
TL;DR: Hyperbaric oxygen therapy (HBOT) is being studied for migraine and cluster headache, two of the most disabling primary headache disorders. The strongest controlled evidence points to a possible acute, attack-aborting effect for some patients, while evidence for a preventive (prophylactic) effect is weak or absent. Importantly, the established oxygen treatment for cluster headache is high-flow normobaric oxygen at sea-level pressure, not hyperbaric oxygen. Headache is not a Health Canada approved indication or a UHMS-recognised indication, so HBOT for headache remains investigational in Canada.
Migraine and cluster headache are common, severe, and costly to manage, and the search for non-pharmacological options has kept oxygen-based therapies under study for decades. Hyperbaric oxygen therapy is the breathing of 100% oxygen inside a pressurised chamber at greater than one atmosphere of pressure, which raises the amount of oxygen dissolved in blood and tissue. This evidence review for researchers summarises what controlled trials, systematic reviews, and mechanistic studies report about HBOT for migraine and cluster headache, where the signal is strongest, and where the research gaps remain. Canada Hyperbarics maintains a research library of these primary sources so that clinicians and investigators can read the underlying studies directly.
What is the difference between hyperbaric and normobaric oxygen for headache?
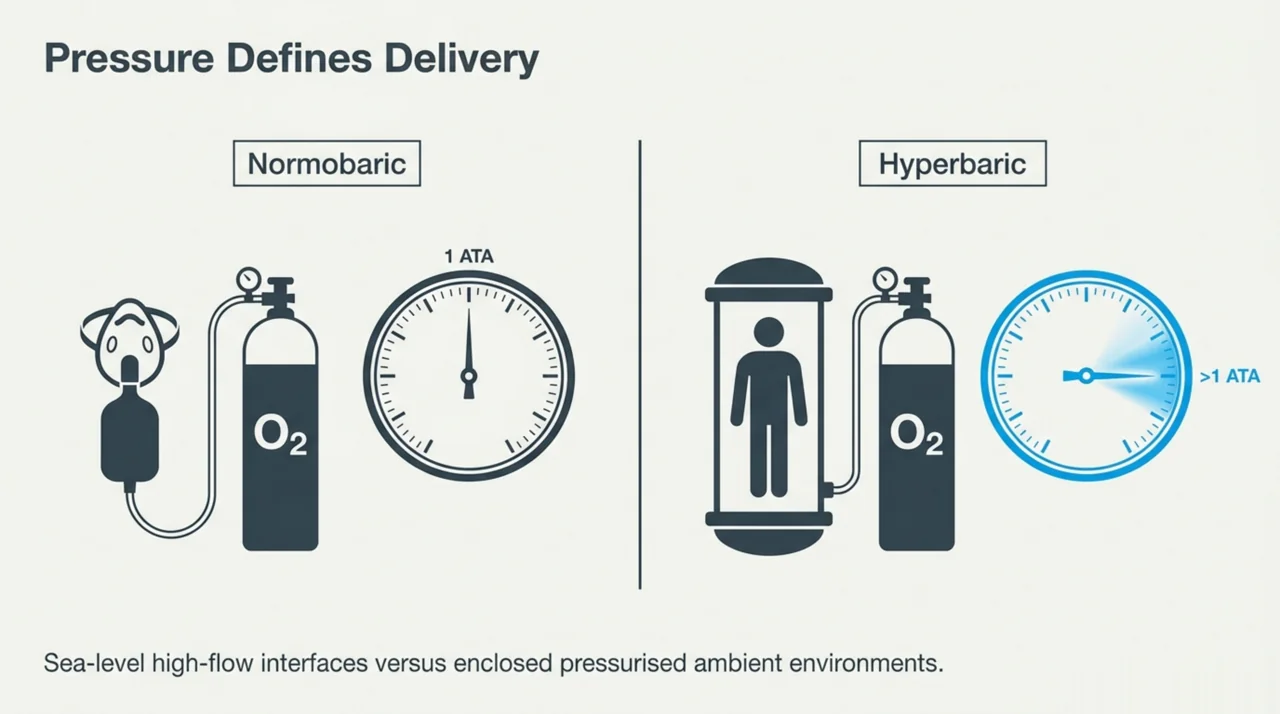
This distinction is the single most important framing point in the headache-oxygen literature, and conflating the two has muddied the field. Normobaric oxygen therapy (NBOT) is 100% oxygen delivered at one atmosphere (sea-level pressure), usually through a high-flow non-rebreather mask. Hyperbaric oxygen therapy (HBOT) delivers 100% oxygen at increased ambient pressure inside a chamber. High-flow normobaric oxygen was first described as an acute treatment for cluster headache by Horton in 1952 and is now a widely recommended and effective abortive therapy, with its mechanism linked to the trigeminovascular system and neuroinflammation, according to a 2019 review (Guo et al., PubMed | Our Assessment).
A 2016 review of oxygen delivery systems for cluster headache attacks examined the standard non-rebreather mask alongside partial rebreathers, demand valves, tusk masks, nasal cannulas, and hyperbaric and cooled oxygen, and found that interfaces such as demand valves and tusk masks may be superior or at least similar to the standard non-rebreather mask (Oude Nijhuis et al., PubMed | Our Assessment). For researchers, the practical implication is that any HBOT signal must be weighed against an inexpensive, low-risk normobaric comparator that is already standard care for cluster headache.
What does the Cochrane evidence say about HBOT for migraine and cluster headache?
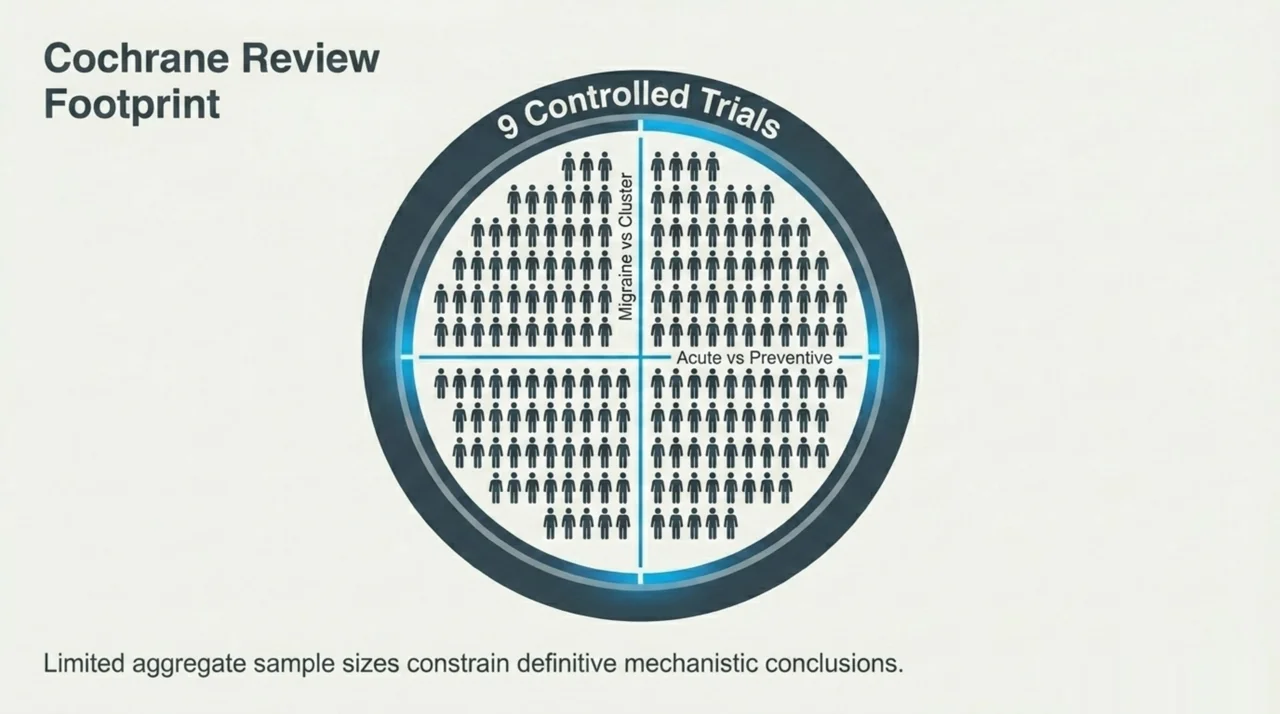
The keystone synthesis is the Cochrane systematic review of normobaric and hyperbaric oxygen for migraine and cluster headache. The 2008 review identified nine small randomised trials involving 201 participants and concluded that there was some evidence that HBOT was effective for the termination of acute migraine, while there was no evidence of any prophylactic (preventive) effect (Bennett et al., PubMed | Our Assessment).
This review was later updated as a 2015 version that re-examined the efficacy and safety of NBOT and HBOT in randomised controlled trials for the treatment and prevention of migraine and cluster headache (Bennett et al., PubMed | Our Assessment).
An independent Cochrane-based analysis reached the same conclusions: across nine trials with 201 participants, HBOT was effective in relieving acute migraine and appeared sufficient to treat an acute cluster attack, normobaric oxygen terminated acute cluster headache compared with sham but not compared with sublingual ergotamine, and there was no evidence for any prophylactic effect, with no serious adverse effects reported (Schnabel et al., PubMed | Our Assessment). The recurring methodological theme is small sample sizes and few high-quality trials, which limits the strength of any conclusion.
How strong is the acute (attack-aborting) evidence for HBOT?
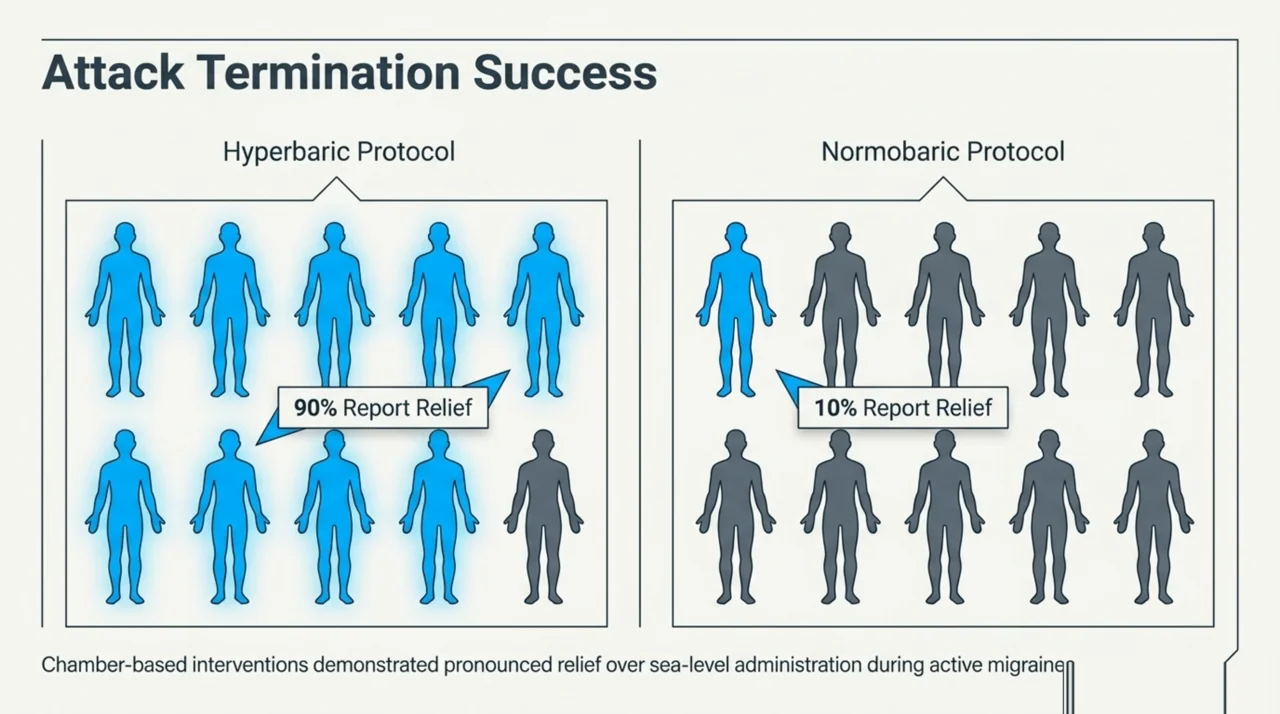
For acute migraine, the most-cited controlled comparison randomised 20 migraine patients during an attack to 100% oxygen at one atmosphere (normobaric) or at two atmospheres (hyperbaric). Nine of 10 patients in the hyperbaric group reported relief, compared with one of 10 in the normobaric group (Myers et al., PubMed | Our Assessment). The authors framed this as a preliminary report, and the small sample limits generalisability.
For acute cluster headache, an early controlled study treated seven patients with episodic cluster headache, of whom six experienced an interruption of the attack, while a placebo procedure in six different patients had no effect; the authors also reported a period without subsequent attacks in some responders (Di Sabato et al., PubMed | Our Assessment). A 2014 review of oxygen treatment for cluster headache reported that HBOT has been investigated in only a few small studies and that evidence exists for an acute, but not a prophylactic, effect, while normobaric low-flow oxygen produced positive responses in 56% to 82% of patients and high-flow oxygen in 78% of attacks (Petersen et al., PubMed | Our Assessment).
Does hyperbaric oxygen prevent migraine or cluster headache attacks?
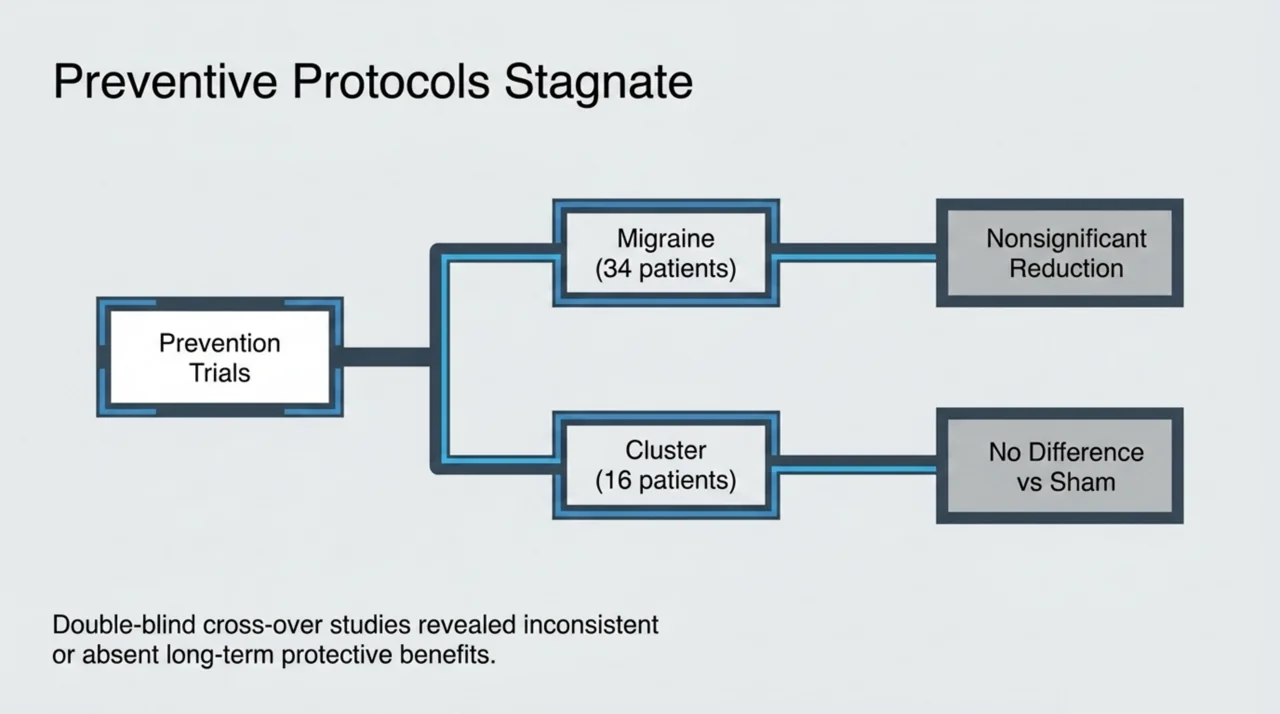
The preventive evidence is weaker and includes notable negative trials. A randomised, double-blind, placebo-controlled study assigned 40 migraine patients to three sessions of hyperbaric oxygen or three hyperbaric air (control) treatments; 34 completed the study, and the result was a nonsignificant reduction in hours of headache in the oxygen group, leading the authors to conclude that the tested protocol did not show a significant prophylactic effect on migraine (Eftedal et al., PubMed | Our Assessment).
For cluster headache prophylaxis, a double-blind, placebo-controlled cross-over study enrolled 16 patients (12 episodic, four chronic) who received 100% oxygen or a hyperbaric normoxic sham gas for 70 minutes at 2.5 ATA in two sessions; the study found no difference between hyperbaric oxygen and sham treatment on the headache index (Nilsson Remahl et al., PubMed | Our Assessment). A separate small case series of four patients with chronic cluster headache unresponsive to drugs reported that two improved markedly during a two-week course, one improved in frequency only, and one showed no benefit, prompting the authors to suggest hyperbaric oxygen as a transient preventive option for refractory sufferers (Pascual et al., PubMed | Our Assessment). Taken together, these results show inconsistent and mostly negative preventive findings.
How does the evidence compare across headache type and treatment goal?
| Treatment and goal | Migraine | Cluster headache |
|---|---|---|
| Normobaric high-flow oxygen, acute attack | Limited evidence; not standard care | Established, effective, and safe first-line abortive therapy |
| Hyperbaric oxygen, acute attack | Some evidence of benefit in small trials | Limited evidence of benefit in a few small studies |
| Hyperbaric oxygen, prevention | No significant effect in a randomised trial | No difference versus sham in a randomised cross-over trial |
| Serious adverse effects in trials | None reported | None reported |
This pattern is consistent with a broader review of hyperbaric oxygen in chronic pain management, which examined fibromyalgia, complex regional pain syndrome, myofascial pain, migraine, and cluster headache and concluded that HBOT may be beneficial when appropriate patients are selected, while cautioning about oxygen toxicity and the scarcity of treatment centres (Yildiz et al., PubMed | Our Assessment). Readers can explore related neurological evidence through the Canada Hyperbarics research library and the conditions index.
What mechanisms have been proposed for an oxygen effect in headache?
Mechanistic work has focused mainly on cluster headache. One controlled study of 14 patients with chronic cluster headache (10 treated with hyperbaric oxygen, four with environmental air) over 15 sessions investigated the influence of treatment on serotonergic pathways by measuring serotonin binding to mononuclear cells (Di Sabato et al., PubMed | Our Assessment).
A separate study evaluated the effect of hyperbaric oxygen on substance P immunoreactivity in the nasal mucosa of cluster headache patients compared with a placebo group, linking the therapy to primary nociceptive neurons and neuropeptide signalling (Di Sabato et al., PubMed | Our Assessment).
An experimental study using the glyceryl trinitrate headache model in 18 healthy subjects found no effect of pure oxygen inhalation on nitrate-induced headache in a double-blind crossover design, which tempers simple vasoconstriction explanations (Daugaard et al., PubMed | Our Assessment). The proposed pathways therefore remain associational and incompletely characterised.
Where does Canadian research fit, and what are the gaps?
Canadian-linked work has helped frame the research agenda. The 2008 Toronto Hyperbaric Medicine Symposium convened to design multicentre trials of hyperbaric oxygen for neurological indications, including stroke, traumatic brain injury, radiation encephalopathy, and status migrainosus, with proposed protocols published to guide future studies (Helms et al., PubMed | Our Assessment). More recently, a 2019 case report of a 23-year-old woman with an 11-year history of migraine with aura described 40 sessions at 1.5 ATA over roughly eight weeks, while noting that neither the United States nor the European consensus list of hyperbaric indications includes migraine (Matera et al., PubMed | Our Assessment).
Headache is not among the 14 conditions for which Health Canada has licensed hyperbaric chambers (see the Health Canada hyperbaric oxygen therapy page), nor is it among the 15 UHMS-recognised indications (see the UHMS Indications list). HBOT for headache is therefore investigational in Canada. The clearest research gaps are the absence of adequately powered randomised trials, the need to separate an acute effect from a preventive one, and the requirement to test HBOT against the inexpensive normobaric oxygen comparator that is already standard care for cluster headache. Canada Hyperbarics tracks new publications in this area as they are indexed.
Frequently asked questions
Is hyperbaric oxygen therapy approved for migraine or cluster headache in Canada?
No. Headache is not among the 14 conditions for which Health Canada has licensed hyperbaric chambers, and it is not a UHMS-recognised indication. Any use of HBOT for headache is investigational and should be framed within research or specialist care.
Is the oxygen used for cluster headache the same as HBOT?
No. The established oxygen treatment for an acute cluster headache attack is high-flow normobaric oxygen delivered at sea-level pressure through a non-rebreather mask. Hyperbaric oxygen therapy delivers oxygen at increased pressure inside a chamber and is a separate, investigational approach for headache.
Does the evidence support HBOT for aborting an acute migraine?
There is some evidence from small randomised trials and a Cochrane review that HBOT may help terminate an acute migraine in some patients, but the trials are small and the finding is not strong enough to establish HBOT as a standard treatment.
Can HBOT prevent future headache attacks?
The preventive evidence is weak. A randomised trial in migraine found no significant prophylactic effect, and a randomised cross-over trial in cluster headache found no difference between hyperbaric oxygen and sham treatment on the headache index.
Were there safety problems in the headache trials?
The published trials summarised by Cochrane reported no serious adverse effects. As with any hyperbaric treatment, oxygen toxicity and barotrauma are recognised risks that must be managed in an appropriate clinical setting.
What is the most important research gap?
The field lacks adequately powered randomised trials that separate an acute effect from a preventive one and that compare HBOT against the inexpensive normobaric oxygen already used for cluster headache. Until such trials exist, HBOT for headache remains investigational.
Conclusion and where to read the primary studies
The evidence for hyperbaric oxygen therapy in migraine and cluster headache is best summarised as a plausible but unproven acute effect with little support for prevention, drawn from small trials and reinforced by Cochrane synthesis. For cluster headache in particular, the practical and well-supported oxygen option is normobaric high-flow oxygen, not HBOT. Researchers can review the underlying studies and our structured assessments through the Canada Hyperbarics research library, browse related neurological topics in the conditions index, and find Canadian treatment settings in our directory of hospitals and regulated facilities. Common questions are also answered on our FAQ page.
This content is for informational purposes only and does not constitute medical advice. Hyperbaric oxygen therapy for migraine and cluster headache is investigational and is not an approved indication in Canada. Always consult a qualified healthcare professional about diagnosis and treatment decisions.