
TL;DR: Radiation cystitis is a chronic bladder injury that affects an estimated 5 to 10 percent of people treated with radiotherapy for pelvic cancers. The RICH-ART randomised controlled trial found that hyperbaric oxygen therapy alleviated urinary symptoms, and its 2025 long-term follow-up examined whether that relief was sustained over five years. Recent systematic reviews report high response rates for haemorrhagic cystitis but caution that most supporting data are observational. Hyperbaric oxygen therapy is a recognised treatment for delayed radiation injury and is offered at hospitals and regulated facilities across Canada.
Reading time: about 8 minutes. This is an evidence review written for researchers and clinicians.
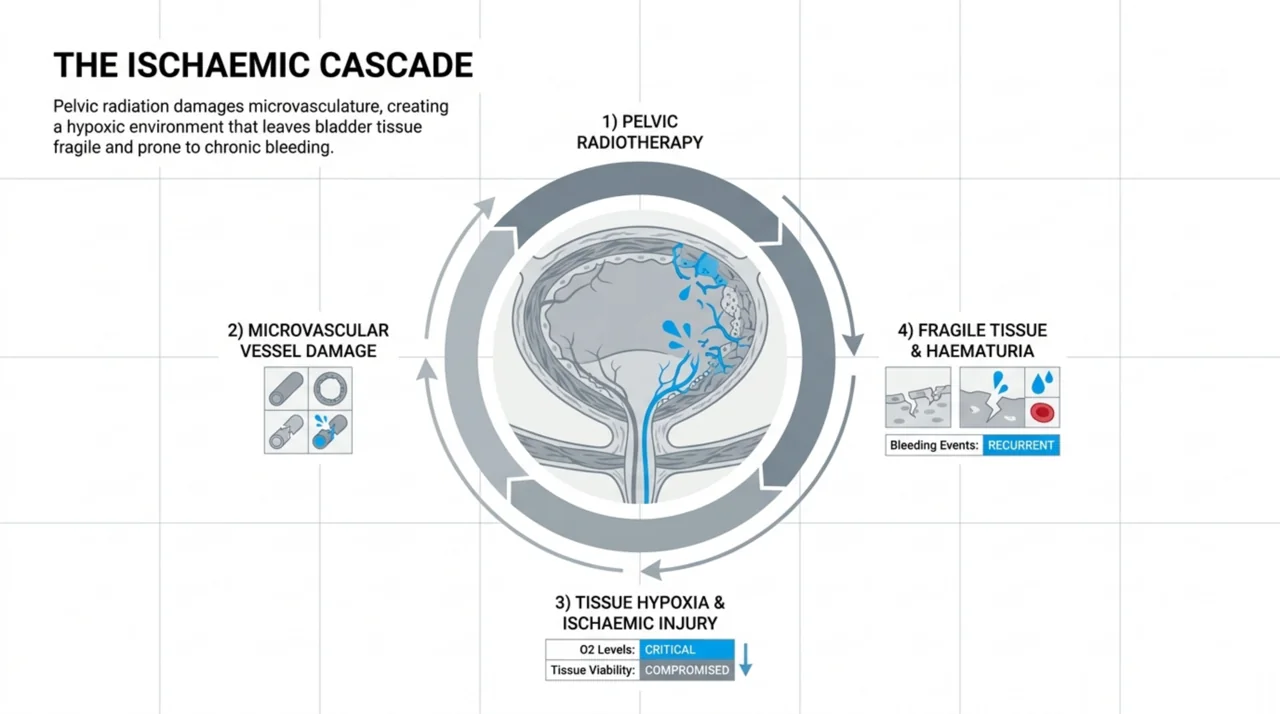
Radiation cystitis is a chronic inflammation of the bladder wall caused by earlier radiotherapy to the pelvis. It develops because radiation damages the small blood vessels of the bladder lining, leaving the tissue hypoxic, fragile, and prone to bleeding. For researchers, the central question is whether hyperbaric oxygen therapy for radiation cystitis can reverse that hypoxia and restore durable bladder function, rather than simply controlling a bleed in the short term. This review summarises what the strongest recent studies actually report, including a Nordic randomised controlled trial and two 2026 evidence syntheses indexed in our research library. Canada Hyperbarics maintains this database so that practitioners can read the primary evidence alongside our own assessments.
What is radiation cystitis, and why is it difficult to treat?
Radiation cystitis is one of the late adverse effects of pelvic radiotherapy. Its symptoms include haematuria (blood in the urine), urinary urgency, increased frequency, dysuria, and urinary retention. As the authors describe it, the condition results from hypoxic and ischaemic injury, which leaves the bladder lining fragile and prone to bleeding (Soriano and colleagues, PubMed | Our Assessment).
The condition is difficult to manage because the affected tissue does not behave like a normal bladder. A 2026 review of radiotherapy effects on the lower urinary tract noted that these late complications can present in the decades following treatment, usually with greater symptom severity, and that irradiated patients tend to have less favourable outcomes when standard, non-radiation treatment strategies are applied. That same review identified hyperbaric oxygen therapy as a treatment with successful outcomes for haemorrhagic cystitis (Sarafis and colleagues, PubMed | Our Assessment). This is why hyperbaric oxygen has been studied as an option when conventional measures fail.
What did the RICH-ART randomised trial find about hyperbaric oxygen therapy?
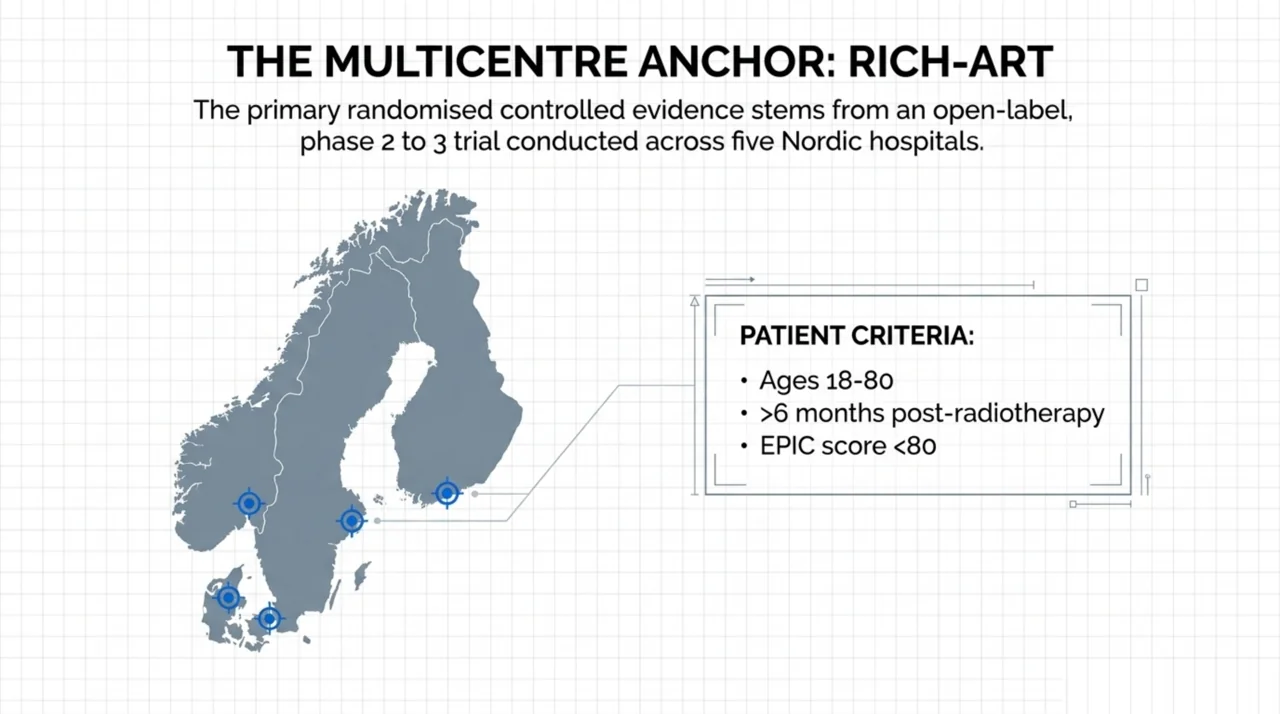
As the only randomised controlled trial dedicated to this question in the recent literature, the RICH-ART trial is the natural anchor for an evidence review. It is a multicentre, open-label, phase 2 to 3 randomised controlled trial conducted at five Nordic hospitals in Sweden, Norway, Denmark, and Finland. Eligible patients were aged 18 to 80, had completed pelvic radiotherapy at least 6 months earlier, had chronic radiation-induced cystitis, and scored below 80 on the Expanded Prostate Cancer Index Composite (EPIC) urology measure. They were randomised to receive hyperbaric oxygen (30 to 40 sessions of 100 percent oxygen breathed at 240 to 250 kPa, roughly 2.4 to 2.5 atmospheres absolute, for 80 to 90 minutes daily) or standard of care (Oscarsson and colleagues, PubMed | Our Assessment).
The trial’s primary outcome, the change in EPIC urinary score from baseline to 6 months, was reported earlier and showed that hyperbaric oxygen alleviated urinary symptoms. Because evidence on whether that benefit lasts has been limited, the 2025 publication reports the secondary outcome: long-term symptom relief at a 5-year follow-up. After the 6-month point, control-group patients were offered hyperbaric oxygen as well, a crossover design that should be kept in mind when interpreting the longer-term comparison. The open-label nature of the trial, with no masking of patients or assessors, is its main methodological limitation.
How strong is the wider evidence base for HBOT in radiation cystitis?
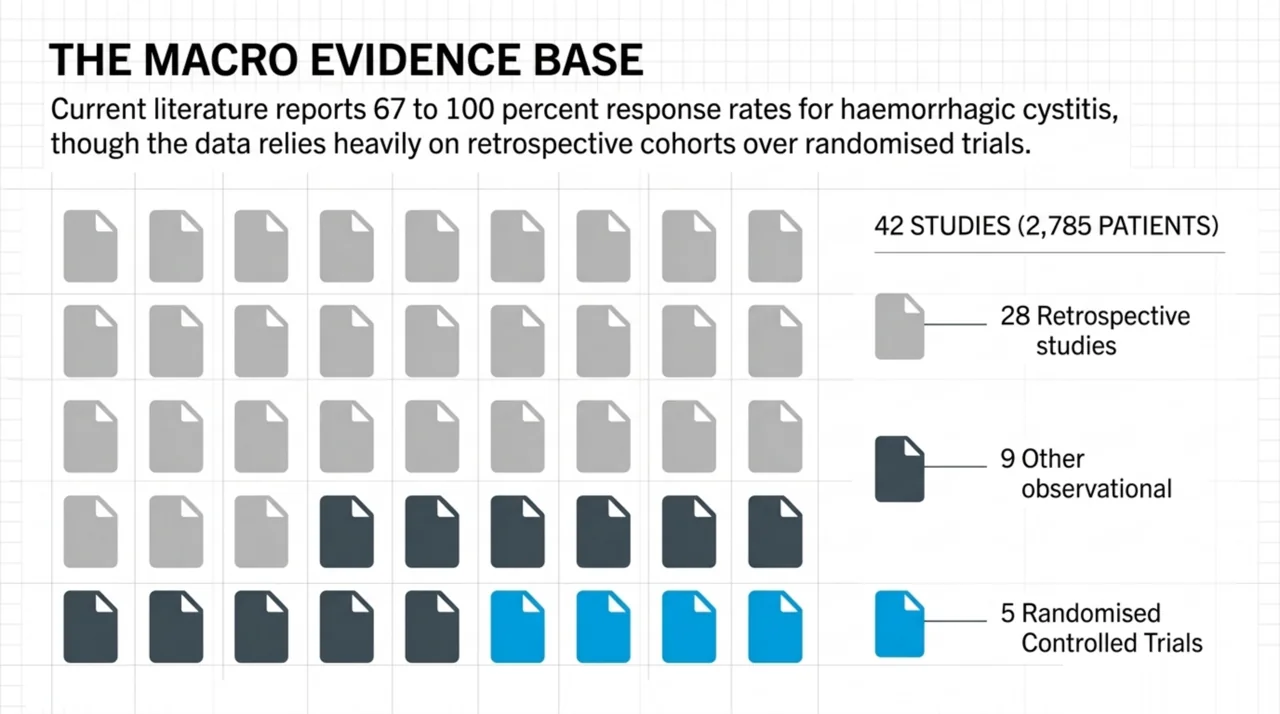
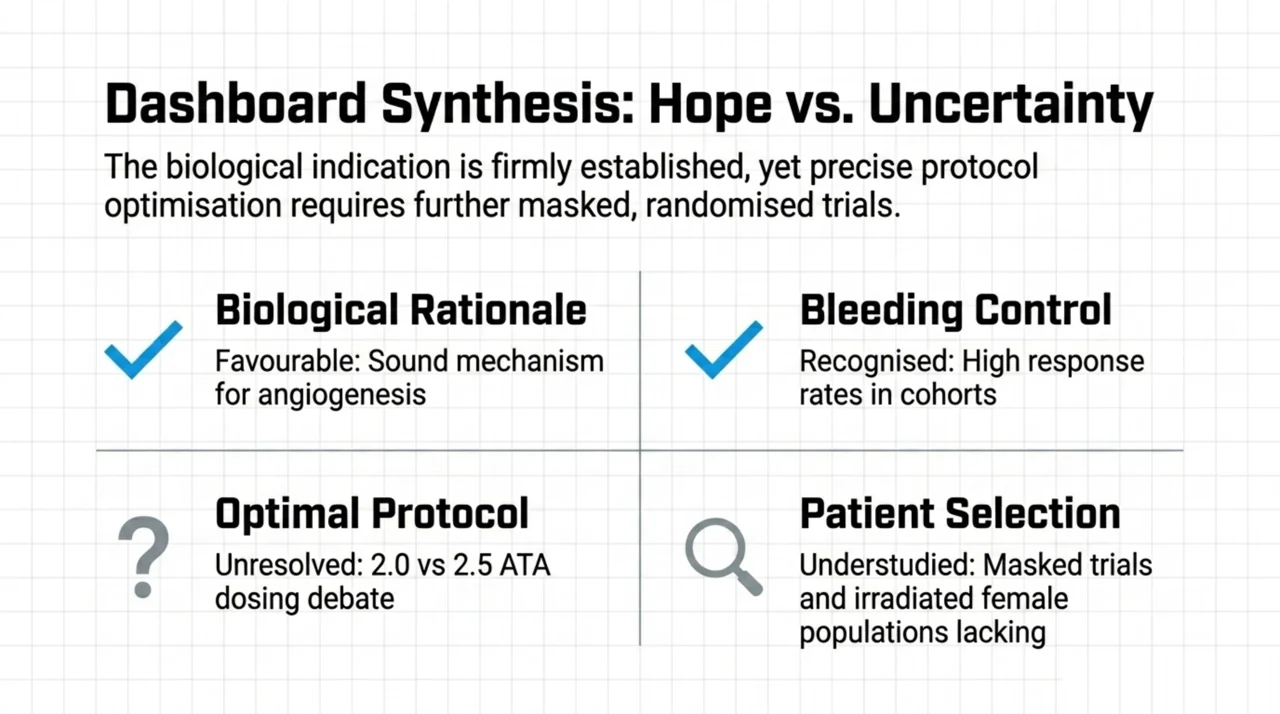
A 2026 systematic review captured the broader picture well, and its title, “Between hope and uncertainty,” is apt. Searching three databases, the authors included 42 studies covering 2,785 patients, of which 28 were retrospective and only 5 were randomised controlled trials. Hyperbaric oxygen was used mainly to manage toxicity, at a median of 34.5 sessions, and the pelvic region was the single largest patient group. For haemorrhagic cystitis specifically, the included studies reported response rates of 67 to 100 percent, although the authors stressed that the evidence is heterogeneous and often limited by small cohorts (Cuccia and colleagues, PubMed | Our Assessment). Notably, in other sites such as breast and head-and-neck cancer, randomised trials in that review failed to demonstrate consistent benefit, which is a useful reminder not to generalise the cystitis signal to every radiation injury.
A clinically focused 2026 review in a high-impact oncology journal framed the biological rationale: hyperbaric oxygen is thought to promote angiogenesis, fibroblast activation, and tissue remodelling in hypoxic environments, which is the basis for its use across radiation cystitis, skin fibrosis, bone necrosis, and proctitis. The same review highlighted the open questions that still limit confident recommendations, including patient selection, the optimal treatment protocol, and long-term outcomes (Dejonckheere and colleagues, PubMed | Our Assessment).
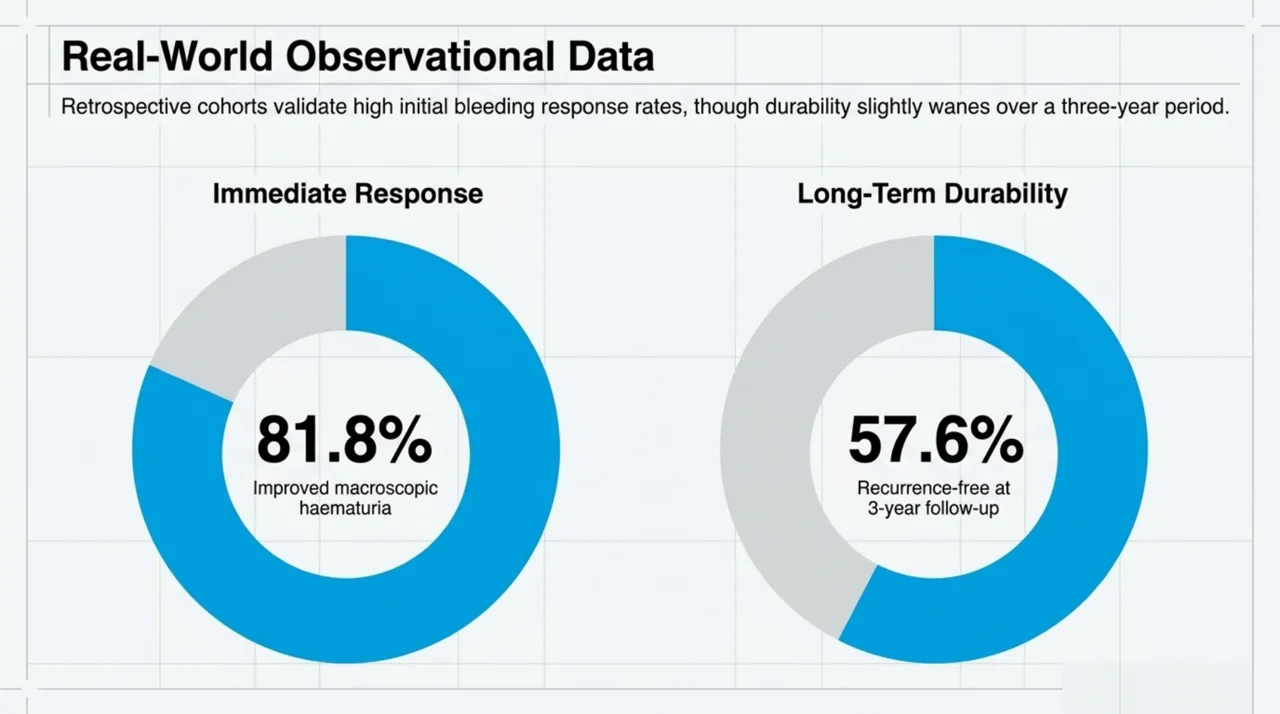
Real-world cohorts point in the same direction while underscoring the limits of observational data. In a retrospective analysis of 33 patients with viral or radiation-induced haemorrhagic cystitis treated at 2.5 atmospheres absolute, 81.8 percent (27 of 33) showed improvement in macroscopic haematuria, and the condition did not recur in 57.6 percent over three years of follow-up. Radiation-induced cases were associated with higher grades of haematuria than viral cases in that cohort (Fraga Carvalho and colleagues, PubMed | Our Assessment). Because this was a retrospective study with a mixed cohort, the findings describe an association rather than proof of cause.
Does treatment pressure matter: 2.0 versus 2.5 ATA?
The optimal pressure for treating radiation cystitis remains unsettled, and a 2026 retrospective chart review tried to narrow it down. Comparing 93 patients with haemorrhagic radiation cystitis treated at either 2.0 or 2.5 atmospheres absolute across two sites, fewer patients in the 2.5 ATA group experienced gross haematuria within one year of therapy than in the 2.0 ATA group, a difference that reached statistical significance. However, the time to haematuria recurrence did not differ between the groups (10.2 versus 9.6 months), and no difference was seen in other urinary symptoms. Adverse events were higher at 2.5 ATA when modelled with mixed-effects logistic regression (Soriano and colleagues, PubMed | Our Assessment). Because the design was retrospective, these results are best read as associations that point toward a dose-response trade-off rather than as a definitive protocol recommendation.
How do the key studies compare?
| Study (year) | Design | Patients | Key reported finding |
|---|---|---|---|
| Oscarsson, RICH-ART (2025) | Open-label randomised controlled trial | Multicentre, 5 Nordic hospitals | HBOT alleviated urinary symptoms; 5-year follow-up assessed durability |
| Cuccia (2026) | Systematic review | 42 studies, 2,785 patients | 67 to 100 percent response for haemorrhagic cystitis; evidence heterogeneous |
| Soriano (2026) | Retrospective chart review | 93 | Fewer gross-haematuria recurrences at 2.5 ATA, but more adverse events |
| Fraga Carvalho (2025) | Retrospective cohort | 33 (viral and radiation) | 81.8 percent improved macroscopic haematuria; 57.6 percent recurrence-free at 3 years |
| Pereira (2025) | Retrospective surgical series | 17 | Supratrigonal cystectomy reserved as a last resort after other therapy fails |
Where does hyperbaric oxygen fit among other radiation cystitis treatments?
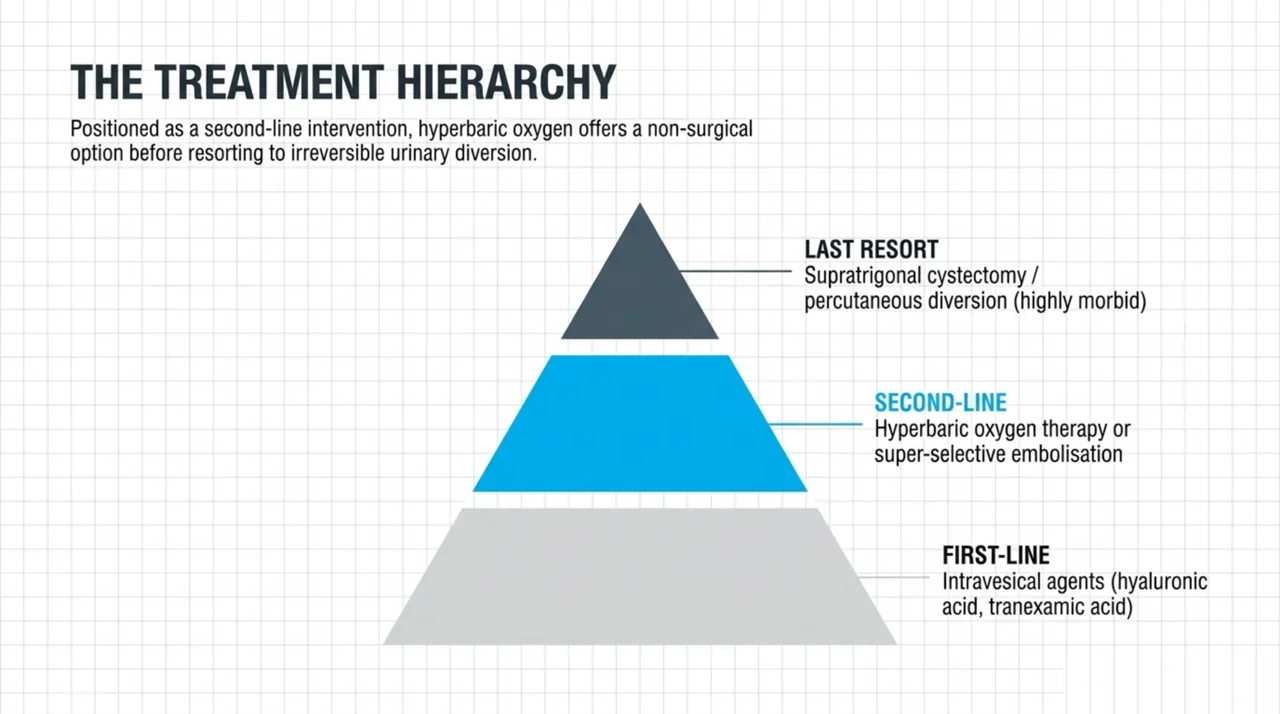
Hyperbaric oxygen is generally positioned as a second-line option rather than a first move. A 2025 literature review of intractable haematuria management proposed a treatment escalation plan in which first-line care includes intravesical agents such as hyaluronic acid, tranexamic acid, and others, second-line treatment includes hyperbaric oxygen therapy or super-selective embolisation, and percutaneous diversion or cystectomy is reserved as a last resort. The same review acknowledged that the overall evidence base for most of these modalities is weak, with a shortage of randomised trials (Mihailidis and colleagues, PubMed | Our Assessment).
When all conservative options fail, surgery becomes the last line. A retrospective series of 17 patients reported supratrigonal cystectomy with urinary diversion for refractory radiation-induced haemorrhagic cystitis, a procedure the authors reserved for those who had exhausted prior therapy because of its associated morbidity (Pereira and colleagues, PubMed | Our Assessment). Set against that backdrop, a non-surgical option that can reduce bleeding has clear appeal, which is part of why delayed radiation injury remains such a common reason for hyperbaric referral.
Indeed, a 2026 review of delayed radiation injuries reported that, based on United States billing records, delayed radiation injury is the most frequent indication for hyperbaric treatment, accounting for roughly 40 percent of those billings. That review also cautioned that hyperbaric oxygen should not be the sole treatment for many radiation injuries and that a multidisciplinary approach is usually required (Feldmeier and colleagues, PubMed | Our Assessment). For referring clinicians, radiation cystitis sits within the broader category of delayed radiation injury.
What are the limitations and research gaps?
The honest summary is that the cystitis signal is encouraging but the evidence is still thin where it matters most. In the largest systematic review, 28 of 42 studies were retrospective and only 5 were randomised, so the body of work leans heavily on observational data. Even the strongest trial, RICH-ART, was open-label and used a crossover after 6 months. Several recurring gaps stand out for anyone designing future studies:
- Optimal dose is unresolved. Whether 2.0 or 2.5 ATA offers the best balance of bleeding control and safety is still an open question driven by retrospective data.
- Patient selection is poorly defined. Reviews repeatedly flag the lack of agreed criteria for who benefits most.
- Long-term outcomes need more masked trials. Most durability data come from a single open-label trial and observational follow-up.
- The irradiated female population is understudied. One 2026 review called specifically for more research focused on women treated for pelvic malignancies.
Is hyperbaric oxygen therapy for radiation cystitis available in Canada?
Yes. Radiation cystitis falls under delayed radiation injury, which is one of the indications recognised by the Undersea and Hyperbaric Medical Society (UHMS). In Canada, hyperbaric oxygen therapy for recognised indications is delivered through hospitals and regulated facilities, and you can search for treating programmes in our directory of hospitals and regulated facilities. Coverage and referral pathways vary by province, so patients should confirm details with their treating team. Canada Hyperbarics curates the underlying studies and our plain-language assessments in the research database so that clinicians and researchers can verify each claim against the primary source.
Frequently asked questions
What is radiation cystitis?
Radiation cystitis is a chronic inflammation and injury of the bladder caused by previous radiotherapy to the pelvis. It can cause haematuria, urgency, frequency, and pain, sometimes years after treatment, and it affects an estimated 5 to 10 percent of people who receive pelvic radiotherapy.
Does hyperbaric oxygen therapy cure radiation cystitis?
The evidence shows symptom relief rather than a guaranteed cure. The RICH-ART randomised controlled trial found that hyperbaric oxygen alleviated urinary symptoms, and observational cohorts report high rates of improvement in bleeding. Results vary between patients, and not everyone responds.
How many hyperbaric oxygen sessions are used for radiation cystitis?
Protocols vary. The RICH-ART trial used 30 to 40 sessions, the largest systematic review reported a median of 34.5 sessions across radiation indications, and one real-world cohort used a median of 11 sessions. The exact number is individualised to the patient and their response.
What pressure is used for hyperbaric oxygen in radiation cystitis?
Most studies use pressures between about 2.0 and 2.5 atmospheres absolute. A 2026 retrospective comparison found fewer gross-haematuria recurrences at 2.5 ATA but more adverse events, so the optimal pressure is still being debated.
Is hyperbaric oxygen for radiation cystitis supported by randomised trials?
Partly. The RICH-ART trial is a randomised controlled trial that supports symptom relief, but most of the wider evidence is observational. Reviewers consistently call for more masked, randomised studies to confirm long-term benefit and define the best protocol.
Where can I read the studies behind these claims?
Every study cited here links to both the primary source on PubMed and our own assessment in the Canada Hyperbarics research database. You can also browse our frequently asked questions for plain-language explanations.
The bottom line for researchers
Hyperbaric oxygen therapy for radiation cystitis rests on a single open-label randomised trial supported by a large but mostly observational literature that reports high response rates for bleeding control. The biological rationale is sound, the safety profile is acceptable at standard pressures, and delayed radiation injury remains one of the most common reasons for hyperbaric referral. The clearest path forward is masked, randomised research that settles dose, patient selection, and long-term durability. To find treating programmes, see our directory of hospitals and regulated facilities.
This content is for informational purposes only and does not constitute medical advice. Hyperbaric oxygen therapy should be discussed with a qualified physician, and treatment decisions should be made on an individual basis in consultation with your care team.