TL;DR: Hyperbaric oxygen therapy (HBOT) has no dedicated tinnitus trials in the current evidence base. Almost all of the relevant research studies sudden sensorineural hearing loss (SSNHL), a condition where tinnitus is a common accompanying symptom. Within that SSNHL literature, results are mixed: some retrospective and cohort studies report an association between HBOT and better hearing recovery, while at least one prospective multicentre study and one propensity matched analysis found no statistically significant benefit once confounding factors were controlled for. The honest summary is that HBOT’s role in hearing recovery, and by extension tinnitus that accompanies it, remains an open question that referring physicians should discuss individually with patients, not a settled treatment claim.
Hyperbaric oxygen therapy tinnitus questions come up often in referral conversations, usually because a patient’s tinnitus started alongside a sudden drop in hearing. Hyperbaric oxygen therapy is a treatment in which a patient breathes 100 percent oxygen inside a pressurized chamber, raising the amount of oxygen dissolved in blood plasma well above what normal breathing can achieve. It is used across a range of approved indications, and researchers have also studied it as an adjunct treatment for sudden sensorineural hearing loss (SSNHL), a condition in which tinnitus frequently appears alongside the hearing change itself.
This article works from a defined pool of recent, peer reviewed studies. None of them are tinnitus trials in the strict sense. All of them study SSNHL, its causes, its prognosis, or its treatment with HBOT, usually as an add on to steroid therapy. That distinction matters, and we want to be upfront about it rather than stretch the evidence to fit the keyword.
What Is Hyperbaric Oxygen Therapy, and Why Does It Come Up for Hearing Loss?
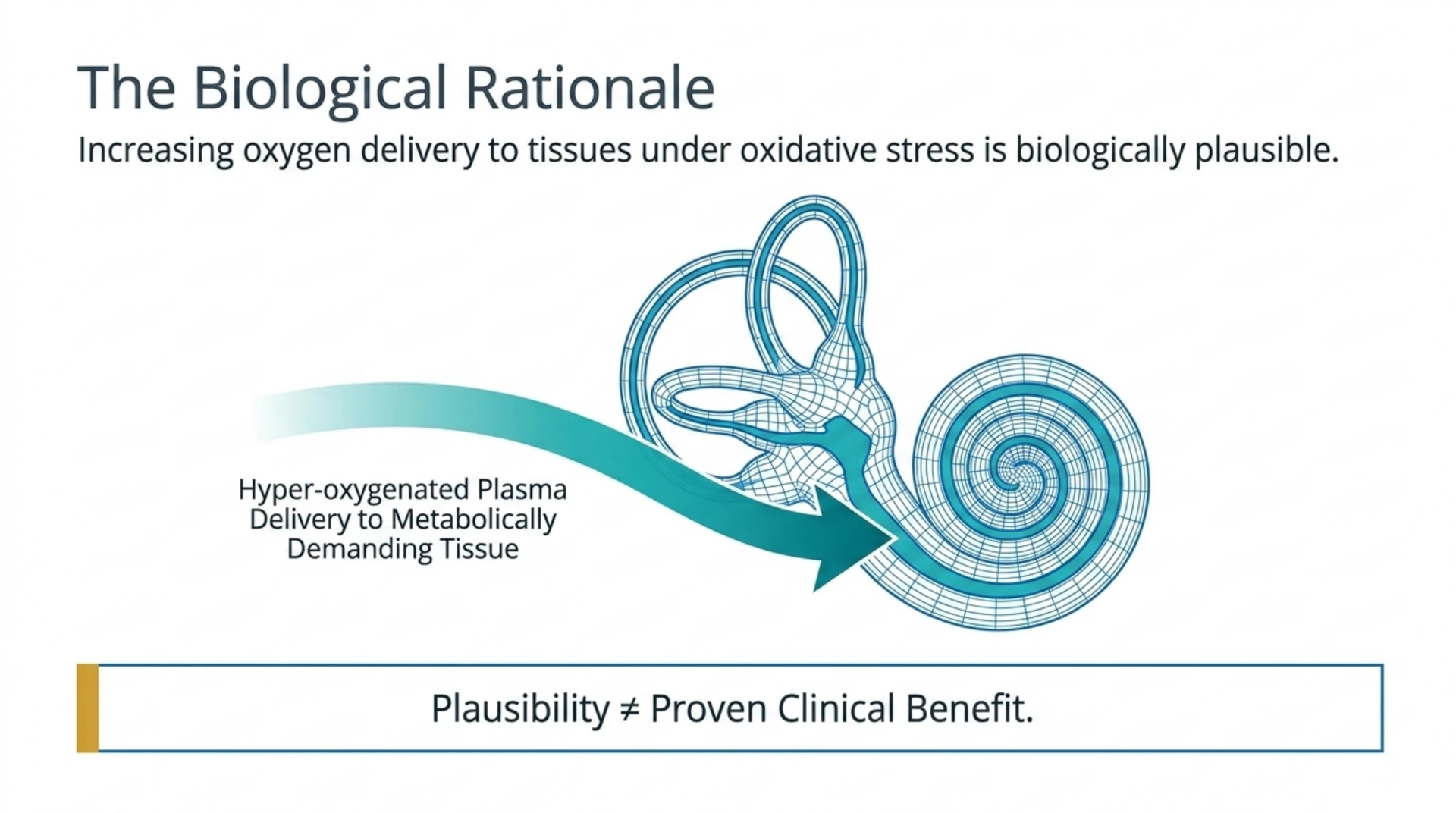
Hyperbaric oxygen therapy increases oxygen delivery to tissues that may be poorly perfused or under oxidative stress. The inner ear’s cochlea is metabolically demanding and sensitive to interruptions in its blood supply, which is the physiological rationale researchers give for testing HBOT in sudden sensorineural hearing loss. The rationale is biologically plausible, but plausibility is not the same as proven clinical benefit, and the studies below show why that distinction is worth holding onto.
Does Hyperbaric Oxygen Therapy Treat Tinnitus Directly?
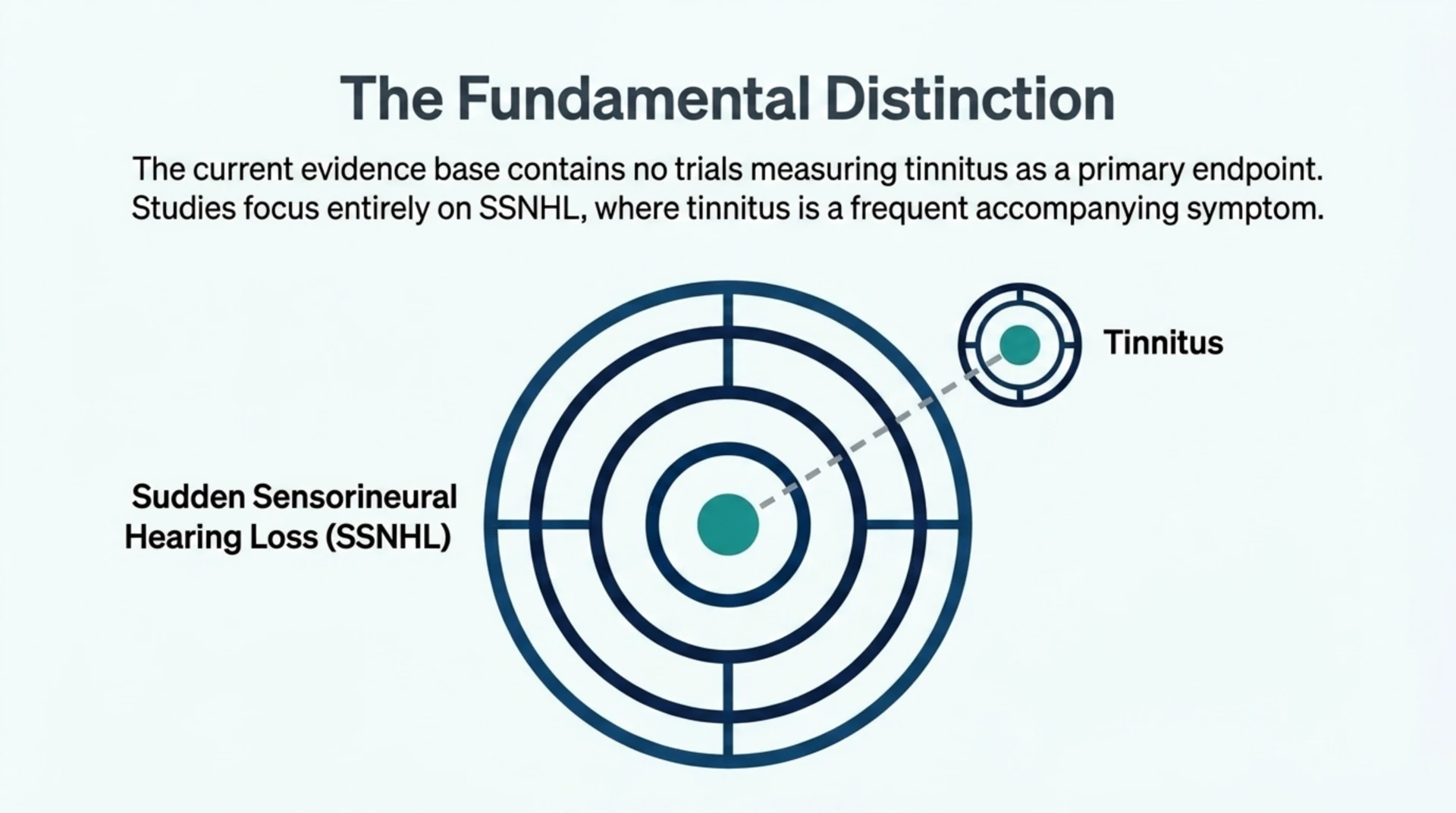
Based on the current pool of research, there is no trial here that measures tinnitus severity or tinnitus-specific outcomes as its primary endpoint. Tinnitus is mentioned in this literature mainly as a symptom that can accompany SSNHL, not as the thing being treated and measured. Any statement that HBOT is proven to treat tinnitus directly would be overreaching what this evidence actually supports. What we can responsibly discuss is the SSNHL literature, where tinnitus commonly co-occurs, and what that literature says about hearing recovery when HBOT is added to standard care.
What Does the Sudden Sensorineural Hearing Loss Evidence Actually Show?
The picture across these studies is inconsistent, and that inconsistency is itself the most useful, honest finding.
Larger observational studies have found no significant added benefit
A 2026 prospective, multicentre observational study across several tertiary care hospitals (PubMed | Our Assessment) examined whether adding HBOT to conventional treatment benefited patients with idiopathic SSNHL. The researchers reported that the difference between groups did not reach statistical significance. In plain terms, this particular study did not find clear evidence of added benefit from HBOT in its patient population.
Study design changes the answer, sometimes dramatically
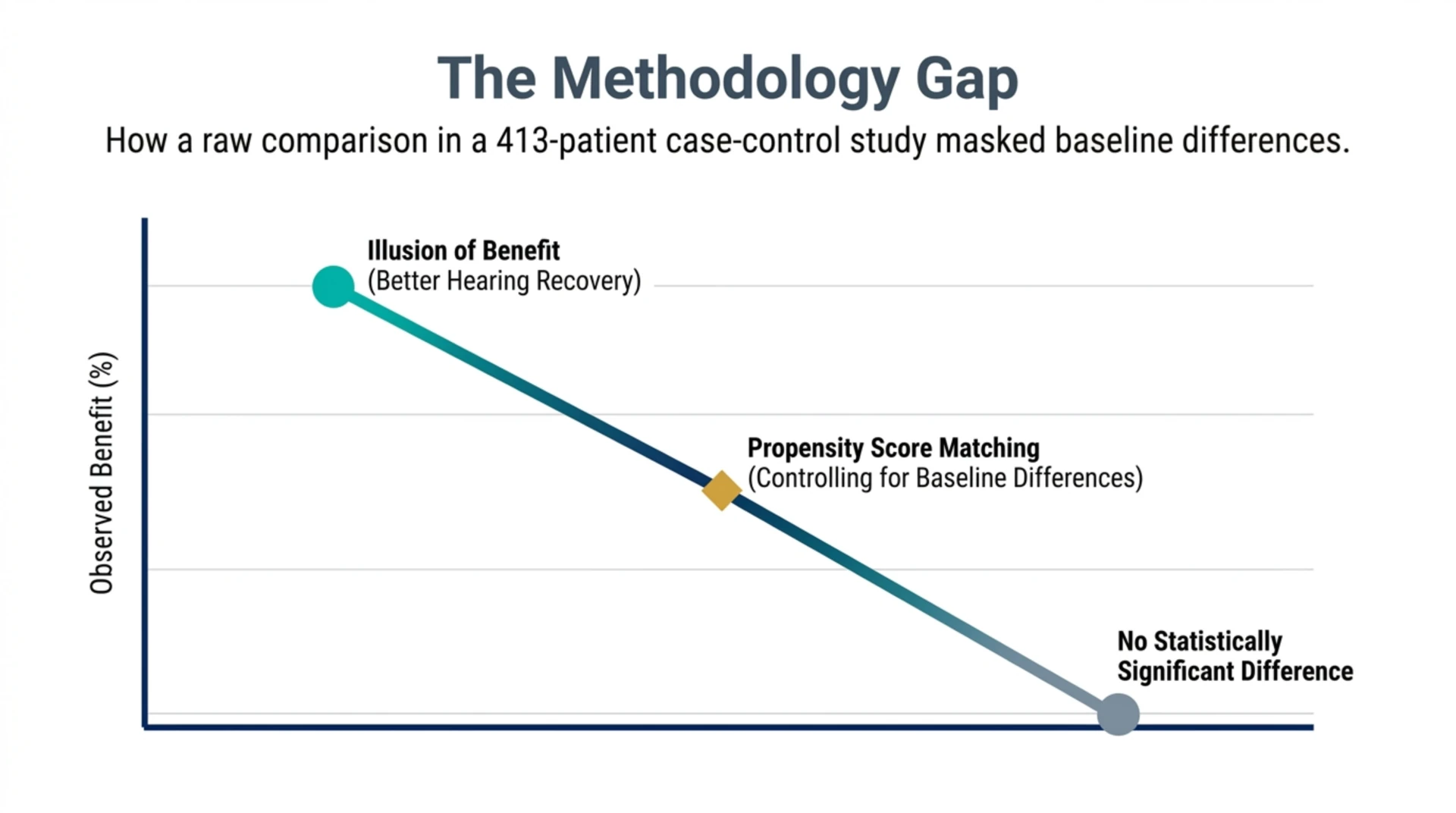
A propensity score matched case-control study of 413 patients (PubMed | Our Assessment) illustrates exactly why methodology matters here. Before the researchers adjusted for baseline differences between the HBOT and non-HBOT groups, patients who received HBOT as an initial treatment appeared to have significantly better hearing recovery. Once propensity score matching controlled for those baseline differences, the difference in overall hearing recovery was **no longer statistically significant**. That gap between the unadjusted and adjusted results is a textbook example of how a raw comparison can be misleading if the two groups were not similar to begin with.
Systematic reviews exist precisely because single studies disagree
A 2026 systematic review and meta-analysis pooling 20 studies and 1,687 patients (PubMed | Our Assessment) was built specifically to make sense of this kind of inconsistency, pooling the accumulated literature on whether HBOT changes hearing recovery odds in SSNHL rather than relying on any single centre’s experience. A separate meta-analysis restricted to 14 randomised controlled trials and 794 participants (PubMed | Our Assessment) narrowed the question further, focusing only on randomised evidence for HBOT used as an adjunct to corticosteroids rather than as a stand-alone treatment. The existence of these two pooled reviews confirms that the underlying single studies are heterogeneous enough that no individual trial should be read as the final word.
Adjunctive use with steroids has some supportive retrospective data
A retrospective analysis (PubMed | Our Assessment) reported that combining HBOT with systemic steroid therapy was associated with additional improvement in hearing outcomes compared with steroids alone, consistent with the adjunctive-therapy hypothesis this literature keeps testing. Because this was a retrospective, non-randomised comparison, “associated with” is the accurate way to describe it. It cannot be read as proof that HBOT caused the extra improvement.
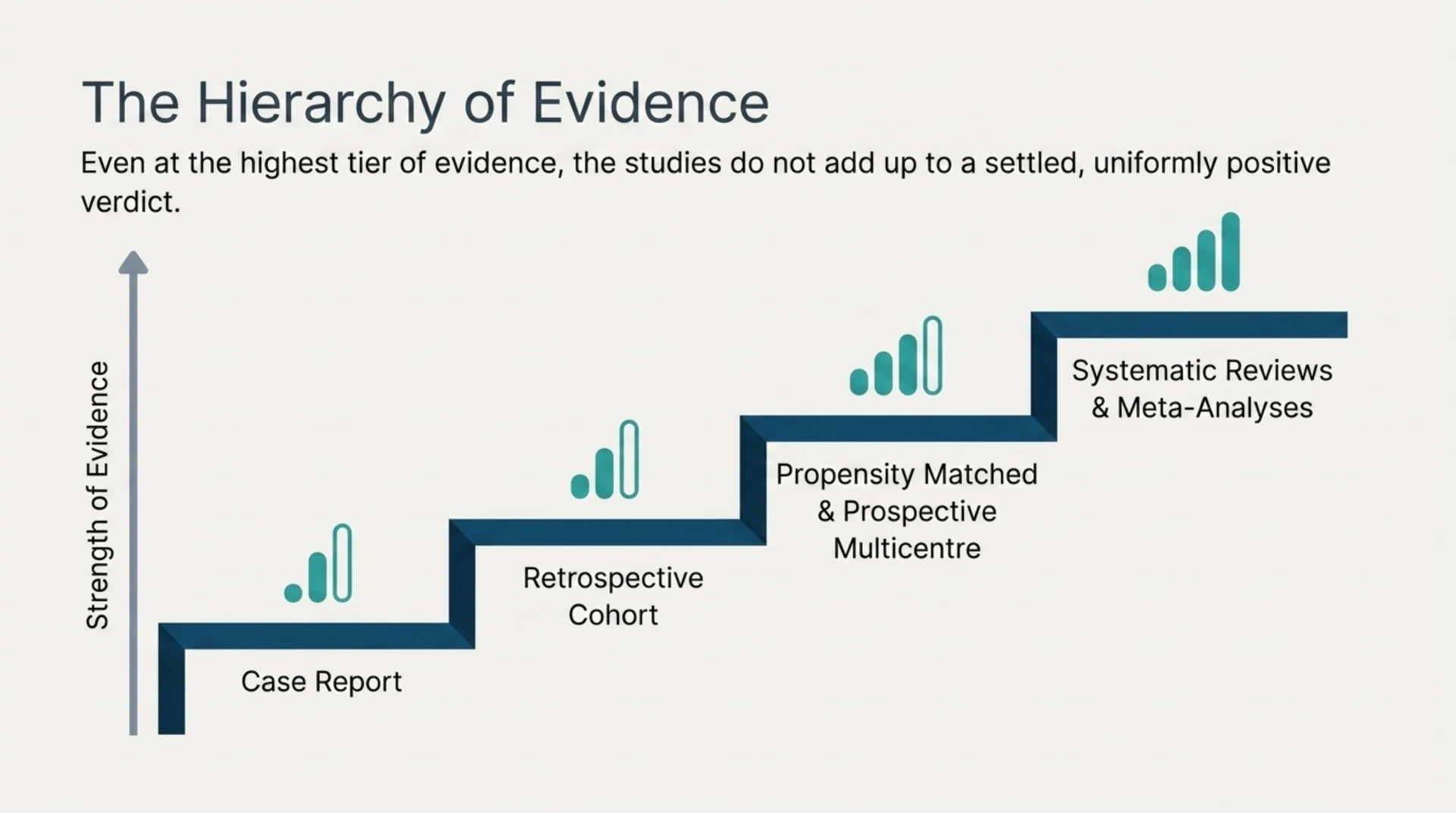
How Do These Studies Compare in Strength of Evidence?
Not all study designs carry the same weight. The table below places the designs represented in this pool on a rough evidence hierarchy, from least to most able to support a cause and effect conclusion.
| Evidence Type | Example From This Pool | What It Can Tell Us | Relative Strength |
|---|---|---|---|
| Case report | HBOT for hearing loss after meningitis | What happened to one patient | Lowest, hypothesis generating only |
| Retrospective cohort | Timing of HBOT in idiopathic SSNHL (70 patients) | Patterns across a treated group, no control comparison | Low to moderate |
| Propensity matched case-control | HBOT as initial treatment (413 patients) | Outcomes adjusted for measured baseline differences | Moderate |
| Prospective multicentre observational | Role of HBOT in idiopathic SSNHL management | Real world outcomes across several hospitals | Moderate to high |
| Systematic review and meta-analysis | HBOT and SSNHL (20 studies, 1,687 patients) | Pooled signal across the existing literature | High |
| Meta-analysis of randomised trials | HBOT as adjunct to corticosteroids (14 RCTs) | Pooled results from randomised comparisons | Highest achievable from this evidence base |
Even at the top of this hierarchy, the studies in this pool do not add up to a settled, uniformly positive verdict. They add up to a field that keeps testing the question because earlier answers were not consistent enough to close it.
Does the Timing of Treatment Matter?
A retrospective cohort study of 70 patients with idiopathic SSNHL (PubMed | Our Assessment) evaluated how the timing of HBOT initiation related to treatment success. Timing is a recurring theme across this body of research: clinicians in this field generally operate on the assumption that earlier intervention gives any adjunct treatment, HBOT included, a better chance of mattering, though the exact window and its effect size are still being worked out study by study rather than settled by one definitive trial.
What About Case Reports Involving Specific Causes of Hearing Loss?
Several entries in this pool are single-patient case reports, and they deserve to be read as exactly that. A case report described a 57-year-old woman who received HBOT for severe hearing loss caused by Streptococcus pneumoniae meningitis (PubMed | Our Assessment), with the authors noting improvement after treatment began. Another case report followed a 74-year-old man who developed sudden hearing loss after a stroke and was treated with HBOT (PubMed | Our Assessment), also with a reported improvement in hearing. Case reports like these cannot establish that HBOT caused the recovery, and they cannot predict how it would perform across a broader population. They document what happened in one patient, nothing more, and they are useful mainly for generating questions that larger, controlled studies then have to answer.
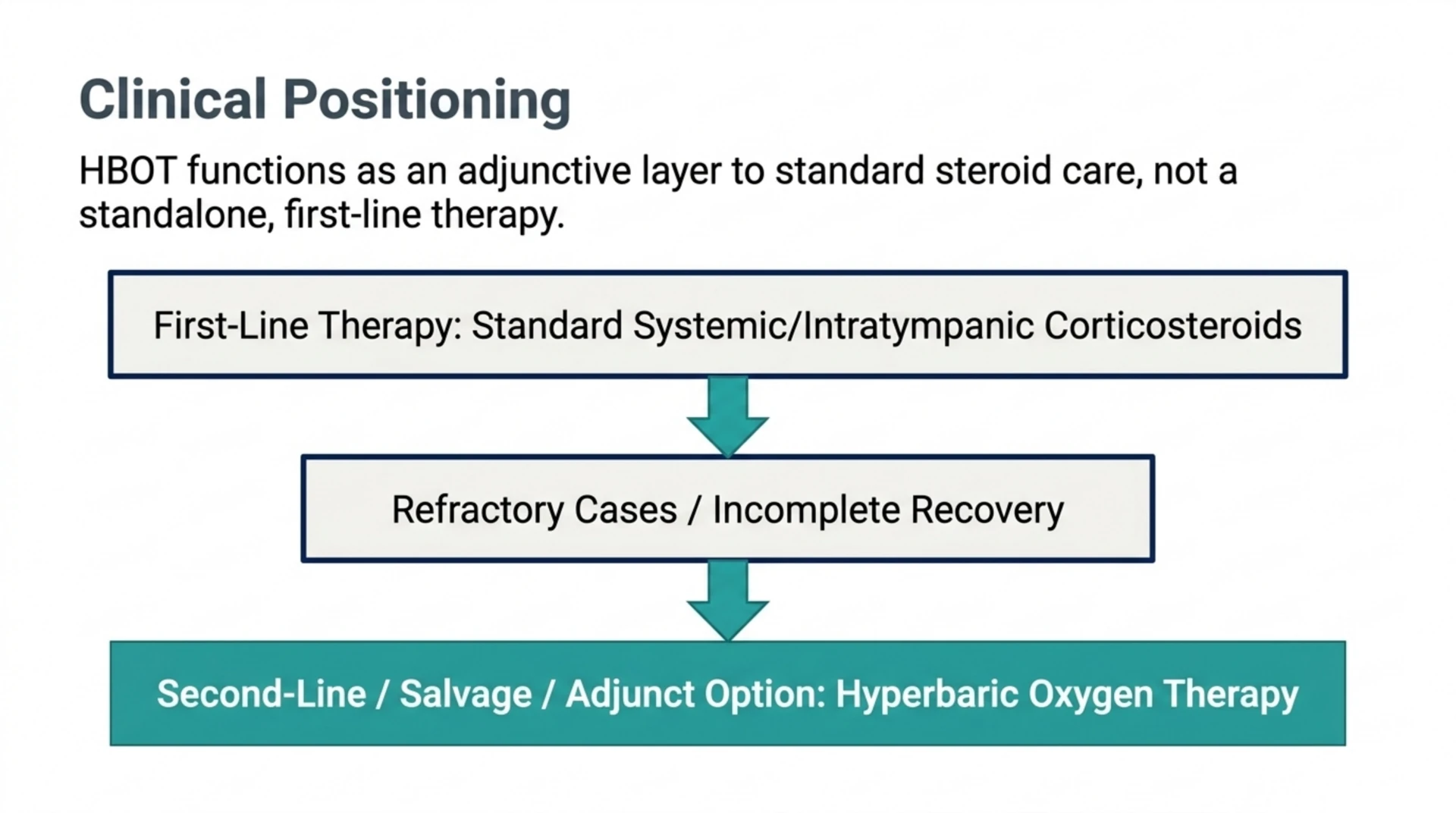
Where Does HBOT Sit Among Other Treatment Options for Refractory Cases?
A systematic review and network meta-analysis comparing five salvage therapies for refractory SSNHL (PubMed | Our Assessment) situated HBOT among the second-line options considered when initial steroid treatment has not worked. That framing is consistent with how HBOT tends to be positioned in this field generally: as an adjunct or salvage option layered onto standard steroid care, rather than a stand-alone, first-line therapy for sudden hearing loss or the tinnitus that can come with it.
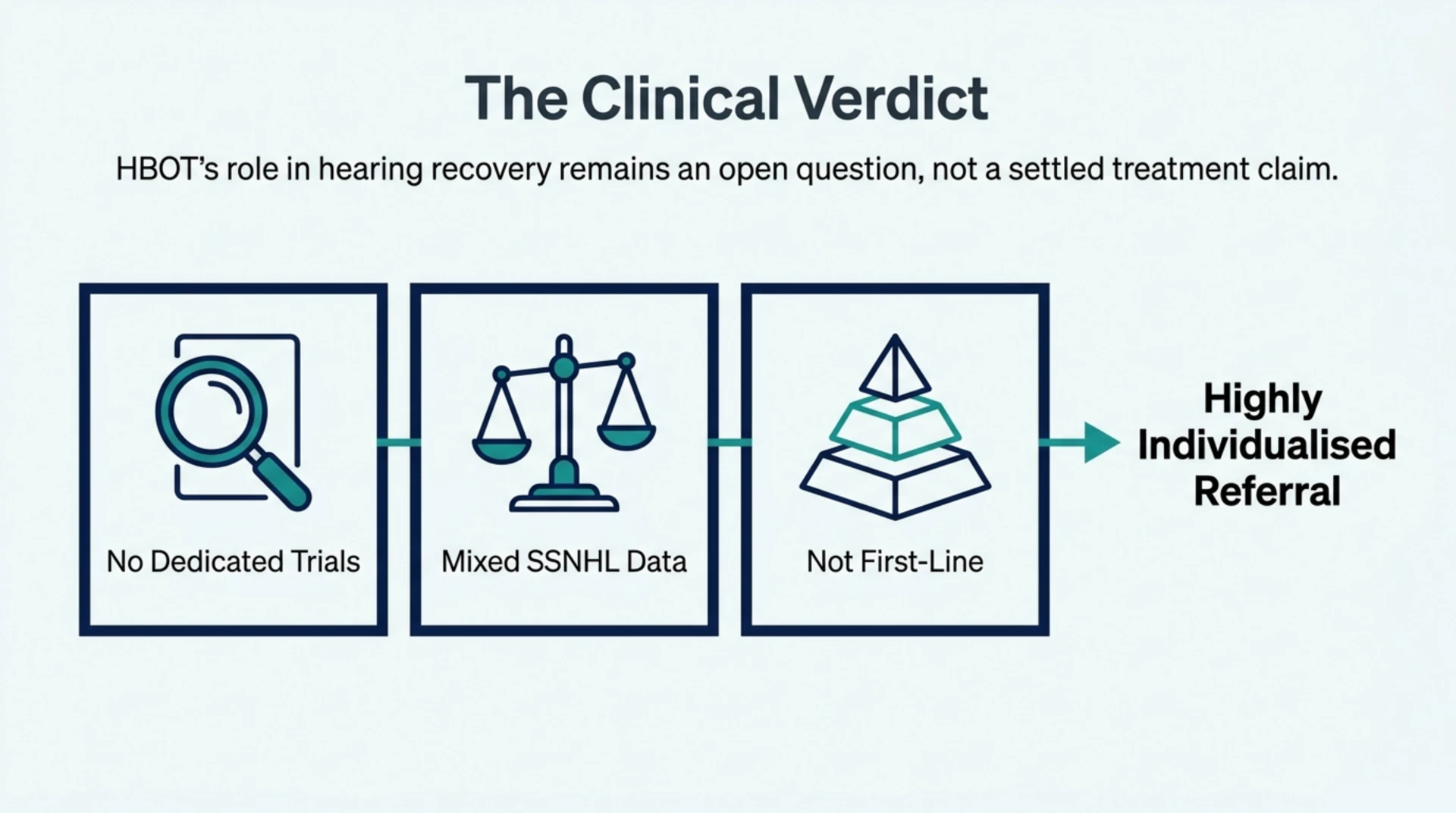
What Should Referring Physicians Take Away From This Evidence?
Three things stand out. First, there are no tinnitus-specific trials in this evidence base, so any counselling about HBOT and tinnitus should be framed through the SSNHL literature, with that limitation stated plainly to the patient. Second, the SSNHL findings themselves are mixed: several studies, including a matched case-control analysis and a prospective multicentre study, found no statistically significant benefit once appropriate controls were applied, while other retrospective analyses reported an association with improved recovery. Third, patient selection and timing appear to matter more than any single average effect size, which is why individualized referral decisions, rather than blanket protocols, are the appropriate response to evidence at this stage of maturity.
At Canada Hyperbarics, our research library tracks over 14,000 peer-reviewed studies across HBOT’s approved and investigational uses, and sudden sensorineural hearing loss is one of the areas where the literature is still actively evolving rather than settled. Canada Hyperbarics exists to help physicians and patients see that evidence as it actually stands, not as marketing copy would prefer it to read.
Frequently Asked Questions
Does hyperbaric oxygen therapy cure tinnitus?
No trial in the current evidence base measures tinnitus as a primary outcome, so there is no basis to call HBOT a cure for tinnitus. The available research studies sudden sensorineural hearing loss, a condition tinnitus often accompanies, and even that research is mixed.
What condition does most of the HBOT and hearing research actually study?
Sudden sensorineural hearing loss, commonly abbreviated SSNHL. It is an idiopathic or occasionally identifiable sudden drop in hearing, usually in one ear, and tinnitus is a frequent accompanying symptom rather than the condition being directly treated in these trials.
Is HBOT proven to restore hearing in SSNHL?
Not conclusively. Some retrospective studies report an association between HBOT and better recovery, but at least one prospective multicentre study and one propensity matched analysis in this pool found no statistically significant benefit once confounding factors were controlled for.
Does the timing of treatment after hearing loss onset matter?
Researchers in this field generally believe earlier intervention gives adjunct treatments a better chance to help, and a retrospective cohort study specifically examined this relationship, but the exact optimal window has not been settled by a single definitive trial.
Is HBOT used alone or alongside other treatments for sudden hearing loss?
In this literature, HBOT is almost always studied as an adjunct to systemic or intratympanic steroid therapy, or as a salvage option when initial steroid treatment fails, rather than as a stand-alone first-line treatment.
Should a physician refer a tinnitus patient for HBOT based on this evidence?
That decision should be individualized. Given the mixed results in the underlying SSNHL literature and the absence of tinnitus-specific trials, a referral conversation should set realistic expectations and treat HBOT as one option among several being investigated, not an established cure.
Related Reading
- HBOT Indications in Canada: A 2026 Referral Guide to the Health Canada and UHMS Lists for Physicians
- Which HBOT Service Lines Have the Strongest 2026 Evidence? An Industry Briefing for Canadian Clinic Owners
- Hyperbaric Clinic Accreditation Pathways in Canada
Physicians considering a referral for a patient with sudden hearing loss or persistent tinnitus can find hospitals and regulated facilities offering supervised hyperbaric oxygen therapy at our facilities directory.
This content is for informational purposes only and is not medical advice.