
TL;DR: Hyperbaric oxygen therapy (HBOT) is a treatment that involves breathing pure oxygen inside a pressurized chamber, and it is used to help radiation-damaged tissue regrow blood vessels. There is no study in this evidence pool that directly enrolled patients with radiation proctitis. The strongest available evidence comes from closely related late radiation tissue injuries, chiefly radiation cystitis of the bladder, plus broader reviews of hyperbaric oxygen for chronic radiotherapy side effects. This post reviews that evidence honestly, including where it does and does not reach the rectum.
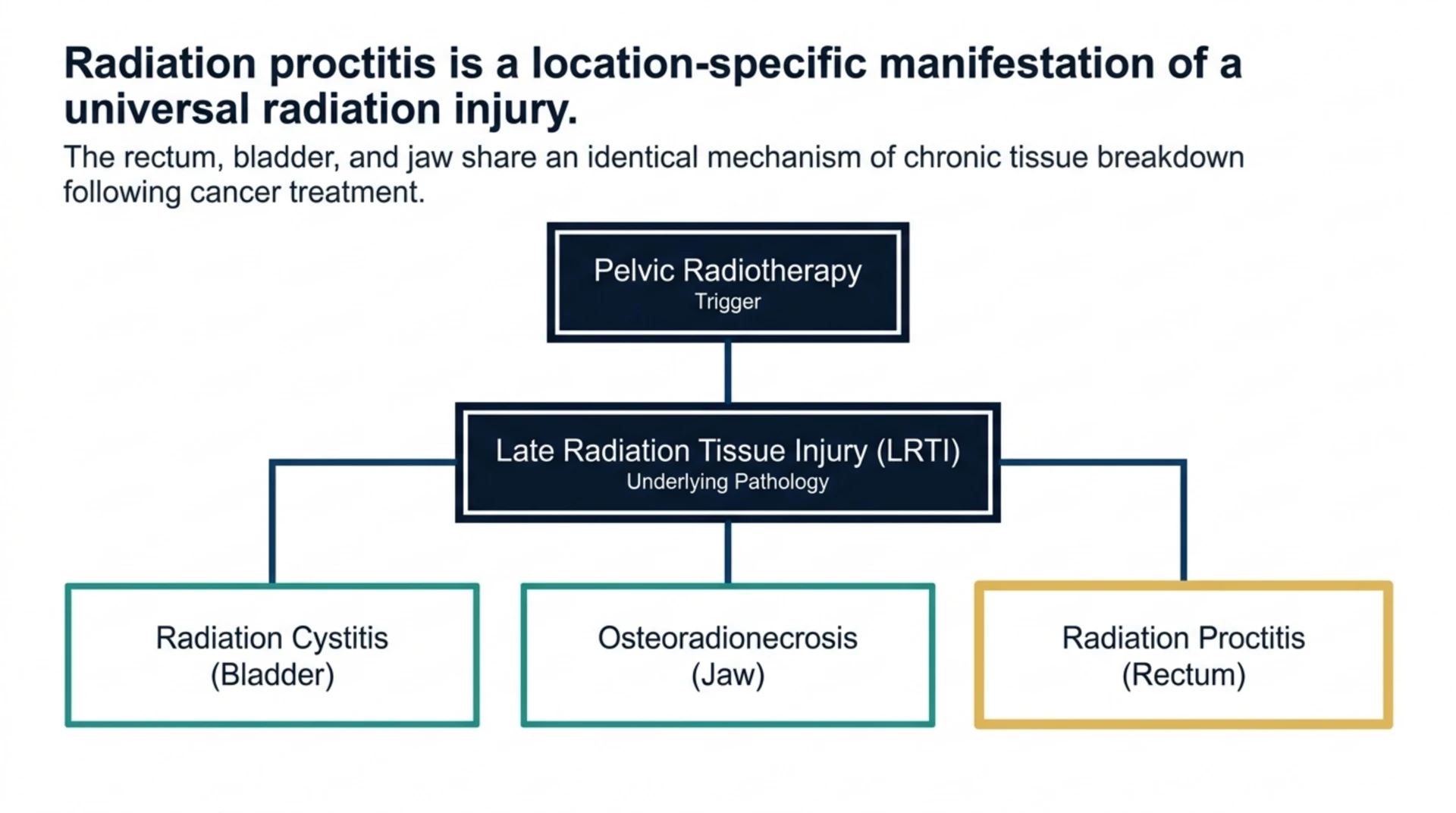
Hyperbaric oxygen therapy for radiation proctitis refers to the use of pressurized oxygen chambers to treat chronic rectal injury caused by prior pelvic radiotherapy. Radiation proctitis is a form of late radiation tissue injury (LRTI), a category that also includes radiation cystitis of the bladder and osteoradionecrosis of the jaw. Researchers investigating hyperbaric oxygen therapy for radiation proctitis are, in effect, asking whether a treatment that works for one type of radiation-damaged tissue also works for another.
That question matters because dedicated trials of HBOT specifically in radiation proctitis are scarce, and this evidence pool does not contain one. What it does contain is a cluster of studies on other pelvic and soft tissue radiation injuries, plus two broad reviews of HBOT across radiotherapy side effects generally. Taken together, they let us map out what is known, what is inferred by analogy, and what remains an open question for the rectum specifically.
What Is Radiation Proctitis?
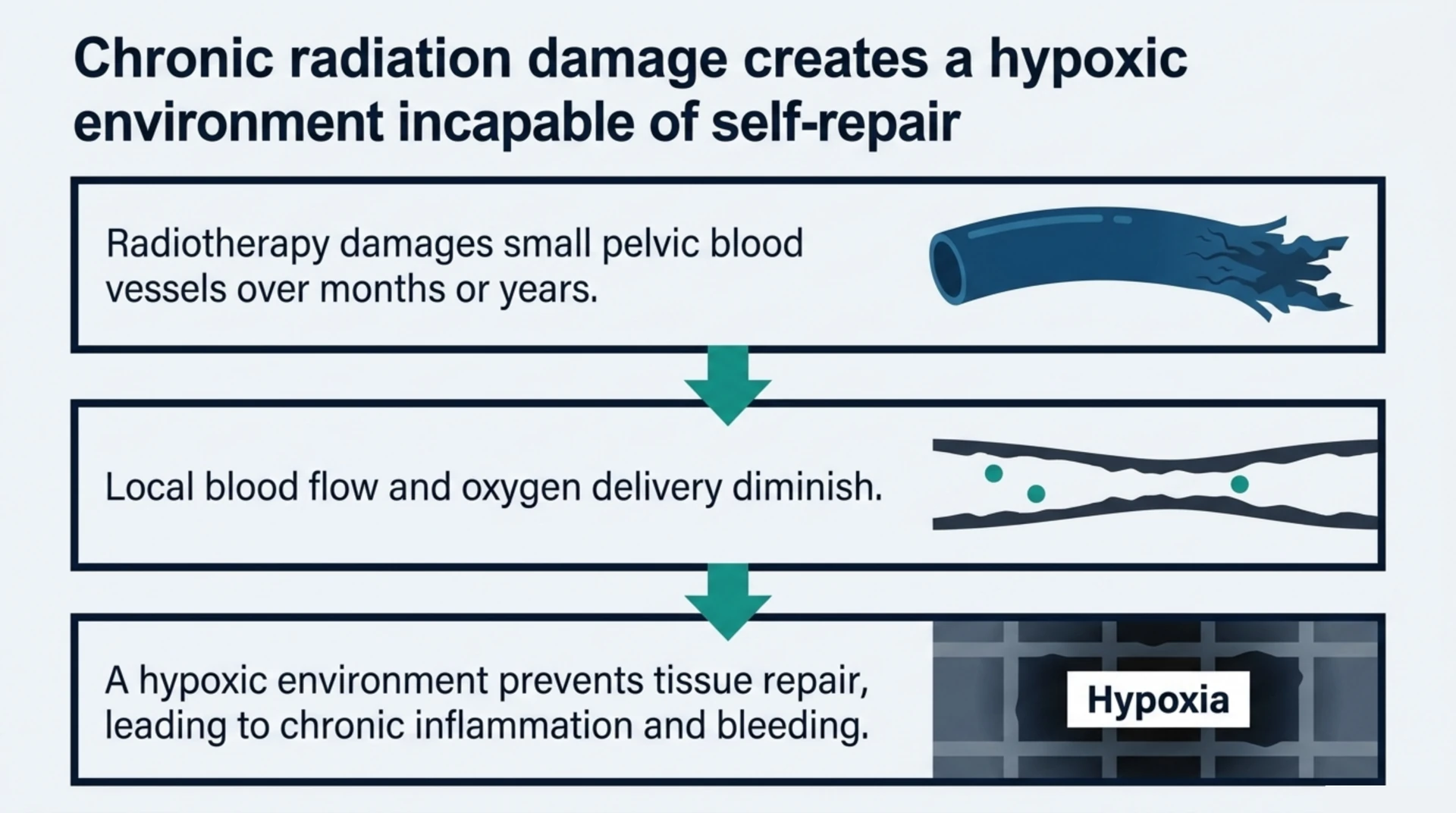
Radiation proctitis is inflammation and tissue damage in the rectum following radiotherapy for cancers of the pelvis, such as prostate, cervical, or rectal cancer. In its chronic form, it can present months to years after treatment as rectal bleeding, urgency, pain, or narrowing of the rectal wall. The underlying mechanism is thought to involve damage to small blood vessels, reducing local blood flow and oxygen delivery, which impairs the tissue’s ability to heal.
Does Hyperbaric Oxygen Therapy Treat Radiation Proctitis? What the Evidence Base Actually Contains
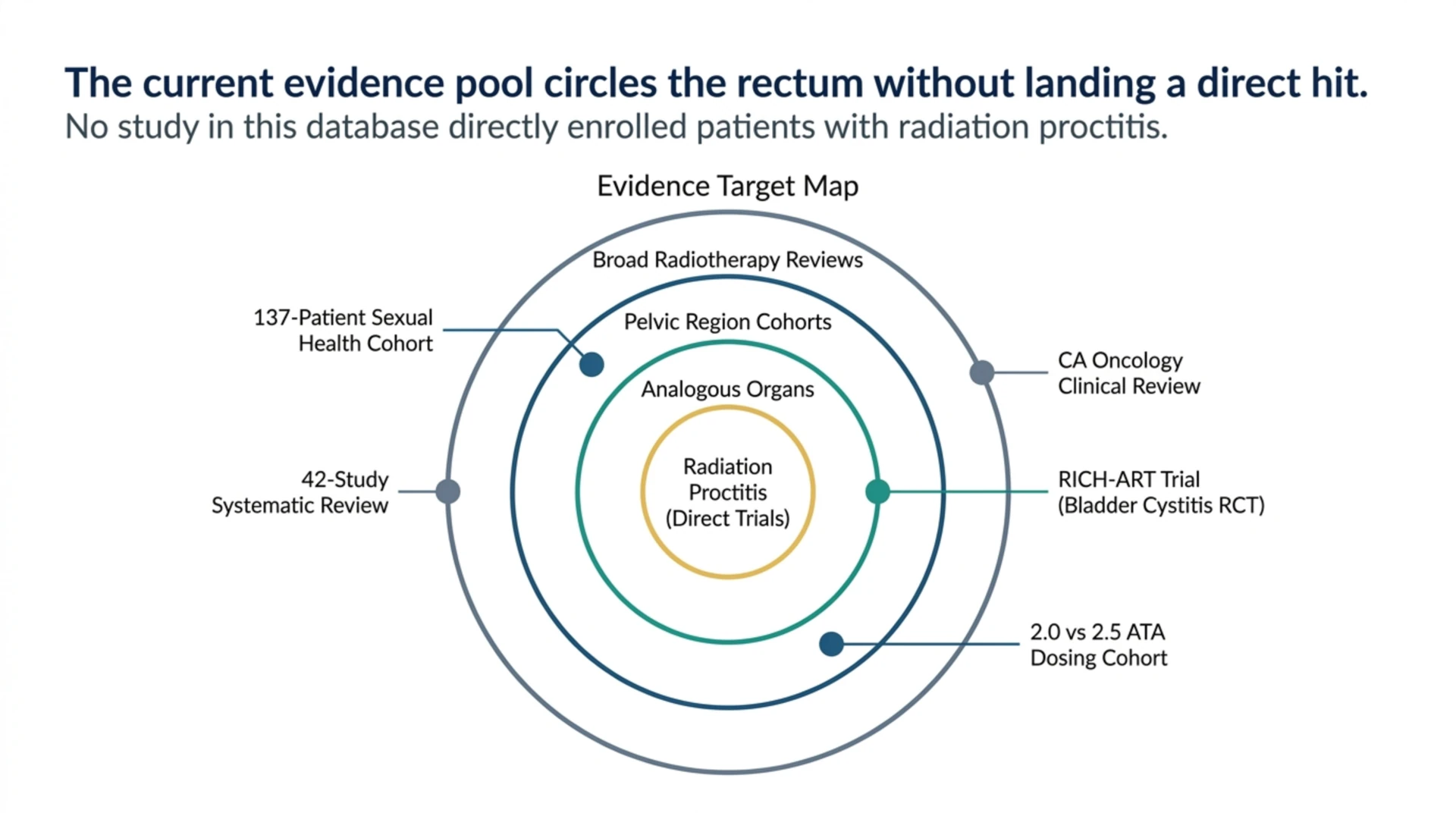
Directly, no study in this pool enrolled a proctitis population. The available research instead clusters around three closely related areas: radiation cystitis of the bladder, sexual health outcomes in pelvic cancer survivors with radiation injuries broadly defined, and narrative reviews of HBOT for chronic radiotherapy-related adverse effects as a category. A review titled “Delayed Radiation Injuries (Soft Tissue and Bony Necrosis) and Potential for Future Research” (PubMed | Our Assessment) explored HBOT’s application to late radiation soft tissue injury generally and specifically flagged this type of injury, including gaps like proctitis, as an area needing further dedicated research rather than one already settled by trial data.
The honest answer is that HBOT for radiation proctitis is supported by biological plausibility and by evidence in analogous pelvic tissues, not by a dedicated proctitis trial in this pool. This is a common situation in a mechanistically-driven field like hyperbaric medicine, where the underlying rationale (restoring oxygen delivery to hypoxic, radiation-damaged tissue) is shared across organ sites even when trial coverage is not.
What Does the Randomised Evidence Show in a Related Radiation Injury?
The strongest single piece of evidence in this pool for any late radiation pelvic injury is the RICH-ART trial, a multicentre, open-label, randomised controlled phase 2-3 study with five-year follow-up (Van De Ven et al., PubMed | Our Assessment). This trial compared HBOT with standard care in patients with chronic radiation-induced cystitis, a bladder condition that shares the same underlying vascular injury mechanism as radiation proctitis. Over long-term follow-up, HBOT improved outcomes in chronic radiation cystitis compared with standard care alone.
This is genuinely useful evidence, but it is bladder evidence, not rectal evidence. **Its relevance to radiation proctitis is by mechanistic analogy, not by direct extension** of the trial’s results. Researchers should treat RICH-ART as proof that HBOT can benefit at least one form of pelvic late radiation tissue injury under randomised conditions, which strengthens the rationale for studying proctitis, without treating the cystitis result as if it were a proctitis result.
What Do the Broader Reviews of HBOT for Radiotherapy Side Effects Report?
Two reviews in this pool take a wide-angle view of HBOT across radiotherapy complications rather than a single organ.
A Systematic Review Across 42 Studies
“Between hope and uncertainty: the elusive evidence on hyperbaric oxygen therapy and radiotherapy” (PubMed | Our Assessment) systematically reviewed 42 studies covering 2,785 patients treated with HBOT for a range of radiotherapy side effects between 2000 and 2025. Its title captures the state of this literature well: encouraging signals exist across several radiation injury types, but the review describes the overall evidence base as uneven in quality and scope. This kind of review is valuable precisely because it does not pretend the evidence is stronger or more uniform than it is.
A Clinically Focused Review in a Major Oncology Journal
“Hyperbaric oxygen therapy for chronic radiotherapy-related adverse effects: A clinically focused review” (PubMed | Our Assessment) critically evaluated the evidence for HBOT in managing chronic radiotherapy-related adverse effects as a category, published in a leading cancer journal. Reviews of this kind are useful for researchers because they synthesize evidence across the multiple organ systems affected by radiation, giving a sense of where the field’s confidence is strongest (generally osteoradionecrosis and radiation cystitis) and where it remains thinner, which includes the rectum.
What About the Pelvic Radiation Injury Population Itself?
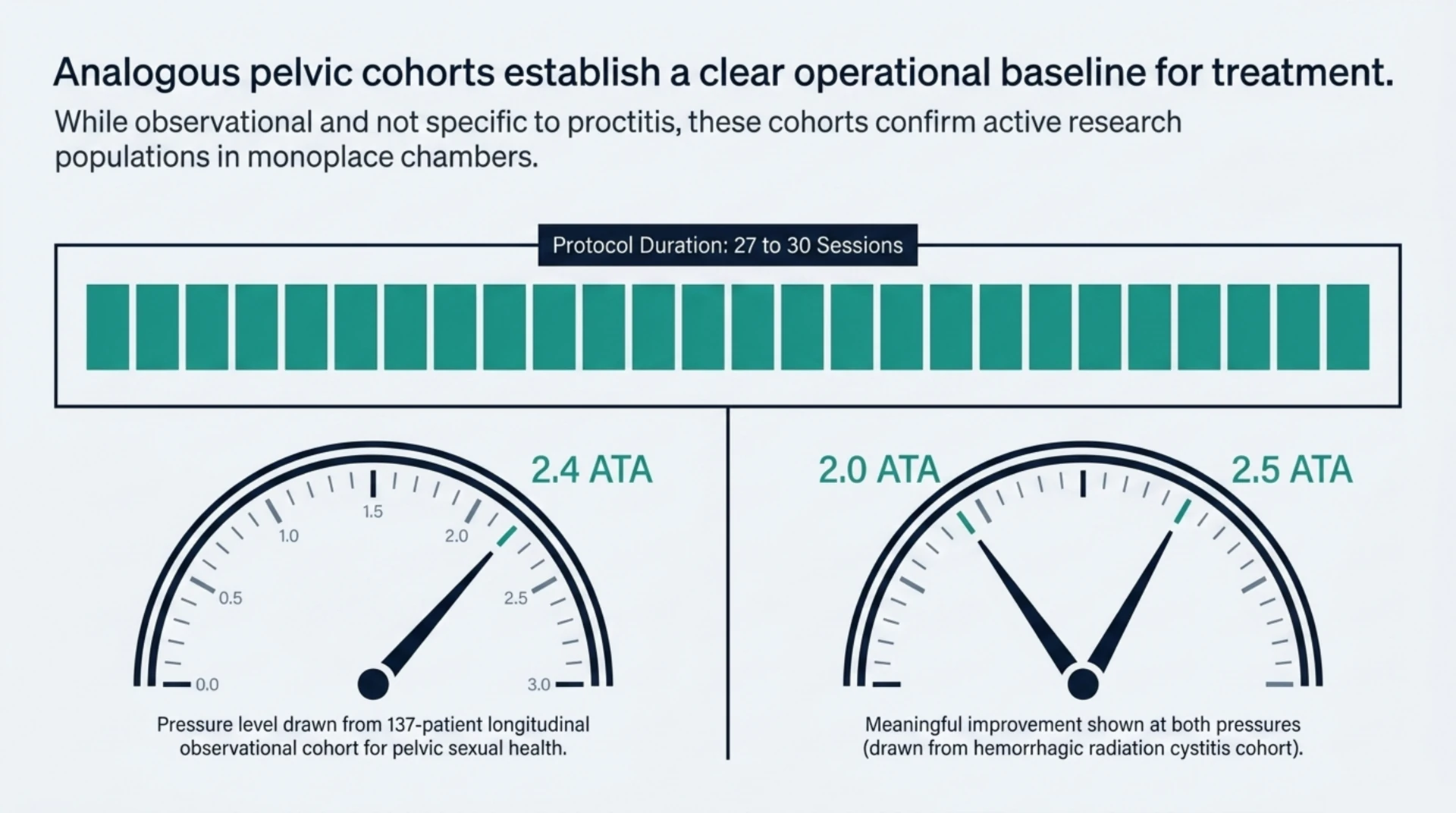
One study followed patients whose profile overlaps meaningfully with a proctitis population: a longitudinal observational study of sexual health outcomes in 137 pelvic cancer survivors with radiation injuries who received 27 to 30 hyperbaric oxygen treatments in monoplace chambers at 2.4 atmospheres absolute (PubMed | Our Assessment). Because this was an observational cohort rather than a controlled trial, changes in sexual health were associated with the treatment course rather than proven to be caused by it. The value of this study for a proctitis discussion is less about its specific outcome measure and more about confirming that pelvic radiation injury patients, broadly defined, are a population actively being studied with HBOT protocols similar to those used for other late radiation injuries.
A related review, “Radiotherapy effects on the lower urinary tract: A review of long-term complications and their management” (PubMed | Our Assessment), conducted a ten-year review of the MEDLINE and PubMed databases using PICO criteria to catalogue the incidence and management of late radiotherapy complications of the urinary tract. It is useful context for understanding how the management landscape for one class of pelvic late radiation injury has developed, and by extension what a comparable evidence base for proctitis might eventually need to look like.
How Might Hyperbaric Oxygen Help Radiation-Damaged Tissue?
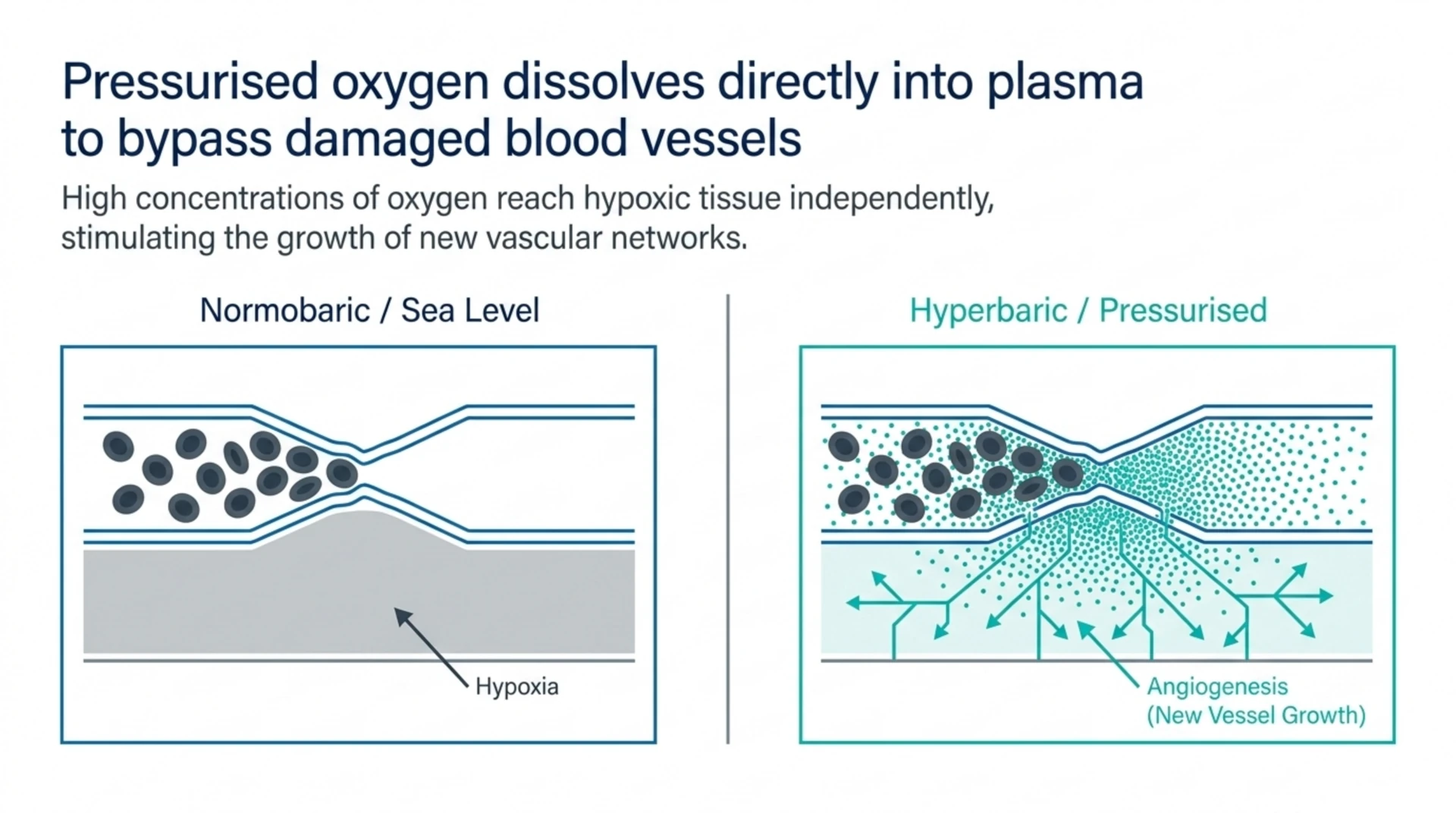
The proposed mechanism is consistent across every late radiation tissue injury studied in this pool, whether bladder, jaw bone, or soft tissue generally. Radiotherapy damages small blood vessels over time, reducing local blood flow and leaving tissue chronically short of oxygen. This hypoxic environment impairs the tissue’s ability to repair itself and fight infection. Breathing high concentrations of oxygen at increased atmospheric pressure raises the amount of oxygen dissolved directly in blood plasma, which can reach hypoxic tissue independent of damaged blood vessels. Over a course of treatments, this is thought to help stimulate new blood vessel growth in the affected area.
This mechanism is organ-agnostic in principle, which is why researchers extend hyperbaric oxygen therapy from one radiation injury site to another. **The mechanism being plausible for the rectum does not substitute for a rectum-specific trial**, and that gap is exactly what this evidence pool illustrates.
Comparing the Evidence Across Related Radiation Injuries
| Condition | Evidence Type in This Pool | Key Study | Strength for Proctitis Question |
|---|---|---|---|
| Chronic radiation cystitis (bladder) | Randomised controlled trial, 5-year follow-up | RICH-ART | Strong direct evidence for cystitis; analogy only for proctitis |
| Hemorrhagic radiation cystitis, dosing question | Cohort comparison of two pressures | 2.0 vs 2.5 ATA study | Informs protocol design by analogy, not proctitis-specific |
| Pelvic radiation injury, sexual health | Longitudinal observational study | 137-patient cohort | Confirms pelvic radiation injury is an active research population |
| Chronic radiotherapy adverse effects, all sites | Clinically focused narrative review | CA: A Cancer Journal for Clinicians review | Broad context, not proctitis-specific data |
| Radiotherapy side effects, multiple conditions | Systematic review, 42 studies | Between Hope and Uncertainty | Field-wide uncertainty acknowledged directly |
| Radiation proctitis specifically | No dedicated study identified in this pool | Not applicable | Evidence gap |
What Are the Limits of the Current Evidence for Radiation Proctitis?
Researchers should take three limitations seriously. First, none of the studies here enrolled a proctitis-specific population, so any application of these findings to the rectum is inferential. Second, several of the closest analogues, including the sexual health cohort, are observational rather than randomised, which limits causal conclusions even within their own study population. Third, the two broad reviews describe the overall HBOT-and-radiotherapy literature as heterogeneous in study quality, meaning that even where positive signals exist across organ sites, they are not uniformly strong evidence.
What this pool does support is a mechanistic and cross-organ rationale strong enough to justify continued research into radiation proctitis specifically, echoed directly by the review noting this gap as a target for future study. Canada Hyperbarics presents this kind of nuance deliberately: an evidence review is only useful to researchers if it distinguishes between what has been directly tested and what has merely been inferred.
Frequently Asked Questions
Is there a randomised controlled trial of HBOT for radiation proctitis?
Not in this evidence pool. The one randomised trial available, RICH-ART, studied chronic radiation cystitis of the bladder rather than the rectum.
Why would HBOT be considered for radiation proctitis if there is no direct trial?
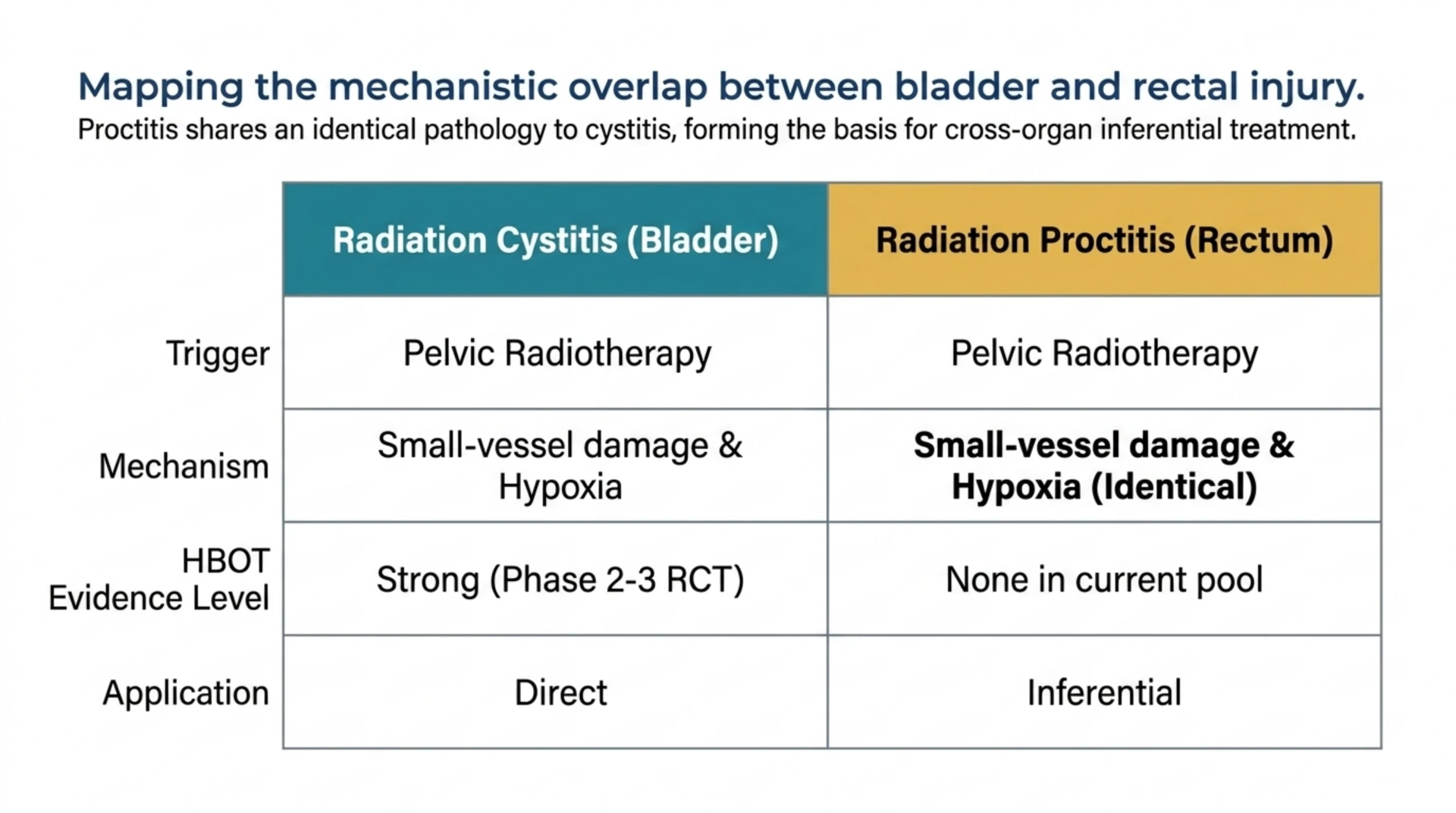
Because radiation proctitis shares the same underlying mechanism, chronic small-vessel damage and tissue hypoxia, as radiation cystitis and other late radiation tissue injuries where HBOT has shown benefit in this evidence pool.
What HBOT protocol has been studied in related radiation injuries?
In the sexual health cohort of pelvic cancer survivors, patients received 27 to 30 treatments in monoplace chambers at 2.4 atmospheres absolute. A separate cohort comparing 2.0 versus 2.5 atmospheres absolute for hemorrhagic radiation cystitis (PubMed | Our Assessment) found both pressures produced meaningful improvement, suggesting some flexibility in protocol design for pelvic late radiation injuries, though this was not tested in proctitis.
Is radiation proctitis the same as radiation cystitis?
No. They affect different organs, the rectum versus the bladder, but both arise from the same category of injury: late radiation tissue damage to small blood vessels following pelvic radiotherapy.
How confident should researchers be in HBOT for radiation proctitis based on current evidence?
Cautiously optimistic at most. The rationale is sound and supported by analogous pelvic organ data, but confidence should be calibrated to the absence of a dedicated proctitis trial, not to the strength of the cystitis evidence alone.
What would strengthen the evidence base for this specific indication?
A randomised controlled trial enrolling patients with chronic radiation proctitis specifically, following the design used in RICH-ART for radiation cystitis, is the clearest gap identified by the reviews in this pool.
Related Reading
- HBOT Indications in Canada: A 2026 Referral Guide to the Health Canada and UHMS Lists for Physicians
- Which HBOT Service Lines Have the Strongest 2026 Evidence? An Industry Briefing for Canadian Clinic Owners
- HBOT for Exceptional Blood Loss Anaemia
Researchers, referring physicians, and patients weighing hyperbaric oxygen for pelvic radiation injury should discuss individual circumstances with a qualified clinician. Canada Hyperbarics maintains this evidence review as an educational resource and encourages seeking treatment only through hospitals and regulated facilities; visit our facilities directory to find one near you.
This content is for informational purposes only and is not medical advice.