genuinely superior. The practical reading for researchers is that the pooled signal favours oxygen-based therapy, but the certainty of that signal is undermined by heterogeneity and network instability. This is exactly the pattern that has kept diabetic foot ulcer HBOT in evidence limbo for two decades.
Single-centre work continues to add granular signal without resolving the larger debate. A 2026 pilot study in Folia Medica (Gyurova-Kancheva et al., PubMed | Our Assessment) positions hyperbaric oxygenation as an established complementary method within complex, individualised diabetic foot care, reflecting the wider clinical consensus that HBOT is an adjunct rather than a replacement for offloading, debridement, infection control, and revascularisation. As a pilot, its role is to generate hypotheses and refine protocols for larger trials, not to establish efficacy on its own.
How does the 2026 evidence compare across study designs?
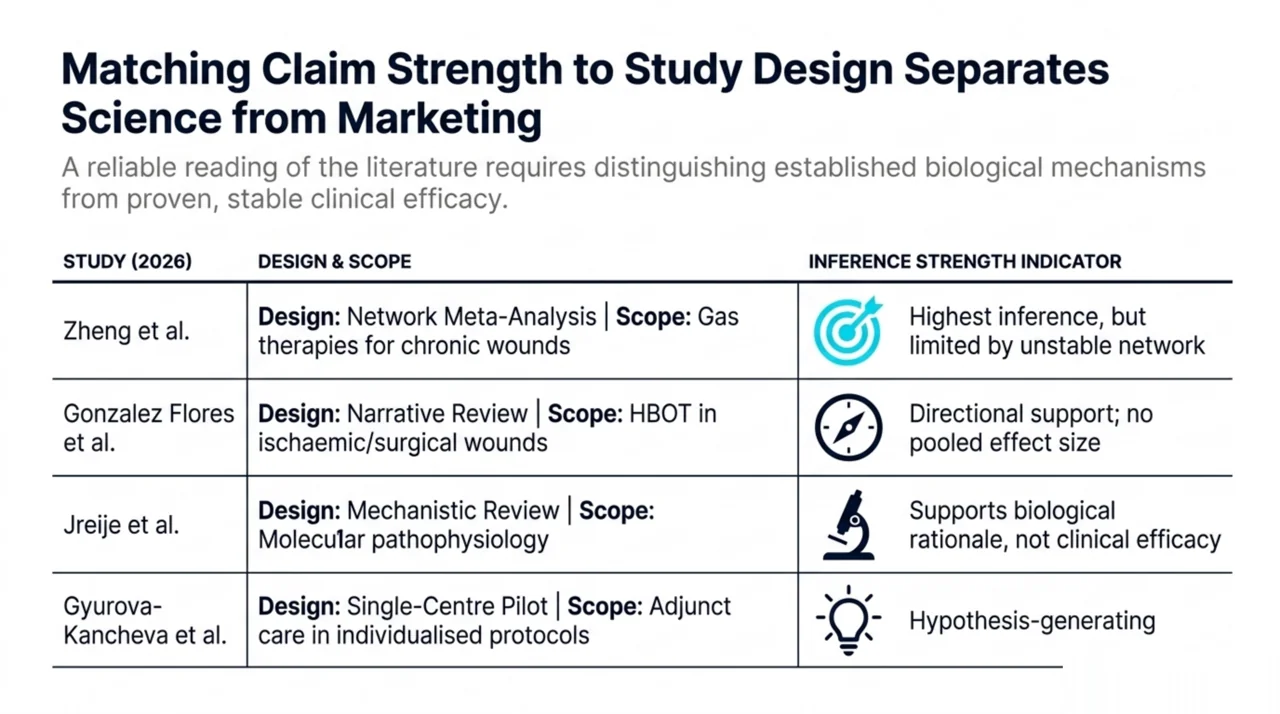
The table below summarises the four 2026 sources that bear most directly on diabetic and chronic wound healing, organised by design and by the strength of inference each supports. Reading the evidence this way, by design rather than by headline, is the discipline that separates a useful research synthesis from a marketing claim.
| Study (2026) | Design | Scope | Strength of inference |
|---|---|---|---|
| Zheng et al., J Clin Med | Systematic review + network meta-analysis (27 RCTs, 1,673 patients) | Gas therapies for chronic wounds, complete healing endpoint | Highest, but limited by heterogeneity (I-squared 75.7%) and unstable network ranking |
| Gonzalez Flores et al., Cureus | Structured narrative review (2000-2026) | HBOT in surgical and ischaemic wounds, including diabetic foot ulcers | Directional; describes supportive evidence without a pooled effect size |
| Jreije et al., Int Wound J | Mechanistic review | Molecular pathophysiology of diabetic wound healing | Mechanistic; supports rationale, not efficacy |
| Gyurova-Kancheva et al., Folia Med | Pilot study | HBOT as adjunct in diabetic foot ulcer care | Hypothesis-generating; not powered for efficacy |
What are the open research questions for Canadian investigators?
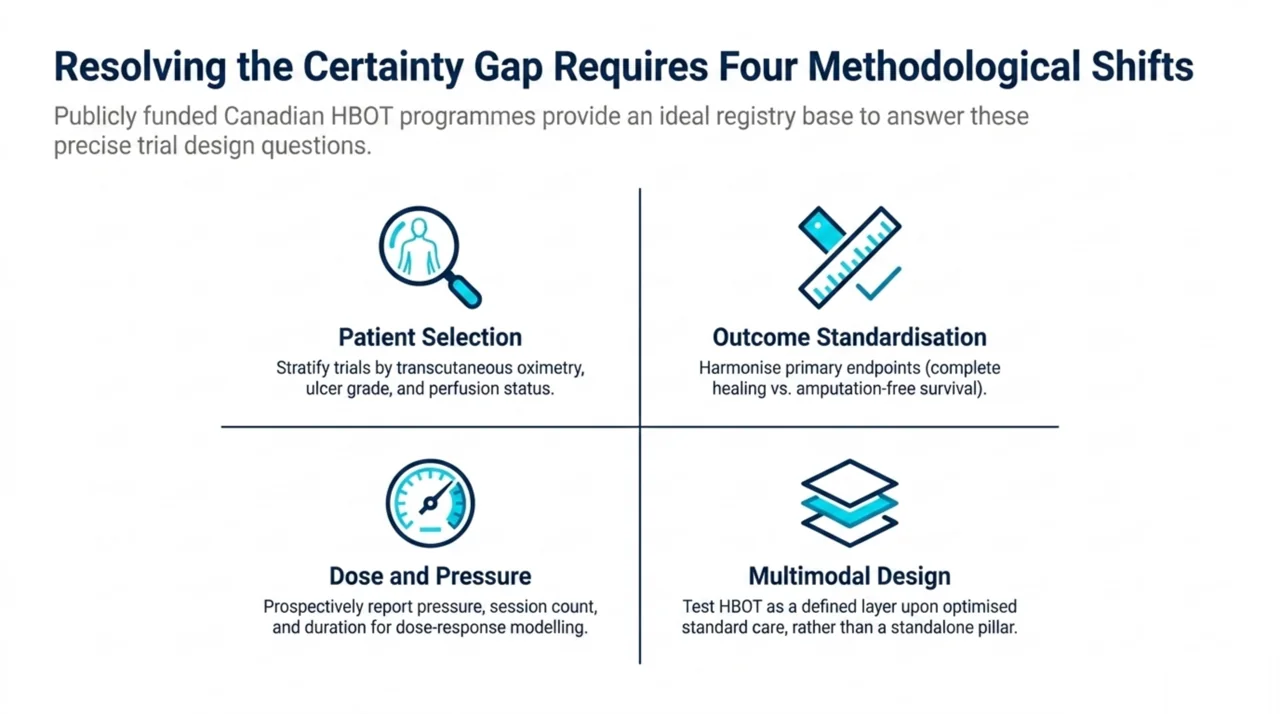
If the broad question of whether oxygenation aids wound repair is settled at the mechanistic level, the productive questions are now narrower and more answerable. Four stand out for Canadian research teams.
- Patient selection. The heterogeneity in pooled analyses strongly suggests effect modification by wound and patient characteristics. Trials that stratify by transcutaneous oximetry, ulcer grade, and perfusion status, rather than enrolling all diabetic foot ulcers together, would clarify who actually benefits.
- Outcome standardisation. Complete wound healing, amputation-free survival, and time-to-healing are not interchangeable endpoints. Harmonising primary outcomes across trials would make future meta-analyses far less heterogeneous.
- Dose and pressure. Protocol variation in pressure, session count, and treatment duration is rarely reported in a way that allows dose-response modelling. Canadian multicentre work could prospectively standardise and report these parameters.
- Multimodal design. Because no single modality resolves diabetic wound pathophysiology, factorial trials that test HBOT layered onto optimised standard care may be more informative than head-to-head comparisons against standard care alone.
Canada is well placed to contribute. Publicly funded HBOT programmes operate within several provincial hospital systems, and the directory of hospitals and regulated facilities offering hyperbaric medicine provides a realistic recruitment base for pragmatic trials. Coordinated registry data, captured consistently across sites, would help close the certainty gap that the 2026 network meta-analysis exposed.
Where do diabetic foot ulcers sit among approved HBOT indications?
Selected diabetic wounds are among the indications recognised by the Undersea and Hyperbaric Medical Society (UHMS), whose indication list is the reference standard most Canadian programmes follow. Diabetes Canada’s clinical practice guidelines situate foot care within comprehensive diabetes management, where adjuncts such as HBOT are considered after offloading, infection control, and vascular assessment. For the regulatory and coverage context that shapes access in each province, see the Canada Hyperbarics coverage guide and the broader conditions overview.
The distinction between an approved indication and proven efficacy is itself a research-relevant point. Recognition reflects a balance of mechanism, accumulated clinical experience, and the available trial base; it is not a claim that the evidence is free of uncertainty. Honest synthesis, of the kind this review aims to model, keeps those two ideas separate.
Frequently asked questions about HBOT for diabetic foot ulcers
Is hyperbaric oxygen therapy proven to heal diabetic foot ulcers?
The evidence is supportive but not conclusive. A 2026 network meta-analysis of 27 randomised trials found gas-based therapies, including HBOT, were associated with roughly double the rate of complete healing versus standard care, but substantial heterogeneity and an unstable treatment ranking lower the certainty of that finding. HBOT is best understood as an adjunct within comprehensive wound care rather than a stand-alone cure.
Why do meta-analyses disagree on HBOT for diabetic wounds?
Disagreement is driven mainly by heterogeneity: trials differ in patient selection, ulcer severity, oxygen pressure and session protocols, and outcome definitions. The 2026 Zheng network meta-analysis reported an I-squared of 75.7%, indicating the included trials varied far more than chance alone would predict, which weakens any single pooled estimate.
What is the biological mechanism behind HBOT for wound healing?
Breathing oxygen under pressure raises the amount dissolved in plasma, increasing delivery to hypoxic tissue. The 2026 evidence describes mechanisms including stimulation of angiogenesis, fibroblast proliferation, collagen synthesis, and immunomodulation. The principle that wound healing depends on tissue oxygenation dates to investigations by Dr T.K. Hunt beginning in 1964.
Is HBOT a replacement for standard diabetic foot care?
No. Across the 2026 literature, HBOT is consistently positioned as a complementary method layered onto offloading, debridement, infection control, and revascularisation. Mechanistic reviews emphasise that no single modality addresses the multifactorial nature of diabetic wounds, so multimodal care remains the standard.
What should the next diabetic foot ulcer trials measure?
Priorities include stratifying patients by perfusion and ulcer grade, standardising primary outcomes such as complete healing and amputation-free survival, reporting pressure and session dose in enough detail for dose-response analysis, and testing HBOT within multimodal rather than stand-alone designs. These steps would reduce the heterogeneity that currently limits evidence certainty.
Where can I read the underlying studies?
Each study cited here links to both its primary PubMed record and a Canada Hyperbarics assessment summarising its methods and findings. The full, filterable collection is available in the Canada Hyperbarics research database, which indexes the wound-healing literature alongside other hyperbaric indications.
The bottom line for researchers
Diabetic foot ulcers remain the best-studied and most instructive wound indication in hyperbaric medicine. The 2026 evidence reinforces a strong mechanistic rationale and a supportive but heterogeneous randomised signal, while exposing exactly where the field needs better-designed trials: patient selection, outcome standardisation, dose reporting, and multimodal design. For Canadian investigators, the combination of an established hospital-based delivery network and a clear methodological agenda makes this an unusually tractable area to advance. Canada Hyperbarics maintains an indexed, continually updated record of this literature to support that work.
To explore the facilities, conditions, and coverage context referenced throughout this review, visit the Canada Hyperbarics directory of hospitals and regulated facilities.
This content is for informational purposes only and does not constitute medical advice. It is intended to summarise published research for an academic and professional audience. Treatment decisions should be made by qualified healthcare professionals in the context of an individual patient’s circumstances.