
Outcomes tracking is the systematic capture of patient-level data – diagnosis, treatment parameters, complications, and pre- and post-treatment outcomes – to evaluate the quality and safety of hyperbaric oxygen therapy (HBOT). For Canadian clinic owners, robust outcomes tracking supports internal quality improvement, accreditation under the Undersea and Hyperbaric Medical Society (UHMS) framework, and participation in international registries that increasingly shape the evidence base for both established and emerging indications.
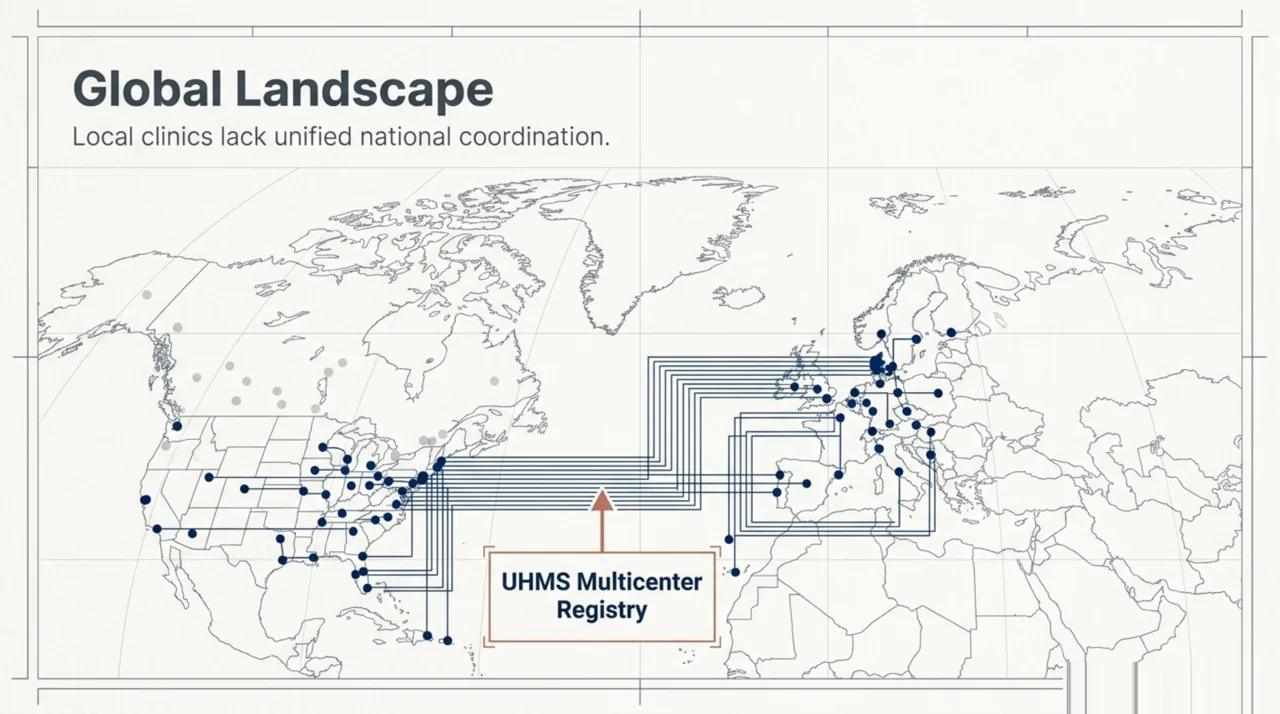
TL;DR: An HBOT patient registry is a structured, prospective dataset that records demographics, treatment protocols, pre- and post-treatment patient-reported outcomes, and complications. Canadian clinic owners can adopt the international UHMS Multicenter Registry for Hyperbaric Oxygen Therapy framework as their internal QI backbone. In a 22-centre international registry cohort of 2,880 patients, pre- to post-treatment changes in quality of life, wound-severity scores, and hearing were measurable across multiple UHMS-recognised indications (Harlan et al., 2022 – PubMed | Our Assessment). At Canada Hyperbarics we list hospitals and regulated facilities across the country at our facility directory; many already collect registry-style data internally, and a Canadian-coordinated contribution to international HBOT outcomes data is overdue.
What is HBOT outcomes tracking and why does it matter for Canadian clinics?
HBOT outcomes tracking is the structured collection of pre-treatment, intra-treatment, and post-treatment data on every patient who receives hyperbaric oxygen therapy at your clinic. The minimum dataset typically includes diagnosis, comorbidities, treatment pressure and duration, number of sessions, adverse events, and a validated patient-reported outcome measure (PROM) captured at baseline and after the treatment course.
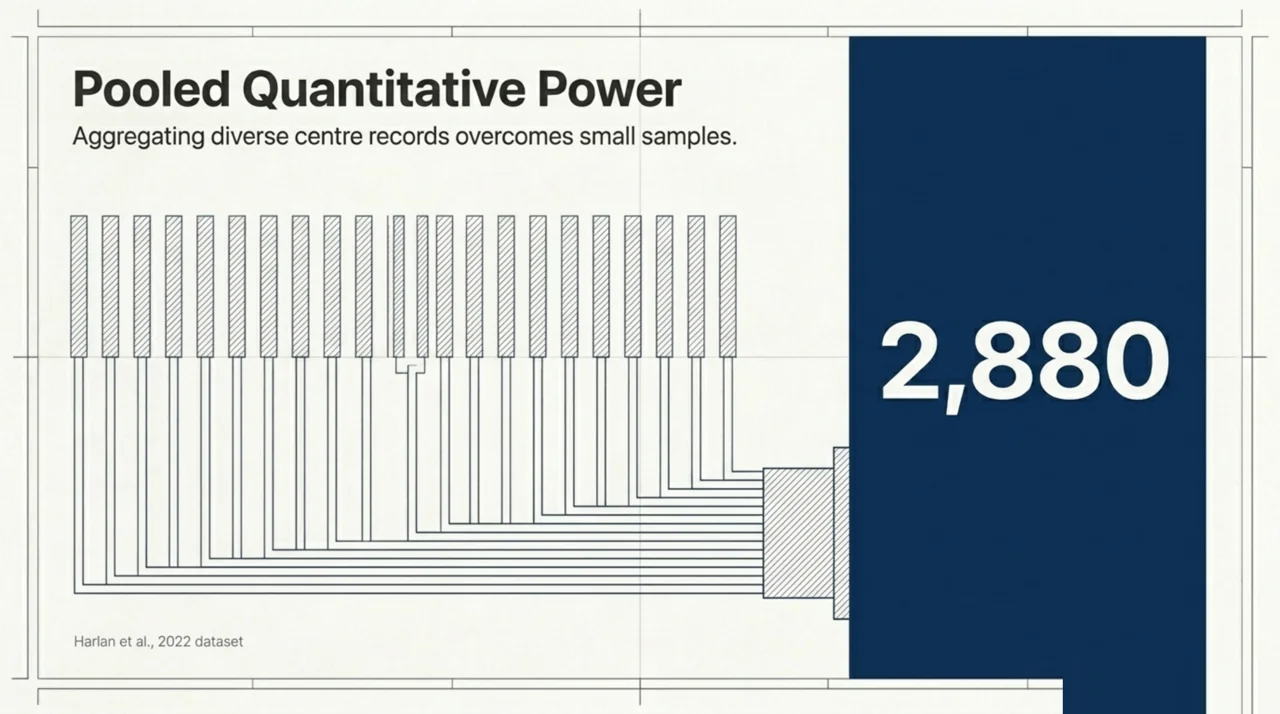
The motivation for systematic tracking is mostly statistical. A typical HBOT course involves 30 to 40 chamber sessions, and individual centres rarely accumulate large condition-specific cohorts. As Harlan and colleagues noted in their 2020 protocol paper – PubMed | Our Assessment, published HBOT outcome data tend to be from small case series because few patients with a particular condition are treated at any one centre. Pooling consistently collected data from multiple institutions is, practically, the only way to generate the cohort sizes needed to assess treatment effectiveness for both established and emerging indications.
For a clinic owner, the day-to-day value of outcomes tracking is more concrete. The same dataset that contributes to an international registry also drives internal quality improvement, supports accreditation audits, generates the documentation that referring physicians want before sending a patient, and provides the basis for credible conversations with private insurers and provincial health programs about reimbursement. Outcomes data is the single most defensible answer to the question, “how do we know your clinic delivers what the evidence says HBOT can deliver?”
Which HBOT registries can a Canadian clinic participate in?
The most established framework is the International Multicenter Registry for Hyperbaric Oxygen Therapy, coordinated through the UHMS and built on a Research Electronic Data Capture (REDCap) template. The registry was established in 2011 to capture outcomes and complications data for the UHMS-recognised indications and a selected set of unapproved indications.
Internationally, several national registries provide parallel models worth understanding:
| Registry | Coverage and reference |
|---|---|
| International Multicenter Registry for HBOT (UHMS-coordinated) | Multi-country, REDCap-based, UHMS-approved and selected unapproved indications; established in 2011 to capture outcomes and complications data across participating centres – see Harlan 2020 protocol – PubMed | Our Assessment. |
| Danish nationwide HBOT registry (population-based, linked to Danish National Patient Registry) | National linkage to civil registration with long observation windows; used to associate HBOT with 30-day mortality in 671 necrotising-soft-tissue-infection patients via inverse-probability weighting and propensity-score matching – see Hedetoft 2023 – PubMed | Our Assessment. |
| Hyperbaric Oxygen Therapy Registry (HBOTR, US payer-cost focus) | Used data from 53 centres across all payers to describe Medicare cost trends in HBOT between 2013 and 2022 – see Gelly 2024 – PubMed | Our Assessment. |
Canada does not currently operate a dedicated, nationally coordinated HBOT outcomes registry. Several Canadian hospital programs and private facilities collect registry-style internal data, and a coordinated Canadian contribution to the international registry framework remains a clear opportunity. Clinic owners interested in joining the international registry should contact the UHMS directly through uhms.org; provincial-network engagement can be discussed with the Canadian Undersea and Hyperbaric Medical Association (CUHMA).
What data should a Canadian HBOT clinic collect on every patient?
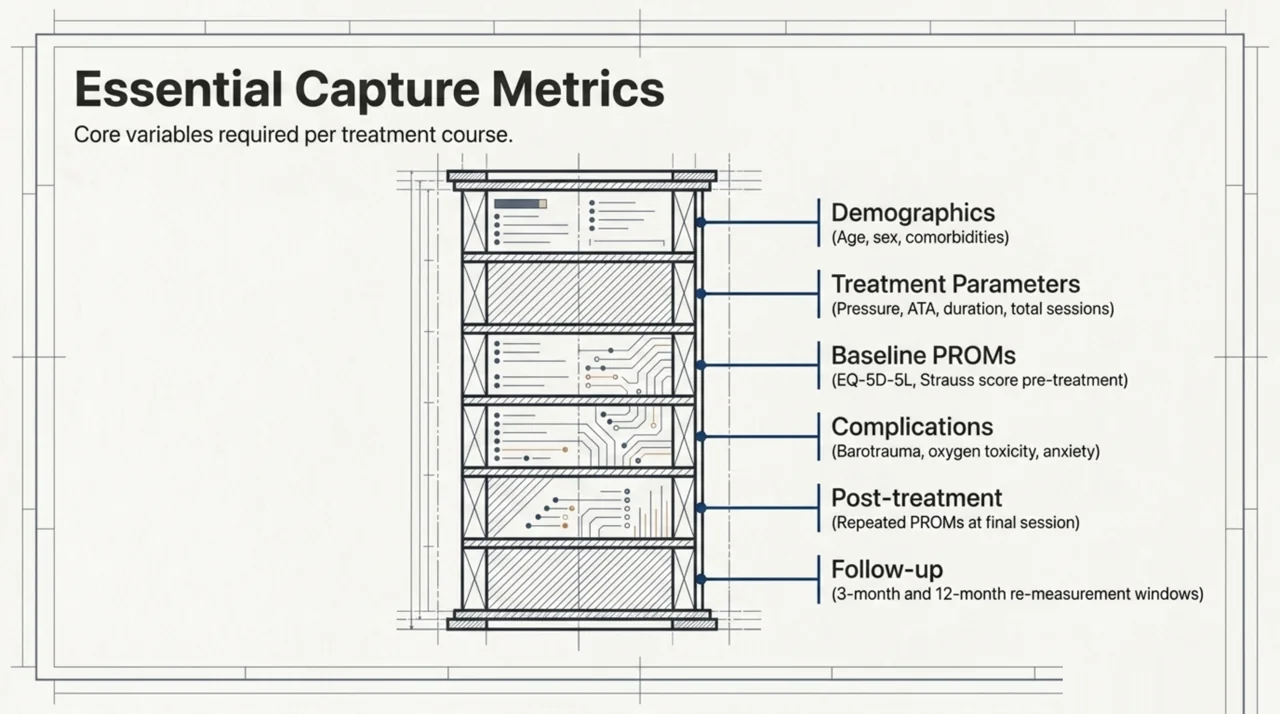
A minimum outcomes-tracking dataset, modelled on the international registry template, includes the following per patient:
- Demographics and referral source: age, sex, comorbidities (smoking status and diabetes are particularly important confounders), referring physician, and indication category.
- Treatment parameters: chamber type, treatment pressure in atmospheres absolute (ATA), session duration, number of sessions completed, any protocol deviations, and the total course length in calendar days.
- Validated baseline measure: a condition-appropriate PROM captured before the first session. The international registry uses the EQ-5D-5L general quality-of-life questionnaire across all indications, with condition-specific overlays (for example, the Strauss score for non-healing wounds and pure-tone audiometry for sudden sensorineural hearing loss).
- Complications and adverse events: middle-ear barotrauma, oxygen toxicity (central or pulmonary), confinement anxiety, and any treatment interruption.
- Post-treatment measure: the same PROMs repeated within a defined window after the final session, plus a clinically meaningful change threshold defined in advance.
- Follow-up: at minimum a 3-month and 12-month re-measurement for chronic indications, capturing durability of any observed change.
This is essentially the dataset the international registry was built around. Standardising on it has two operational advantages: it makes future participation in the international registry straightforward, and it generates the documentation that UHMS accreditation reviewers and Canadian regulators expect to see.
How do patient-reported outcome measures (PROMs) fit into a clinic’s QI program?
PROMs are short, validated questionnaires completed by patients before treatment and at defined intervals afterwards. They capture the dimensions of recovery that matter most to patients – symptom burden, function, and quality of life – in a way that is comparable across centres.
The clinical value of PROMs in HBOT is illustrated by the 2024 Multicenter Registry analysis of radiation cystitis. Moses and colleagues – PubMed | Our Assessment drew on prospectively collected registry data from 470 radiation-cystitis patients to describe patient-reported changes in haematuria and urinary symptoms between the week before and the week after a course of HBOT. That cohort size – and the consistency of the PROMs used across centres – was only possible because the data structure was agreed and registered before patient enrolment.
The 2024 emerging-indications analysis offers a second example. In a registry cohort of 9,726 patients, Tanaka and colleagues – PubMed | Our Assessment identified 378 patients (3.89%) treated for 45 emerging indications, with post-COVID-19 condition (149 patients, 39.4% of the emerging-indication group), ulcerative colitis (47, 12.4%), and Crohn disease (40, 10.6%) the most frequent. Patients with the post-COVID indication reported a significant improvement in Neurobehavioral Symptom Inventory score from pretreatment to posttreatment assessment (mean 30.6 to 14.4, p<0.001). Patients with Crohn disease reported improved EQ-5D quality of life (53.8 to 68.8). These are observational, within-cohort pre- to post-treatment changes and are not RCT-level evidence of efficacy, but they are exactly the kind of signal that justifies further controlled study, and they exist only because the registry captured them.
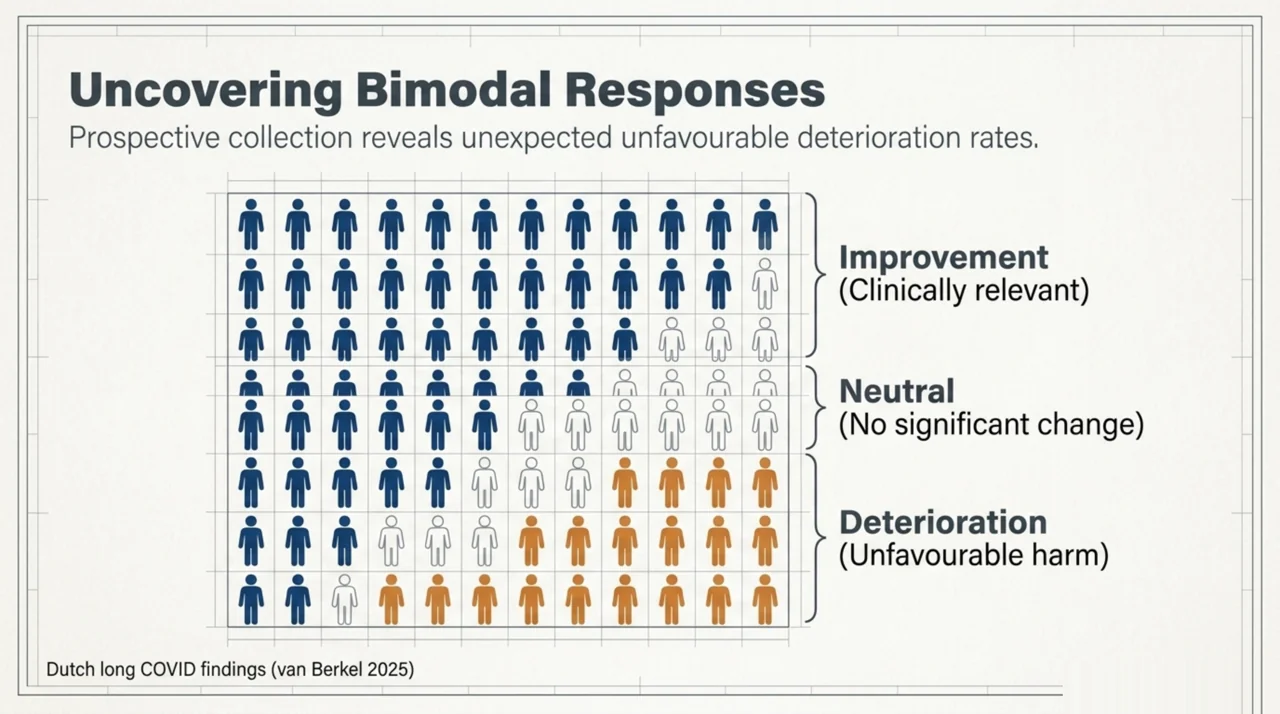
The 2025 Dutch long COVID prospective registry adds the most important methodological nuance. van Berkel and colleagues – PubMed | Our Assessment reported that 56 to 63% of long-COVID patients had a clinically relevant improvement in SF-36 mental and physical component scores 3 months after HBOT, but 13 to 19% had a clinically relevant deterioration. That kind of two-tailed signal – benefit for most, harm for some – is only visible when every patient is tracked prospectively, not just the responders. A clinic without registry-style data collection would never see the deterioration subgroup.
What does the international HBOT registry evidence show so far?
The most comprehensive picture of registry-based HBOT outcomes comes from the 2022 interim report by Harlan and colleagues – PubMed | Our Assessment. Twenty-two centres contributed data for 2,880 patients through June 2021. The most common UHMS-recognised indications were delayed radiation injury, enhancement of wound healing, and carbon monoxide poisoning. A further 125 patients were treated for non-UHMS-recognised indications. The report described significant pre- to post-treatment changes in quality of life (EQ-5D-5L), head and neck radiation symptom scores, Strauss wound scores, and hearing – with complication rates that were low and comparable to previous reports.
National registry data from Denmark provides a complementary view. The Hedetoft 2023 Danish nationwide HBOT NSTI registry study – PubMed | Our Assessment identified 671 Danish necrotising-soft-tissue-infection patients between January 2011 and June 2016 and used inverse-probability-of-treatment weighting and propensity-score matching – with prespecified variables including age, sex, weighted Charlson comorbidity score, presence of septic shock, and SAPS II – to evaluate the association between HBOT treatment and 30-day mortality. That kind of severity-adjusted nationwide analysis is only possible with population-based register coverage.
The earlier Danish nationwide NSTI cohort 2005-2018 – PubMed | Our Assessment identified 1,527 Danish patients with necrotising-soft-tissue infection between 1 January 2005 and 31 August 2018, of whom 36% received HBOT as an adjunctive therapy. The same nationwide cohort reported all-cause 30-day mortality of 19.4%, 90-day mortality of 25.2%, and 1-year mortality of 30.4%, and identified higher age, female sex, and increasing comorbidity index as independent risk factors. Admission to high-volume hospitals was associated with improved survival (odds ratio 0.59, 95% CI 0.45 to 0.77) – a structural finding about service organisation that only a nationwide register could detect.
For diabetic-wound HBOT, the Vinkel 2019 Danish national registry study – PubMed | Our Assessment described 148 patients referred to the Copenhagen HBOT chamber between 1999 and 2016 and reported sobering 5-year amputation and mortality estimates of 73.5% and 51.8% respectively – data that have direct implications for patient-selection criteria and informed-consent conversations in any Canadian diabetic-wound HBOT program.
Registry data also support utilisation and cost analysis. Gelly and colleagues, 2024 – PubMed | Our Assessment used Hyperbaric Oxygen Therapy Registry data from 53 US centres to describe Medicare cost trends between 2013 and 2022. The total Medicare cost per patient for a standard 40-treatment course decreased by 15.6%, and a single session cost roughly six hundred US dollars by the end of the decade. This is a US dataset and the dollar values do not transfer to Canada, but the methodology – using a registry to track cost-per-course over time across many centres – is directly portable to a Canadian context. It is the kind of analysis a future Canadian HBOT registry could support.
How do I build an outcomes-tracking workflow without disrupting clinic operations?
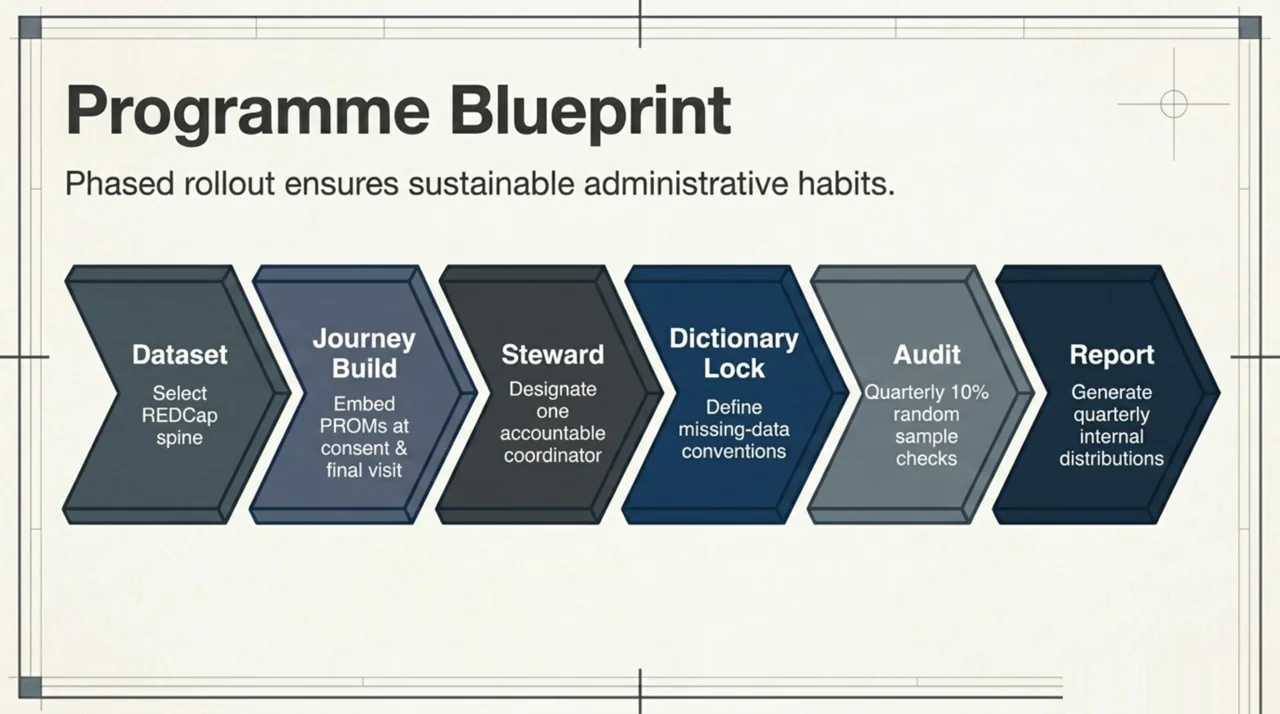
A practical implementation plan looks like this:
- Select your dataset. Start with the international registry’s REDCap template as your spine. Adopt the EQ-5D-5L across all indications. Add the condition-specific instruments you need (Strauss wound scoring, pure-tone audiometry, condition-specific PROMs).
- Build PROM capture into the patient journey. Baseline PROM at consent. Post-treatment PROM at the final-session appointment. 3-month and 12-month PROMs by secure email or patient portal, with a single phone follow-up for non-responders. The post-treatment PROM cannot be added retrospectively, so the workflow has to be built in from day one of any new tracking program.
- Designate a data steward. One named clinician or coordinator is responsible for the integrity of the dataset. Without that, completeness deteriorates quickly.
- Lock the data dictionary before you start. Variable names, units, allowed values, and missing-data conventions should be written down and agreed before the first patient is entered. Retrofitting consistency across months of free-text data is far more expensive than enforcing it from the start.
- Audit your data quarterly. Random-sample 10% of records and check completeness, internal consistency, and accurate coding of adverse events.
- Report internally every quarter. A short standing report – patients enrolled, indications, mean treatment course, PROM change scores by indication, adverse-event rate – keeps clinical and administrative leadership engaged.
What are the regulatory and privacy considerations for HBOT outcomes data in Canada?
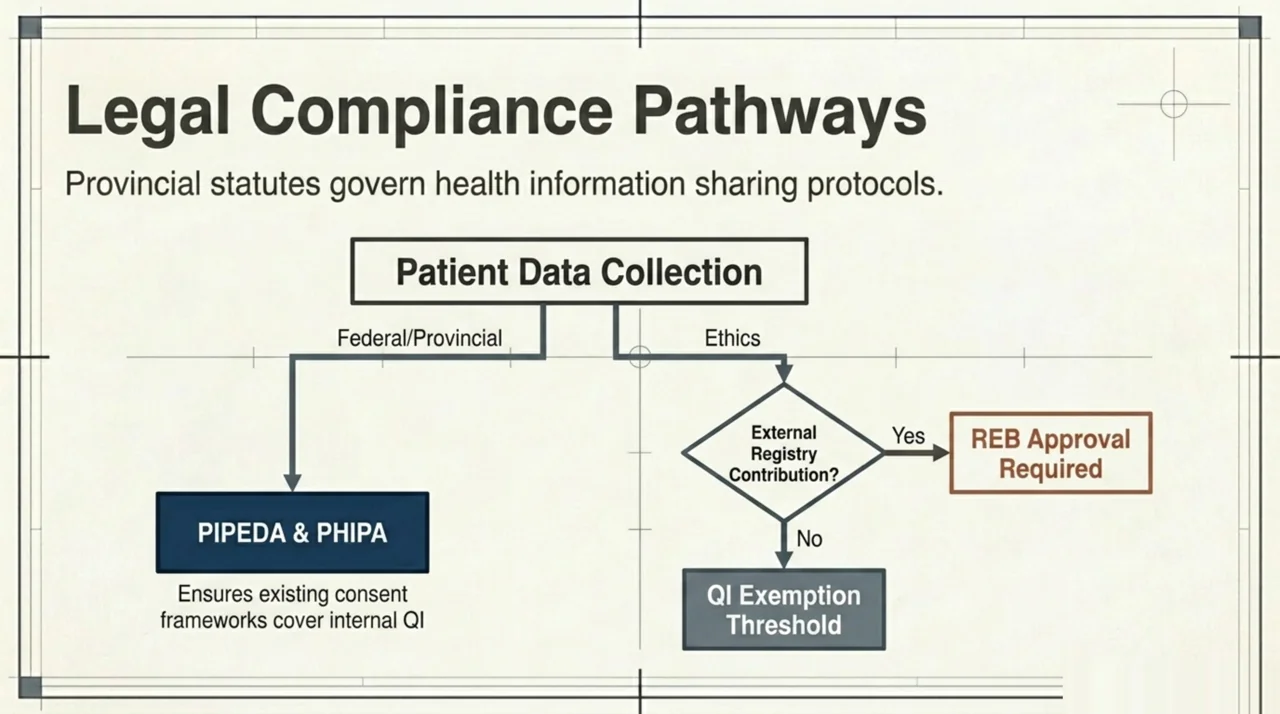
Patient-level outcomes data is personal health information (PHI). Canadian clinics are subject to the federal Personal Information Protection and Electronic Documents Act (PIPEDA) and, in most provinces, a provincial health-information statute – the Personal Health Information Protection Act (PHIPA) in Ontario, the Personal Health Information Act in Manitoba and Nova Scotia, and parallel statutes elsewhere. Before any outcomes-tracking program goes live:
- Confirm your collection, use, and disclosure are covered by your existing privacy framework and consent forms. Internal QI use generally is; contribution of de-identified data to an international registry usually requires an explicit additional consent line.
- Identify whether your activity meets the threshold of research that requires Research Ethics Board (REB) approval. Quality-improvement work is typically exempt; multicentre registry contribution often is not.
- Confirm that any chamber, monitoring, or data-capture device involved is a Health Canada-licensed medical device as required for its risk class.
- Maintain a documented data-retention and destruction schedule.
For a deeper review of regulatory expectations for Canadian HBOT clinics, see our overview at canadahyperbarics.ca/regulatory/ and the provincial-coverage details at canadahyperbarics.ca/hbot-coverage-canada/.
How can clinic owners use outcomes data for accreditation and reimbursement conversations?
Two practical use cases recur in Canadian clinic operations.
Accreditation. UHMS Clinical Hyperbaric Facility Accreditation requires evidence of an active quality assurance program with documented outcomes review. A structured registry-style dataset is the cleanest way to satisfy that requirement. Clinics that have already adopted the international registry template will find that most of what an accreditation surveyor asks for is already in the export.
Reimbursement and referral conversations. Outcomes data is the strongest single artefact a Canadian clinic can bring to a conversation with a private insurer, a provincial program administrator, or a referring physician. Aggregate, de-identified outcome distributions – mean PROM change by indication, adverse-event rate, completion rate – give those audiences something concrete to evaluate. Anecdote does not move reimbursement policy; comparable, prospectively collected outcomes data eventually does. The Canada Hyperbarics independent-directory mission is built on the same premise: comparable, verifiable data is the only way to support trust at scale.
Frequently Asked Questions
Does Canada have a national HBOT outcomes registry?
Not as of 2026. Several Canadian hospital programs and private facilities collect registry-style internal data, and Canadian patients are represented in the international Multicenter Registry for HBOT through a small number of participating centres, but a dedicated nationally coordinated Canadian registry does not exist. CUHMA is the logical sponsor for any future Canadian effort, and the international registry’s REDCap template provides a ready-made structure that a Canadian project could adopt directly.
How long does outcomes tracking take per patient?
For a clinic with a single dedicated data coordinator and an electronic data-capture template, baseline data entry plus PROM administration adds roughly 10 to 15 minutes per patient at consent, 5 to 10 minutes at the post-treatment visit, and a few minutes per follow-up touchpoint. The largest one-time cost is workflow design and staff training, not the per-patient time itself.
What PROM should we use for a wound-focused HBOT program?
The international registry pairs the general EQ-5D-5L with the Strauss score for non-healing wounds. Strauss assesses several wound-specific dimensions (appearance, depth, infection status, etc.) and produces a numeric score sensitive to clinically meaningful change. Other validated wound instruments exist; the operational principle is to choose one, register the choice in your data dictionary, and apply it consistently.
Do we need Research Ethics Board approval to track outcomes internally?
Internal quality-improvement activity is typically exempt from REB review under the Tri-Council Policy Statement (TCPS 2) framework that governs research with humans in Canada. The picture changes when the activity is designed to contribute generalisable knowledge – for example, when you plan to contribute data to an external registry, present at a conference, or publish a case series. In those cases, REB approval is usually required. Speak to your institution’s REB or, for an independent clinic, a regional REB before assuming exemption.
Can a small Canadian clinic meaningfully contribute to an international registry?
Yes. The international registry is explicitly designed so that small centres can contribute. The registry’s analytical value comes from pooling small contributions from many centres – that was the founding premise of the entire project, as Harlan and colleagues set out in the 2020 protocol paper – PubMed | Our Assessment. A clinic that treats 80 patients per year still contributes meaningfully to a multi-thousand-patient pooled cohort.
What is the minimum follow-up window for chronic indications?
A reasonable default is a baseline PROM, an immediate post-treatment PROM, a 3-month follow-up, and a 12-month follow-up. The 12-month point matters because some HBOT benefit is durable and some is not, and that distinction is invisible at 3 months. The 2025 Dutch long COVID prospective registry, for example, scheduled follow-up at baseline, post-treatment, 3 months, and 1 year – the 3-month results are published and the 1-year results are still being collected.
Where can I find a directory of Canadian HBOT facilities for reference benchmarking?
Canada Hyperbarics maintains a directory of hospitals and regulated facilities across the country at canadahyperbarics.ca/facilities/. The directory is independently maintained and includes both public hospital programs and private clinics. It is a useful starting point for benchmarking your own clinic against the wider Canadian landscape.
Next steps for Canadian HBOT clinic owners
If your clinic is not yet running structured outcomes tracking, the most actionable single step is to adopt the EQ-5D-5L as your baseline PROM across all indications, beginning with the next consented patient. That single change – one validated questionnaire, captured pre- and post-treatment – is the foundation of every registry program in the published literature. Layer in condition-specific instruments, complications coding, and follow-up timing from there.
For a wider view of Canadian HBOT regulation, accreditation, and provincial coverage that informs how registry data is used in practice, see our regulatory overview, our provincial coverage guide, and the directory of hospitals and regulated facilities.
This content is for informational purposes only and does not constitute medical advice. Clinic owners should consult their institutional privacy officer, accreditation body, and Research Ethics Board before initiating any new outcomes-tracking program.