
TL;DR: Hyperbaric oxygen therapy (HBOT) is a treatment in which a person breathes 100% oxygen in a pressurised chamber, and it has been promoted for cerebral palsy for more than two decades, but the strength of the evidence depends almost entirely on study design. In the highest-quality sham-controlled randomised trials, HBOT produced no benefit over pressurised air, while both groups improved similarly – a pattern best explained by a participation effect. Open-label studies and a 2022 meta-analysis of mostly active-control trials report apparent gains, and a 2024 reanalysis argues the controversy is not settled. Cerebral palsy is not a Health Canada or UHMS-recognised indication, and the main documented harm is middle ear barotrauma. This 2026 Canada Hyperbarics evidence review traces the literature from 2002 to 2025 for researchers.
Reading time: about 9 minutes.
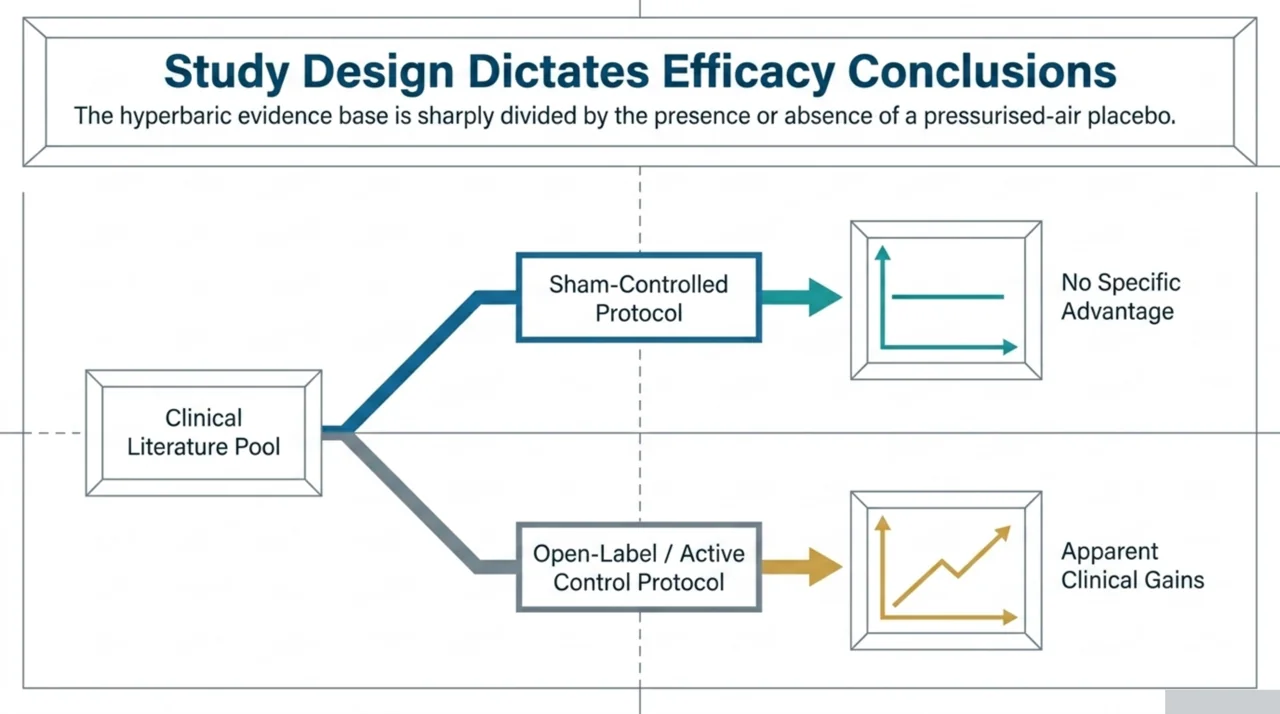
Hyperbaric oxygen therapy for cerebral palsy is one of the most studied and most contested applications of HBOT in paediatric neurology. The short answer for researchers is that the evidence is sharply divided along methodological lines: blinded, sham-controlled trials have not shown that breathing pressurised oxygen helps more than breathing pressurised air, yet uncontrolled and active-control studies keep reporting improvement. Understanding why these two literatures disagree is the central research question, and it is the focus of this review.
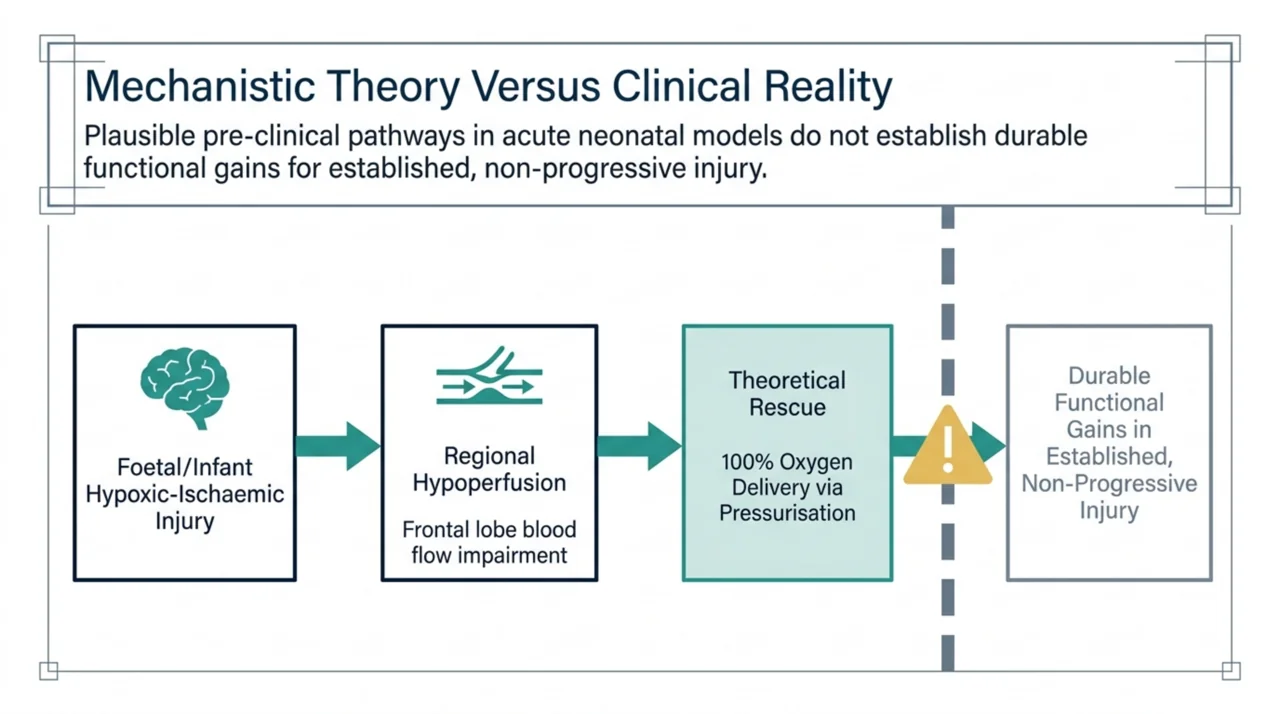
Cerebral palsy is a group of permanent disorders of movement and posture caused by non-progressive injury to the developing foetal or infant brain. It is the leading cause of physical disability in children. Because some of that brain injury involves hypoxia-ischaemia and impaired regional perfusion, hyperbaric oxygen has long been proposed as a way to deliver more oxygen to marginally viable tissue. Whether that mechanistic rationale translates into measurable clinical benefit is exactly what the trials below were designed to test.
Why was hyperbaric oxygen therapy proposed for cerebral palsy in the first place?
The biological argument rests on perfusion and oxygen delivery. Brain perfusion imaging studies have documented regional hypoperfusion in children and adults with cerebral palsy. In a small single-photon emission computed tomography (SPECT) study of 11 patients, all participants showed perfusion impairments, most often in the frontal lobe, and 2 of the 4 patients who went on to receive hyperbaric oxygen showed some degree of perfusion improvement afterward (Asl and colleagues, 2015; PubMed | Our Assessment). The sample is far too small to support efficacy claims, but it illustrates the perfusion-based reasoning that motivated clinical interest.
Pre-clinical work added to the rationale. In a neonatal rat model of hypoxia-ischaemia, the injury that can produce cerebral palsy, hyperbaric oxygen delivered one hour after the insult was associated with markedly less hemispheric atrophy and apoptosis and with improved sensorimotor function at five weeks (Calvert and colleagues, 2002; PubMed | Our Assessment). Animal neuroprotection in acute injury, however, is a very different question from durable functional gains in children with established, non-progressive injury years later. Mechanistic reviews of HBOT in neurological conditions make the same point: plausible molecular pathways exist, but they do not by themselves establish clinical efficacy (Fischer and colleagues, 2020; PubMed | Our Assessment).
What do the sham-controlled trials of HBOT for cerebral palsy actually show?
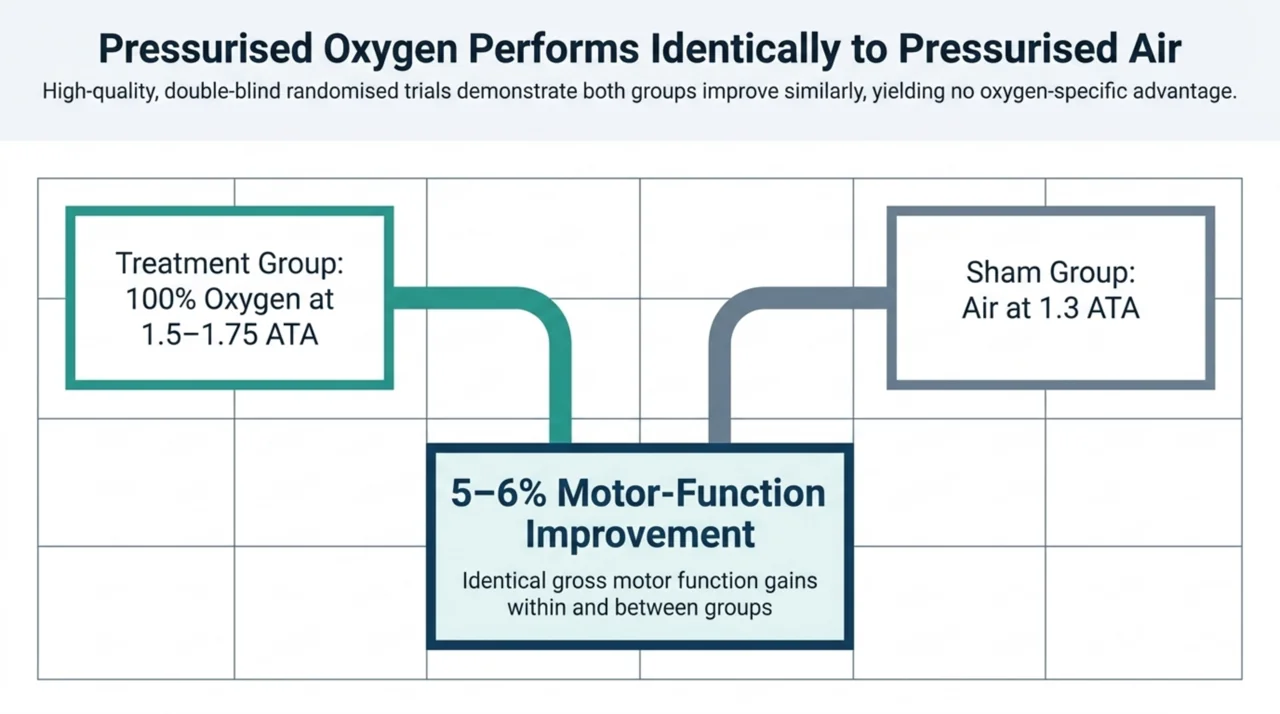
This is where the evidence is strongest and most consistent. When children are randomised to pressurised oxygen versus a sham of pressurised air, the two groups improve to a similar degree, and HBOT shows no specific advantage. In a randomised, double-blind trial of 49 children aged 3 to 8 years with spastic cerebral palsy, participants received 40 sessions of either 100% oxygen at 1.5 atmospheres or hyperbaric air over eight weeks. There was no change in the Gross Motor Function Measure within or between groups, and the trial was stopped early because a meaningful between-group difference had become statistically improbable (Lacey and colleagues, 2012; PubMed | Our Assessment).
A multi-centre, double-blind, placebo-controlled randomised trial reached the same conclusion on efficacy. Across 111 children aged 3 to 12 years, an intention-to-treat analysis did not demonstrate a beneficial effect of HBOT, with the treated group receiving 100% oxygen at 1.75 atmospheres and the control group receiving air at 1.3 atmospheres (Muller-Bolla and colleagues, 2006; PubMed | Our Assessment). An earlier systematic review identified two randomised controlled trials and four observational studies and found that its best evidence, a randomised trial, showed HBOT at 1.75 atmospheres and 1.3 atmospheres of room air produced similar motor-function improvements of roughly 5 to 6%, with no difference between the conditions (McDonagh and colleagues, 2007; PubMed | Our Assessment).
The most recent dedicated systematic review pooled the randomised evidence directly. It identified five randomised controlled trials, four of high quality, all using 100% oxygen at 1.5 to 1.75 atmospheres, with pressurised air as the control in three and physical therapy in two. The authors concluded there is high-level evidence that HBOT is ineffective at improving motor and cognitive function in children with cerebral palsy, and moderate-level evidence that it carries a higher rate of adverse events than pressurised air (Laureau and colleagues, 2022; PubMed | Our Assessment).
Why do open-label studies of HBOT for cerebral palsy look more positive?
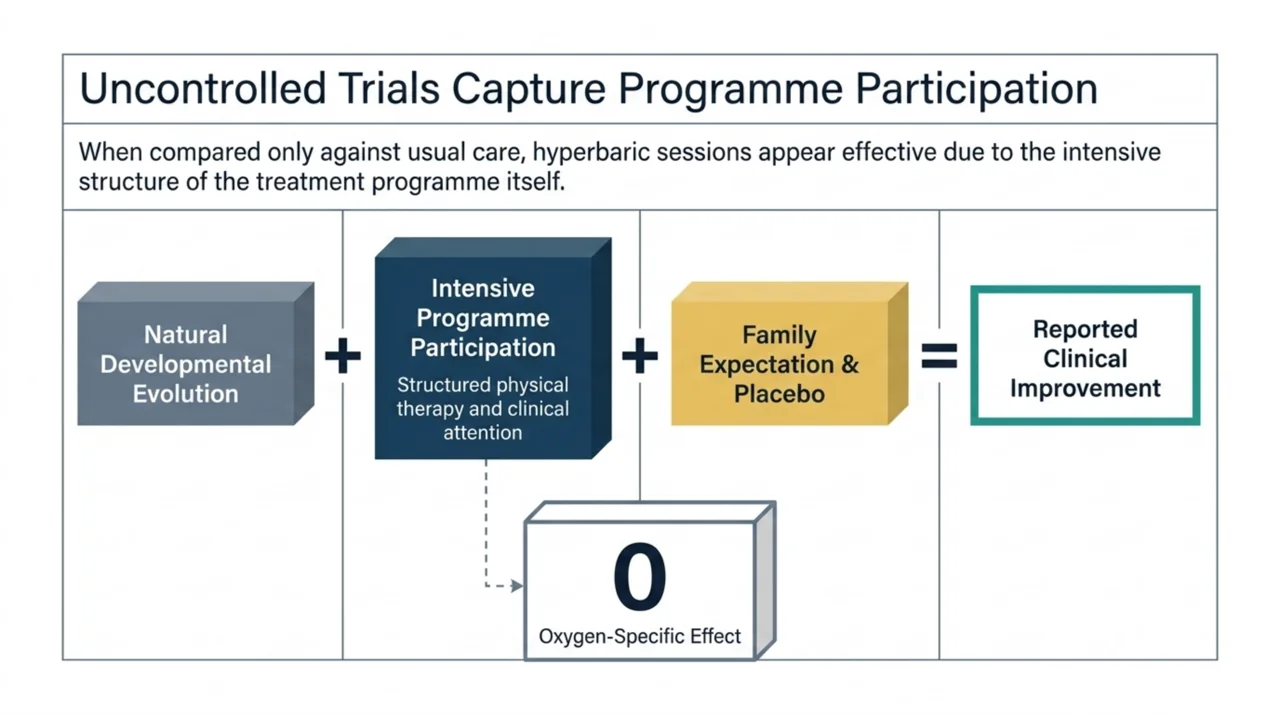
The positive signal in the literature comes mainly from studies that did not use a sham. When the comparison group receives usual care or therapy alone rather than a pressurised-air placebo, HBOT often looks effective, because the act of attending an intensive treatment programme itself drives improvement. In an open, observational longitudinal study of 150 children, all groups improved over eight months, and the three hyperbaric arms improved significantly more than rehabilitation alone. Critically, there was no significant difference between the 1.3-atmosphere air arm and the two 100% oxygen arms, which points to pressurisation and participation rather than oxygen as the active ingredient (Mukherjee and colleagues, 2014; PubMed | Our Assessment).
A more recent randomised trial of 39 children with hemiplegic cerebral palsy reported that gait parameters and functional balance improved significantly in the group that received hyperbaric oxygen plus physical therapy, while the control group that received physical therapy alone did not show the same changes; outcomes were assessed at baseline, after the intervention, and six months after treatment ended (Khalil and colleagues, 2023; PubMed | Our Assessment). Because the control group received no chamber sessions at all, this design cannot separate a true oxygen effect from the added attention, structure, and expectation of the chamber arm. That is the same confound that the sham-controlled trials were built to remove.
The largest pooled estimate comes from a 2022 systematic review and meta-analysis of 25 randomised controlled trials involving 2,146 participants, with 1,185 in the HBO group and 961 in control groups. It reported that, compared with controls, HBOT was associated with improvements in gross motor function on the Gross Motor Function Measure (standardised mean difference 0.29, 95% confidence interval 0.07 to 0.51) and on several developmental scales (Zhang and colleagues, 2022; PubMed | Our Assessment). The effect size is modest, and the result is dominated by trials whose controls were active therapy rather than sham, so it largely reflects the same open-label signal rather than overturning the blinded findings.
Not every author accepts that the question is closed. A 2024 reanalysis applied a Gross Motor Function Measure Evolution Ratio, which uses historical Gross Motor Function Classification System curves to account for the natural expected change over a study’s duration, and used it to compare hyperbaric treatment against physical therapy, selective dorsal rhizotomy, botulinum toxin, hippotherapy, and stem cell treatment (Marois and colleagues, 2024; PubMed | Our Assessment). It is a methodological argument that uncontrolled gains may still be meaningful relative to natural history, and researchers should weigh it as a reframing of the existing data, not as new blinded evidence.
How does the evidence compare across study designs?
The table below groups the key studies by design, because design is the single best predictor of whether a study reported benefit. This is the most important pattern for researchers to take away.
| Study (year) | Design | Comparator | Reported result |
|---|---|---|---|
| Lacey (2012) | Double-blind RCT, 49 children | Hyperbaric air (sham) | No within- or between-group change in gross motor function |
| Muller-Bolla (2006) | Double-blind RCT, 111 children | Air at 1.3 ATA (sham) | No beneficial effect on intention-to-treat analysis |
| Laureau (2022) | Systematic review, 5 RCTs | Sham air or physical therapy | High-level evidence HBOT is ineffective; more adverse events |
| Mukherjee (2014) | Open observational, 150 children | Rehabilitation only (no sham) | Hyperbaric arms improved more; no oxygen-specific effect |
| Khalil (2023) | RCT, 39 children | Physical therapy only (no sham) | Gait and balance improved in the HBOT-plus-therapy group |
| Zhang (2022) | Meta-analysis, 25 RCTs | Mostly active therapy | Modest pooled improvement (GMFM SMD 0.29) |
How safe is hyperbaric oxygen therapy in children with cerebral palsy?
Safety is the other half of any evidence appraisal, and here the signal is more consistent than the efficacy signal. The most common harm is middle ear barotrauma. In the multi-centre placebo-controlled trial, middle ear barotrauma occurred in 50% of children in the hyperbaric oxygen group at 1.75 atmospheres compared with 27.8% in the lower-pressure control group, a statistically significant difference, while no oxygen-toxicity events were recorded (Muller-Bolla and colleagues, 2006; PubMed | Our Assessment). The 2022 systematic review similarly graded the adverse-event rate as higher with HBOT than with pressurised air, with barotrauma affecting up to half of children (Laureau and colleagues, 2022; PubMed | Our Assessment).
Other documented events include the need for ear pressure-equalisation tube placement and, less commonly, seizures, though the precise incidence has been hard to pin down across studies (McDonagh and colleagues, 2007; PubMed | Our Assessment). For an intervention whose efficacy beyond sham has not been demonstrated, a measurable harm such as the barotrauma documented in the controlled trials above is a meaningful consideration in any risk-benefit analysis. Clinicians should also note that some children with cerebral palsy have implanted neurological devices, such as intrathecal baclofen pumps, that raise additional safety questions in the hyperbaric environment (Schiavo and colleagues, 2023; PubMed | Our Assessment).
Is HBOT an approved or recognised indication for cerebral palsy in Canada?
No. Cerebral palsy is not a recognised indication for hyperbaric oxygen therapy, and it is not on the Undersea and Hyperbaric Medical Society (UHMS) Indications list. Health Canada licenses hyperbaric chambers only for the specific conditions it recognises, and it explicitly names cerebral palsy among the conditions that some private clinics claim to treat without scientific proof (Health Canada). The current list of recognised indications is maintained separately by the UHMS (UHMS HBO Indications), and cerebral palsy does not appear on it. For researchers, this regulatory status frames cerebral palsy clearly as an investigational use rather than a standard of care.
The hyperbaric medicine community has been direct about the implications. A review of unestablished indications noted that there are now multiple randomised, blinded, sham-controlled trials of HBOT in chronic brain injury, including cerebral palsy in children, and that none showed benefit over sham, even though sham and treatment groups often both improved through a placebo or participation effect. The authors raised ethical concerns about offering paid therapy of doubtful benefit and about the reputational risk to the wider field (Mitchell and colleagues, 2014; PubMed | Our Assessment).
This tension between parental demand and limited evidence is itself a documented research-practice problem. Reviews of how clinicians should respond to families requesting unproven interventions, including hyperbaric oxygen, have framed informed, evidence-based counselling as central to ethical paediatric care (Bell and colleagues, 2011; PubMed | Our Assessment). You can compare this against the established and emerging indications catalogued elsewhere on Canada Hyperbarics, and against the full study record in our research library.
What are the open research questions and priorities?
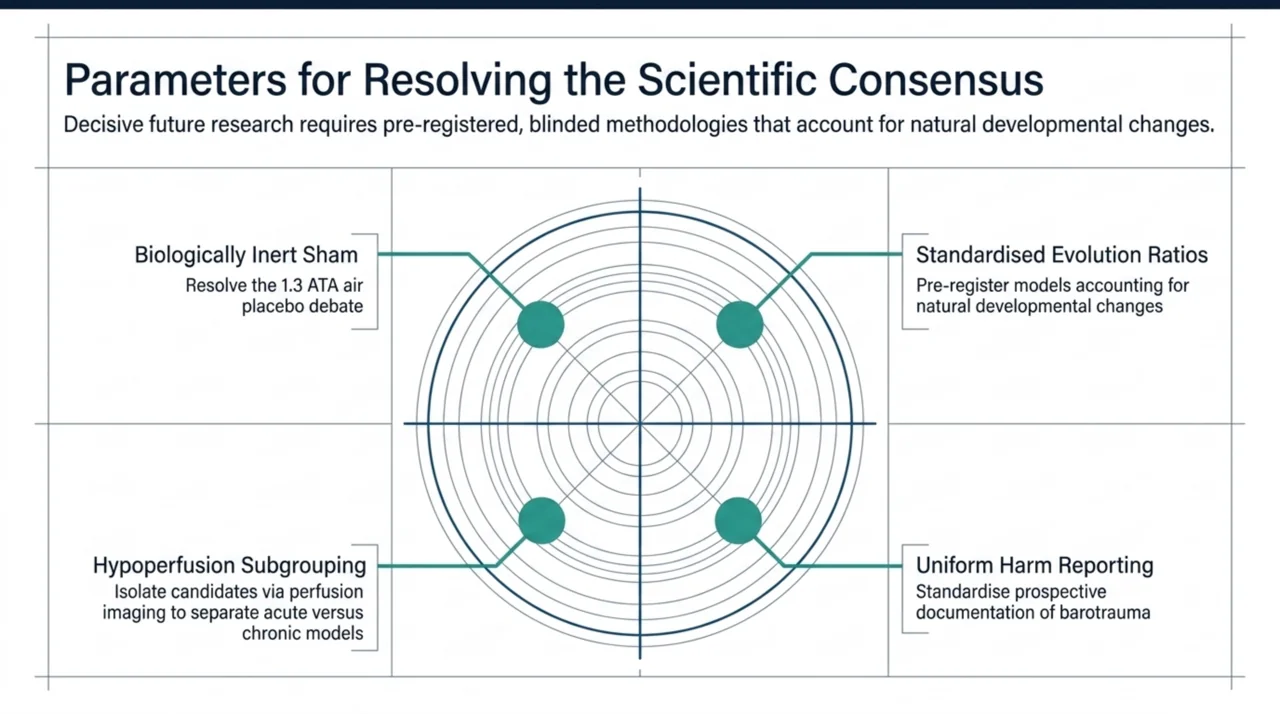
Several gaps stand out for anyone designing the next generation of studies. The numbered list below summarises where the evidence is thinnest and what a higher-quality study would need to address.
- Resolve the sham question definitively. The recurring debate is whether low-pressure air at 1.3 atmospheres is an inert placebo or a low-dose active treatment. Future trials need a control that the field agrees is biologically inert, or a clear dose-response design that settles the issue.
- Standardise outcome measures and account for natural history. The Gross Motor Function Measure Evolution Ratio approach is one attempt to separate treatment effect from expected developmental change, and future work should pre-register such methods rather than apply them retrospectively.
- Report adverse events uniformly. Barotrauma rates vary widely by pressure and protocol, and consistent, prospective harm reporting would strengthen every risk-benefit appraisal.
- Investigate biological subgroups. Perfusion imaging hints that some children have measurable hypoperfusion, but no trial has yet tested whether such children respond differently from those without it.
- Separate acute neuroprotection from chronic rehabilitation. The animal evidence concerns acute hypoxic-ischaemic injury, a fundamentally different scenario from treating established cerebral palsy years later, and the two should not be conflated in trial rationales.
Frequently asked questions
Does hyperbaric oxygen therapy cure or treat cerebral palsy?
No. There is no evidence that HBOT cures cerebral palsy, and the best controlled trials show no benefit over a pressurised-air sham. Cerebral palsy involves a fixed, non-progressive brain injury, and no therapy reverses it. HBOT for this condition remains investigational.
Why do some studies say HBOT helps children with cerebral palsy?
Studies that report benefit almost always compared HBOT against usual care rather than a sham. In those designs, the structured, intensive nature of attending chamber sessions, together with families’ expectations, produces improvement that is not specific to oxygen. Blinded sham-controlled trials remove that confound and find no oxygen-specific effect.
What is the main risk of HBOT in children with cerebral palsy?
Middle ear barotrauma is by far the most common adverse event, affecting up to half of treated children in controlled trials. Some children also need ear pressure-equalisation tubes, and seizures have been reported less often. Implanted neurological devices add further safety considerations.
Is HBOT covered by provincial health insurance for cerebral palsy in Canada?
No. Because cerebral palsy is not a recognised indication, public health plans do not fund HBOT for it, and any treatment offered at private clinics for this purpose would be out of pocket. Funded HBOT in Canada is limited to recognised indications delivered at hospitals and regulated facilities.
What pressure and number of sessions have studies used?
Most randomised trials used 100% oxygen at 1.5 to 1.75 atmospheres, typically 40 sessions over roughly eight weeks, with sham controls breathing air at 1.3 atmospheres. These protocols were chosen to test efficacy, not to establish a clinical regimen, and they did not demonstrate benefit over sham.
What would change the scientific consensus?
A large, pre-registered, blinded trial with a control the field agrees is biologically inert, standardised outcomes that account for natural developmental change, and uniform adverse-event reporting would be the most decisive contribution. Until then, the weight of high-quality evidence does not support HBOT for cerebral palsy.
The bottom line for researchers
The cerebral palsy literature is a textbook example of how study design drives conclusions. Blinded, sham-controlled trials and the systematic reviews that pool them find no benefit of hyperbaric oxygen over pressurised air, while the harm of barotrauma is real and measurable. The apparently positive open-label and active-control studies are best read as evidence of a participation effect, and the 2024 evolution-ratio reanalysis is a methodological argument worth engaging rather than a new efficacy signal. For the research community, the priority is a definitive blinded trial; for clinical practice in Canada, cerebral palsy remains an investigational, non-recognised use. Explore the underlying studies in the Canada Hyperbarics research library, review where evidence-based HBOT is actually delivered across Canada’s hospitals and regulated facilities, and learn more about our editorial approach on our About page.
Medical disclaimer: This content is for informational purposes only and does not constitute medical advice. Hyperbaric oxygen therapy for cerebral palsy is investigational and is not a recognised indication. Always consult a qualified healthcare professional before making any treatment decision.