
Reading time: about 8 minutes
TL;DR: Hyperbaric oxygen therapy (HBOT) is being studied as an add-on for cardiovascular disease, but it is not an approved cardiac treatment in Canada. The strongest 2025-2026 signal comes from a single-arm interim study of ischaemic cardiomyopathy, where a combined counterpulsation-plus-HBOT protocol was associated with a higher left ventricular ejection fraction and better functional capacity. Systematic-review and mechanistic work point in the same direction, yet almost all of it is small, uncontrolled, or preclinical. For now, cardiovascular HBOT is an investigational research area, not a Health Canada approved indication.
Hyperbaric oxygen therapy is a medical treatment in which a person breathes 100% oxygen inside a pressurised chamber, raising the amount of oxygen dissolved in the blood and delivered to tissue. In cardiovascular medicine, researchers are testing whether that oxygen boost can protect ischaemic myocardium, support angiogenesis, and calm the inflammation that drives heart failure. This review for researchers summarises what the newest studies in the Canada Hyperbarics research database actually report, and where the evidence remains thin.
An important caveat first: cardiovascular disease is not among the conditions Health Canada has licensed hyperbaric chambers to treat, nor is it on the Undersea and Hyperbaric Medical Society (UHMS) recognised indications list. Health Canada has issued device licences for hyperbaric chambers only for a defined set of conditions (see the federal Health Canada guidance on hyperbaric oxygen therapy and our conditions overview). Everything below sits outside that approved scope and should be read as emerging research.
What does the newest 2026 evidence on HBOT for ischaemic cardiomyopathy show?
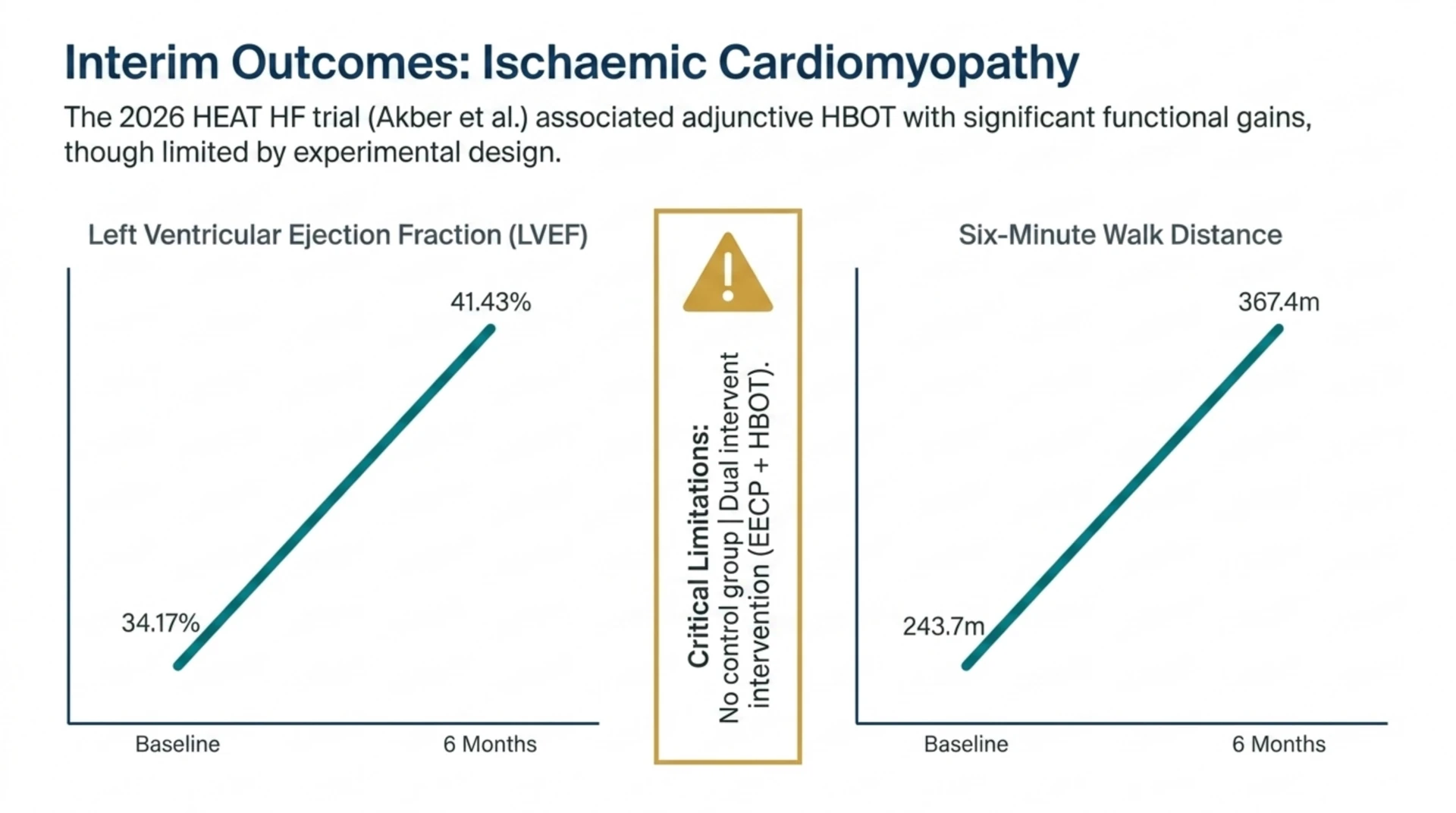
The most notable recent clinical entry is the HEAT HF interim analysis (Akber et al., 2026, PubMed | Our Assessment). This prospective interventional study enrolled 100 adults with ischaemic cardiomyopathy and a left ventricular ejection fraction (LVEF) of 50% or less, and treated them with enhanced external counterpulsation (EECP) plus adjunctive HBOT. The cohort was 88% male with a mean age of 61.5 years.
In this single-arm interim analysis at six months, the combined protocol was associated with improvement across every measured endpoint. LVEF rose from 34.17% to 41.43% (p<0.001), six-minute walk distance increased from 243.7 to 367.4 metres (p<0.001), and New York Heart Association (NYHA) class shifted from mostly III/IV to mainly I (p<0.001). Global longitudinal strain, NT-proBNP, and heart-failure hospitalisations also improved (p<0.001).
Two design features must temper any conclusion. First, the study had no control group, so regression to the mean and background guideline-directed medical therapy cannot be separated from the intervention. Second, HBOT was delivered alongside EECP, so the observed gains cannot be attributed to hyperbaric oxygen on its own. The authors themselves frame this as an interim look at an ongoing trial. It is a hypothesis-strengthening result, not proof of a cardiac HBOT effect.
How might hyperbaric oxygen affect the cardiovascular system?
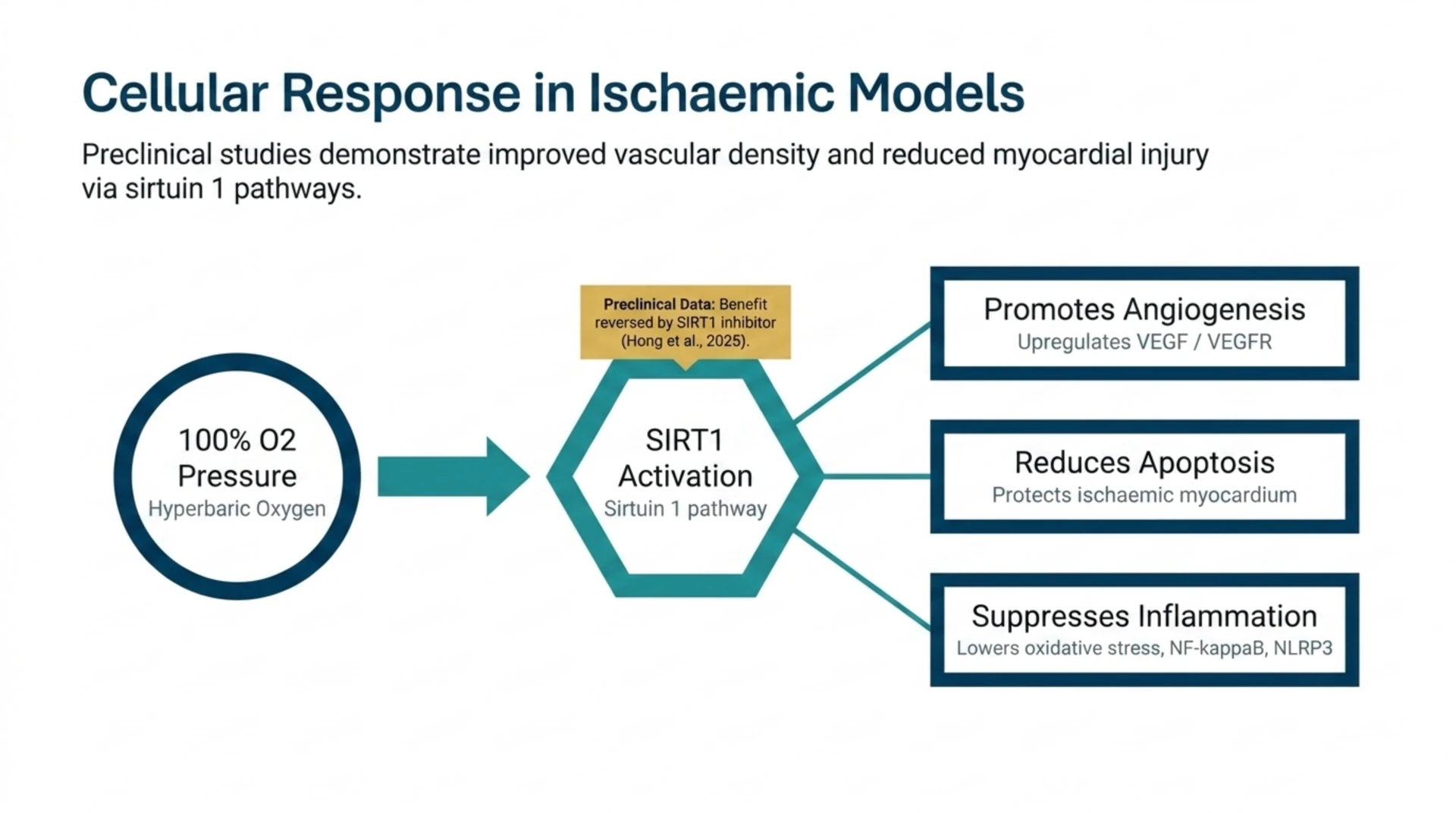
A 2025 review of HBOT in cardiovascular disease (Tian et al., 2025, PubMed | Our Assessment) describes the proposed mechanisms. The review reports that hyperbaric oxygen enhances oxygen delivery to ischaemic and reperfused tissue, promotes angiogenesis, and suppresses oxidative stress, inflammatory cascades, and cardiomyocyte apoptosis. It notes that when combined with reperfusion, HBOT has been reported to improve LVEF in acute myocardial infarction, and that in heart failure it may support myocardial repair.
Most of the mechanistic detail still comes from the laboratory. A 2025 animal study (Hong et al., 2025, PubMed | Our Assessment) used a limb-ischaemia model in high-fat-diet mice and found that hyperbaric oxygen improved blood flow and vascular density while reducing apoptosis. The effect tracked with sirtuin 1 (SIRT1) activation: the benefit was reversed by a SIRT1 inhibitor, and hyperbaric oxygen upregulated angiogenesis proteins (VEGF, VEGFR) while downregulating apoptosis markers. These are preclinical vascular findings, so they inform biology rather than clinical practice, but they help explain why the cardiovascular hypothesis persists.
What does the systematic-review evidence say about HBOT and myocardial injury?
A 2026 systematic review with qualitative synthesis (Almomany et al., 2026, PubMed | Our Assessment) searched the literature through May 2025 and identified five clinical studies covering 431 patients. In acute myocardial infarction, HBOT was associated with reduced creatine phosphokinase (up to a 35% reduction, p=0.03) and improved LVEF (p<0.05) in the randomised studies included.
The reviewers were explicit about the limits. They could not perform a meta-analysis because of substantial heterogeneity and incomplete reporting, and they concluded that the clinical effect of HBOT on myocardial injury and inflammatory biomarkers remains unclear. In other words, the direction of the signal is encouraging, but the quantity and consistency of evidence are not yet sufficient to guide cardiac practice.
Can HBOT reduce complications after cardiac surgery?
Perioperative use is a distinct research thread. A 2025 review of HBOT in cardiovascular surgery (Wang et al., 2025, PubMed | Our Assessment) summarises the rationale for hyperbaric oxygen as a preconditioning strategy before procedures such as coronary artery bypass grafting, valve replacement, and cardiac intervention. The review reports that hyperbaric oxygen has been used to lower the morbidity of postoperative complications, including hypoxic encephalopathy, air embolism, cognitive dysfunction, and major adverse cardiovascular events.
Inflammatory heart disease is being explored too. A 2026 preclinical review of experimental autoimmune myocarditis (Pindovic et al., 2026, PubMed | Our Assessment) reports that in animal models hyperbaric oxygen suppressed NF-kappaB and NLRP3 inflammasome activation, lowered oxidative stress, and boosted regulatory T-cell responses. The authors stress the translational gaps: inconsistent protocols, no long-term outcome data, and uncertainty about the best treatment length and patient selection.
How strong is the cardiovascular HBOT evidence overall?
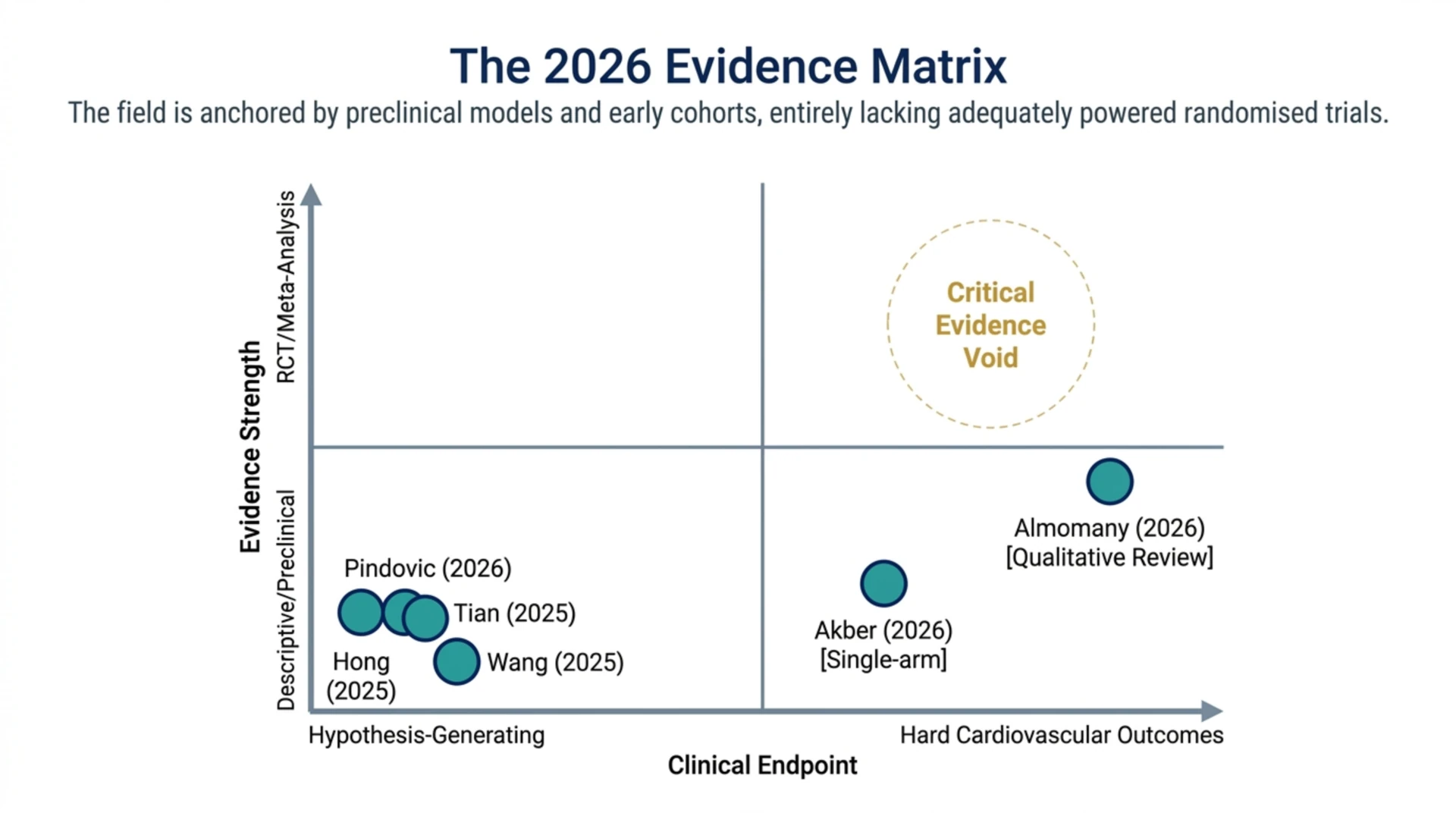
The table below maps the studies covered here by design and evidence strength. It is a useful reminder that the field is anchored by reviews and one uncontrolled clinical cohort, not by large randomised trials.
| Study (year) | Design | Focus | Reported signal | Evidence strength |
|---|---|---|---|---|
| Akber et al. (2026) | Prospective, single-arm interim | Ischaemic cardiomyopathy (EECP + HBOT) | LVEF and 6-minute walk improved | Low (no control, combined therapy) |
| Almomany et al. (2026) | Systematic review (qualitative) | Myocardial injury and inflammatory biomarkers | Reduced CPK, improved LVEF in acute MI | Low to moderate (heterogeneous, no meta-analysis) |
| Tian et al. (2025) | Narrative review | Cardiovascular disease mechanisms and outcomes | Angiogenesis, anti-inflammatory effects | Descriptive (hypothesis-generating) |
| Wang et al. (2025) | Narrative review | Cardiovascular surgery preconditioning | Fewer postoperative complications | Descriptive |
| Hong et al. (2025) | Animal and in vitro | Limb ischaemia, SIRT1 pathway | Improved perfusion, less apoptosis | Preclinical |
| Pindovic et al. (2026) | Preclinical review | Autoimmune myocarditis | Reduced inflammation in models | Preclinical |
The pattern is consistent: a plausible mechanism, encouraging early signals, and a near-total absence of adequately powered randomised controlled trials with hard cardiovascular endpoints. That combination is exactly where a research programme, not a treatment recommendation, belongs. Researchers can browse the underlying studies in the Canada Hyperbarics research database and filter by condition and evidence type.
Frequently asked questions
Is hyperbaric oxygen therapy an approved treatment for heart disease in Canada?
No. Health Canada has licensed hyperbaric chambers only for a defined set of recognised conditions, and cardiovascular disease is not among them. Any cardiac use is investigational and should occur within a research study or a clinical trial, not as routine care.
Does HBOT improve ejection fraction in heart failure?
The 2026 HEAT HF interim analysis reported that LVEF rose from 34.17% to 41.43% in patients treated with combined counterpulsation and HBOT. Because the study had no control arm and used two therapies together, this cannot be read as proof that hyperbaric oxygen alone improves ejection fraction.
Is the cardiovascular evidence based on randomised controlled trials?
Mostly not. The current base is dominated by narrative reviews, one uncontrolled clinical cohort, a small systematic review that could not pool its data, and preclinical models. A handful of randomised studies exist for acute myocardial infarction, but the overall quantity and quality remain limited.
Could HBOT help after a heart attack?
Some randomised studies summarised in the 2026 systematic review found that HBOT was associated with reduced creatine phosphokinase and improved LVEF in acute myocardial infarction. This is an active research question, not established practice, and any use would be experimental.
Are there cardiovascular risks to hyperbaric oxygen therapy?
Hyperbaric oxygen is generally well tolerated, but it is not risk-free in medically complex patients. A 2025 retrospective cohort in thoracic-trauma patients (Canarslan Demir et al., 2025, PubMed | Our Assessment) reported that 20% of patients developed respiratory or cardiac symptoms during treatment, underscoring the need for careful screening.
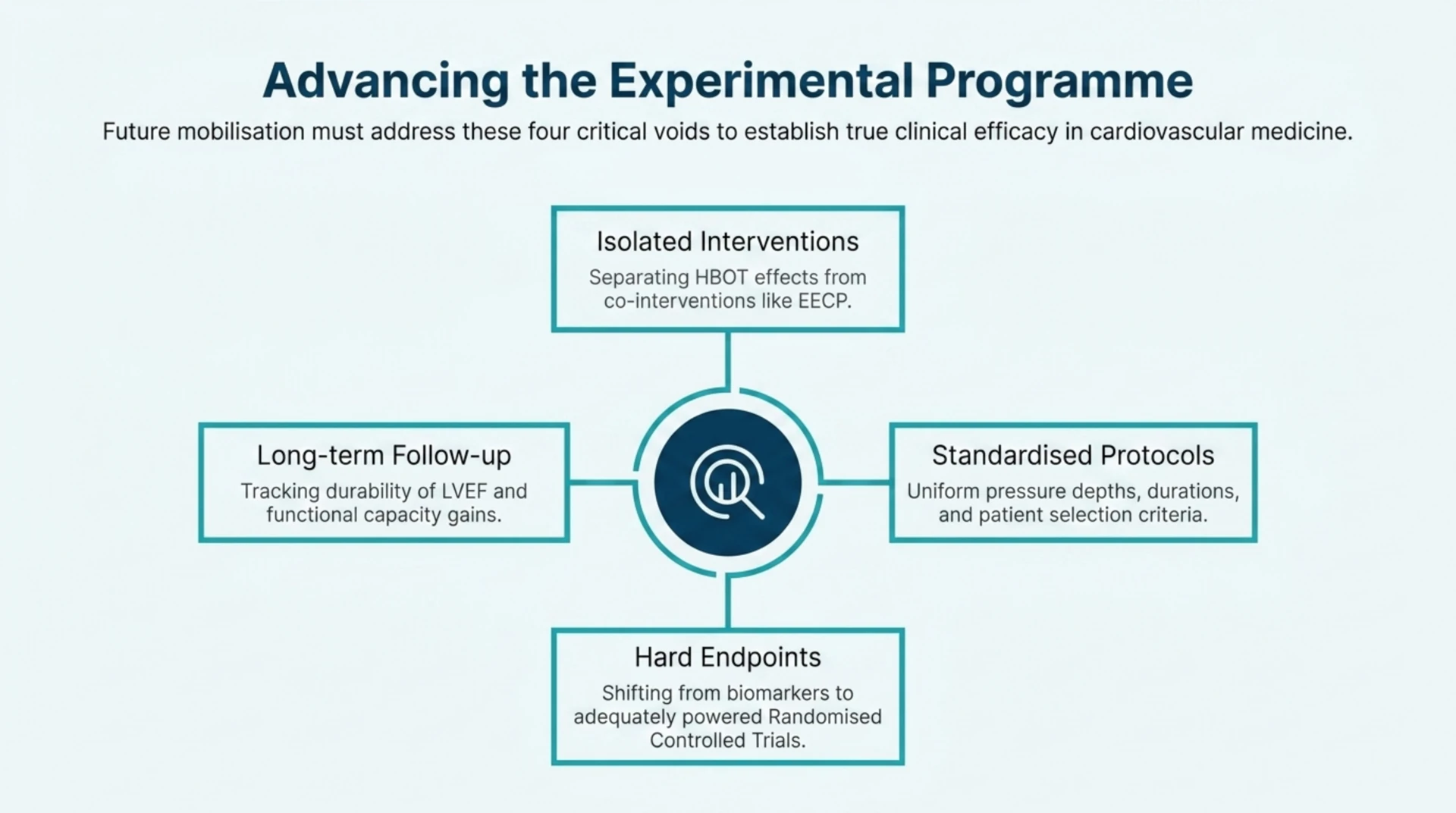
What should future cardiovascular HBOT research prioritise?
The reviews converge on the same needs: standardised treatment protocols, adequately powered randomised controlled trials with hard endpoints, longer follow-up, and clearer patient-selection criteria. Studies that isolate hyperbaric oxygen from co-interventions would be especially valuable.
Where can I find qualified facilities and the source studies?
Canada Hyperbarics maintains a directory of Canadian hospitals and regulated facilities that deliver hyperbaric oxygen therapy for its approved indications. The cardiovascular applications described in this review are investigational and fall outside that approved scope, so they are not offered as standard care. To review the primary literature yourself, start with the research database, and to see where accredited care is delivered in Canada, visit our directory of hospitals and regulated facilities.
Medical disclaimer: This content is for informational purposes only and does not constitute medical advice. It summarises research for a professional and research audience and does not recommend hyperbaric oxygen therapy for any cardiovascular condition. Always consult a qualified healthcare provider about diagnosis and treatment.